Did you know, you can still access recent national C0VID #wastewater data in the U.S.?
I'll walk you though it.
🧵
1/
I'll walk you though it.
🧵
1/

First, go to Verily's #wastewater website.
Click on the little Line Graph icon on the left side.
2/ data.wastewaterscan.org
Click on the little Line Graph icon on the left side.
2/ data.wastewaterscan.org

When you click on the Line Graph icon, it makes an annoying pop-up.
In the 1st menu, choose SARS-CoV-2.
In the 2nd menu, click *ANY* location. We want national, but they don't include it there. So pick anywhere, and we'll fix it later.
3/
In the 1st menu, choose SARS-CoV-2.
In the 2nd menu, click *ANY* location. We want national, but they don't include it there. So pick anywhere, and we'll fix it later.
3/

Click the "Get Started" button. Then you'll see something like this. It's the recent wastewater data at whatever rando site you selected.
Again, this is not what we want yet.
4/
Again, this is not what we want yet.
4/

Now, click to the right of the magnifying glass by "Location(s)" --> then "National" --> then "All Wastewater Sites"
5/
5/

The graph that will come up is overwhelming. No data synthesis. We're getting closer though.
Click the little crossed out eyeball I've circled in red.
6/
Click the little crossed out eyeball I've circled in red.
6/

Woo-hoo. We finally have a national average line. I can see why the CDC prefers this over Biobot. 🤣
Click a number on the vertical access and drag up or down (it moves opposite of how I expect). Play around with the start date too. See red circles.
7/
Click a number on the vertical access and drag up or down (it moves opposite of how I expect). Play around with the start date too. See red circles.
7/

I like to see either the entire pandemic (big picture) or the last 6-7 months (current wave, shown).
8/
8/

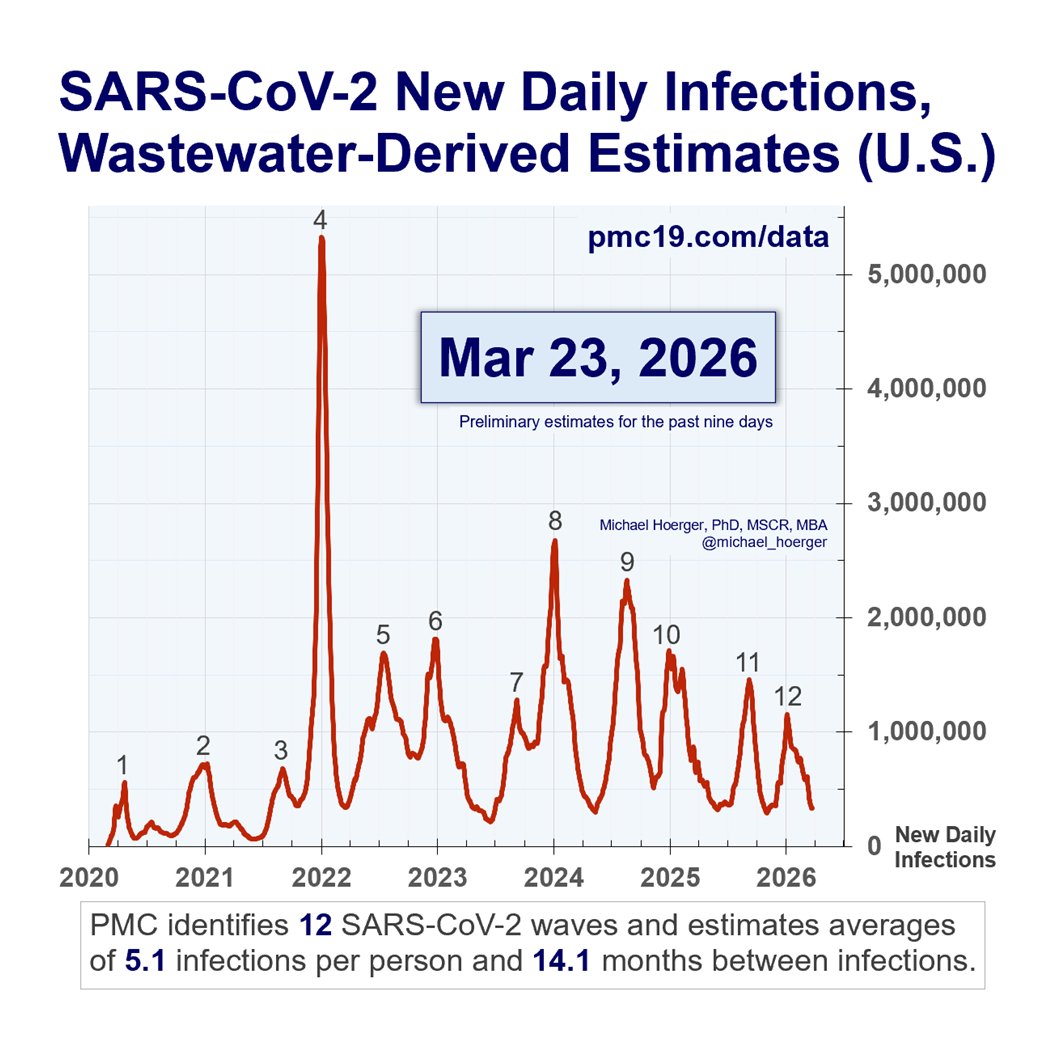
If you zoom out to see the entire pandemic, you'll find a similar picture relative to what you may have been tracking with Biobot, Walgreens, etc.
The waves show up. The estimates of magnitude vary by methodology.
9/
The waves show up. The estimates of magnitude vary by methodology.
9/
https://twitter.com/michael_hoerger/status/1711971052320870509
I hope to post an interim Biobot-to-Verily PMC forecast Monday.
I stand by prior forecasts. We'll reach the bottom of the current (very high) valley in 1-2 wks. Cases will pick up noticeably so around mid-November and get very very bad in Dec/Jan.
10/
I stand by prior forecasts. We'll reach the bottom of the current (very high) valley in 1-2 wks. Cases will pick up noticeably so around mid-November and get very very bad in Dec/Jan.
10/
https://twitter.com/michael_hoerger/status/1708945426261385476
Point of clarification: Verily data are included in this dashboard, but others have noted Verily does not own the dashboard. The language on their website is ambiguous in this regard, IMO (pic below). It's the first link on Verily's page.
Others report that as CDC Biobot sites come on, they will be included in a Verily-specific dashboard, independent of that above. It seems that rather than harmonizing and unifying data, we are at risk of proliferating more and potentially lower quality dashboards.
11/
Others report that as CDC Biobot sites come on, they will be included in a Verily-specific dashboard, independent of that above. It seems that rather than harmonizing and unifying data, we are at risk of proliferating more and potentially lower quality dashboards.
11/

• • •
Missing some Tweet in this thread? You can try to
force a refresh