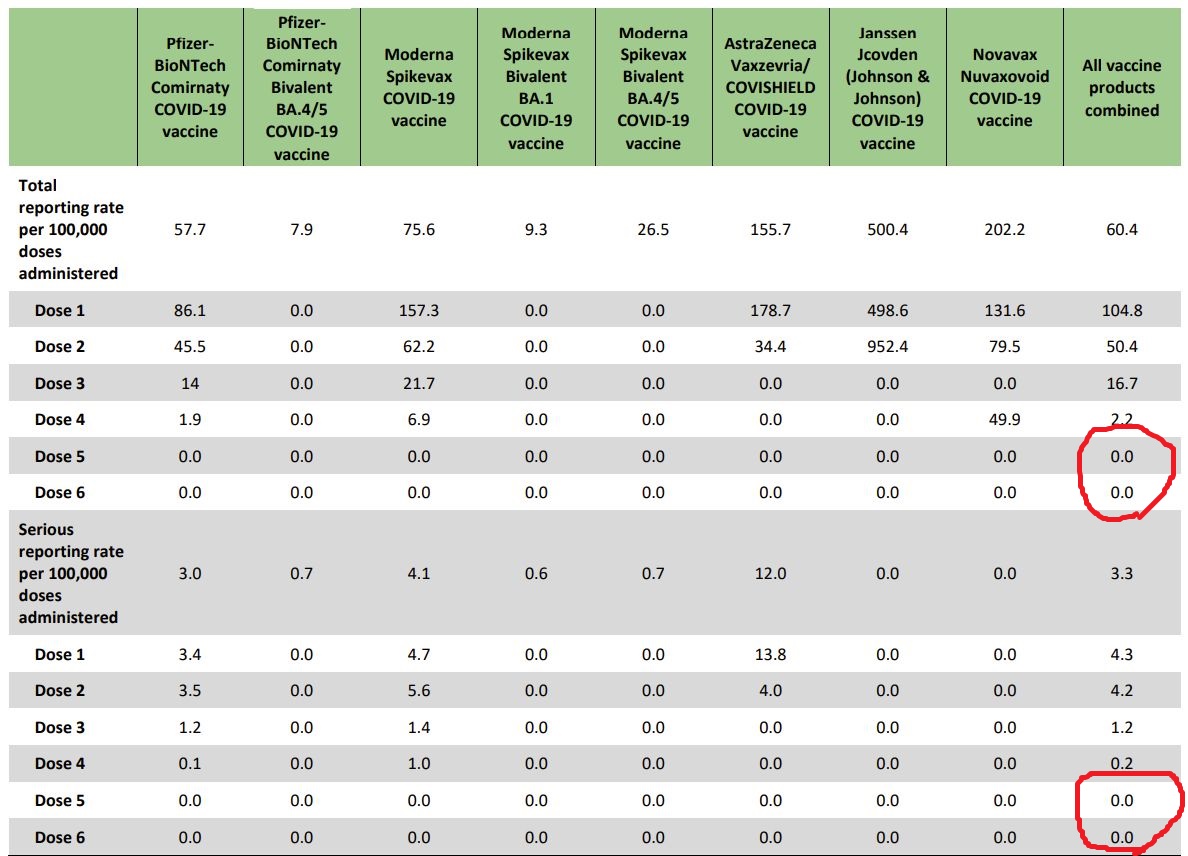
Some people going on vaguely about the "risk/benefit" analysis of a COVID booster. This is actual Ontario surveillance data of COVID vaccine adverse event reporting. Risk of boosters is practically nonexistent.
publichealthontario.ca/-/media/Docume…

publichealthontario.ca/-/media/Docume…
• • •
Missing some Tweet in this thread? You can try to
force a refresh