
1/The medulla is anything but DULL!
Does seeing an infarct in the medulla cause your heart to skip a beat?
Does medullary anatomy send you into respiratory arrest?
Never fear, here is a thread on the major medullary syndromes!
Does seeing an infarct in the medulla cause your heart to skip a beat?
Does medullary anatomy send you into respiratory arrest?
Never fear, here is a thread on the major medullary syndromes!

2/The medulla is like a toll booth.
Everything going down into the cord must pass through the medulla & everything from the cord going back up to the brain must too.
That’s a lot of tracts for a very small territory. Luckily you don’t need to know every tract
Everything going down into the cord must pass through the medulla & everything from the cord going back up to the brain must too.
That’s a lot of tracts for a very small territory. Luckily you don’t need to know every tract

3/Medulla has 4 main vascular territories, spread out like a fan:
Anteromedial, anterolateral, lateral, and posterior.
You don’t need to remember their names, just the territory they cover—and I’ll show you how
Anteromedial, anterolateral, lateral, and posterior.
You don’t need to remember their names, just the territory they cover—and I’ll show you how

4/The anterior territory is fed by the anterior spinal artery.
As a result, you can commonly get bilateral anteromedial infarcts as a result of the fact that the anterior spinal artery is unpaired.
As a result, you can commonly get bilateral anteromedial infarcts as a result of the fact that the anterior spinal artery is unpaired.

5/This results in a classic appearance for a medial medullary infarct.
Some say it looks like ear buds, while others say it looks like a heart.
But if you see either—that’s a medial medullary infarct
Some say it looks like ear buds, while others say it looks like a heart.
But if you see either—that’s a medial medullary infarct

6/Anterolateral territory has more variable anatomy—being fed by a combination of feeders from the anterior spinal artery, vertebral perforators, and branches of the PICA.
Different articles will say different vessels are dominant—which means NONE of them really are.
Different articles will say different vessels are dominant—which means NONE of them really are.
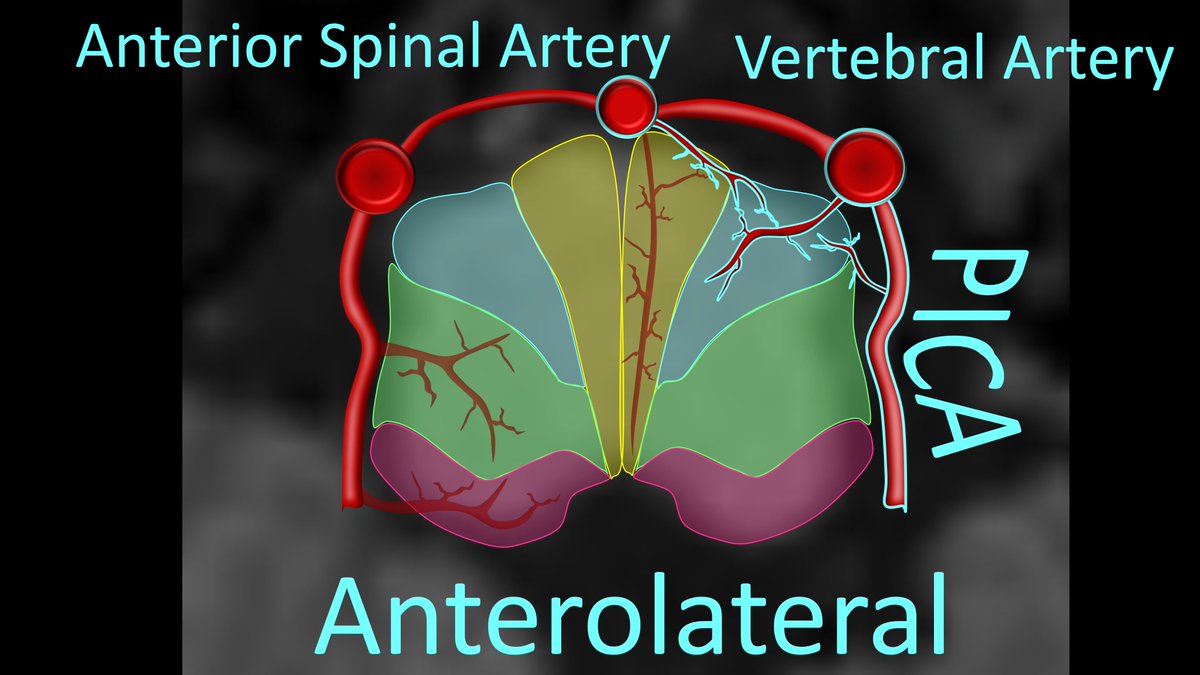
7/Because it is fed by combinations of different vessels, it is relatively uncommon to see isolated infarcts in this territory because the different vessels can collateralize for each other

8/Finally, both the lateral and posterior territories are both fed by branches of the PICA.
So if there is a PICA infarct, they go out together
So if there is a PICA infarct, they go out together
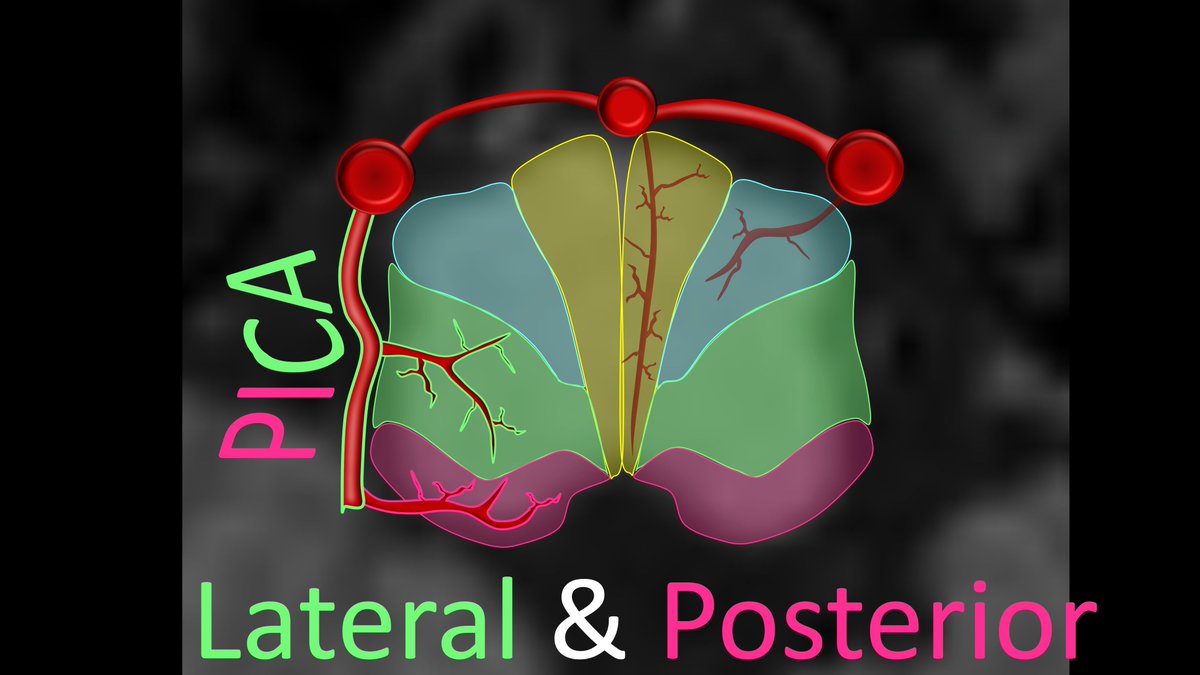
9/Infarcts of both of these territories give us what I call the classic “bruised cheek” appearance of the medulla
It looks like the little chubby cheek of the medulla has been in hit with lateral/posterior PICA medullary infarcts. (often just called lateral medullary infarcts)
It looks like the little chubby cheek of the medulla has been in hit with lateral/posterior PICA medullary infarcts. (often just called lateral medullary infarcts)

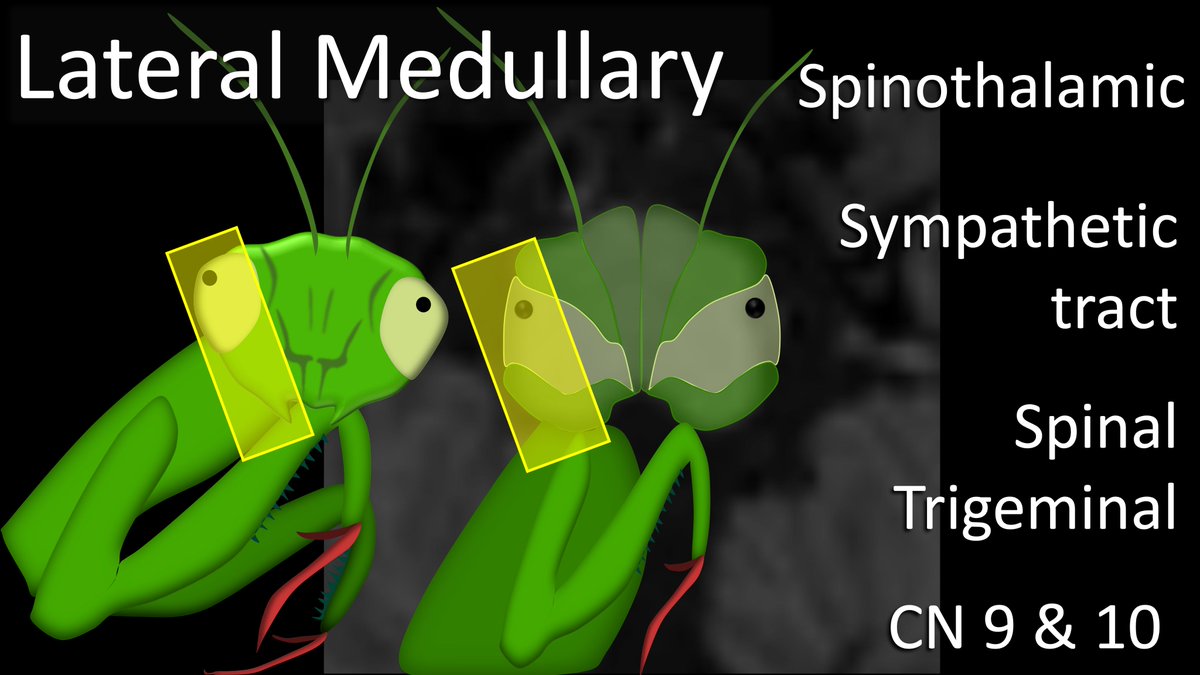
10/I think the vascular territories of the medulla look like a praying mantis face
The antennae is hypoglossal nerve that comes out it the “head” here.
This face will help you remember the medullary syndromes associated with medial & lateral medullary infarcts.
The antennae is hypoglossal nerve that comes out it the “head” here.
This face will help you remember the medullary syndromes associated with medial & lateral medullary infarcts.

11/So what are the main deficits associated with medial medullary infarcts?
Well, it will hit the pyramids (weakness)
It will affect the medial lemniscus (sensory)
And the exiting hypoglossal nerves
Well, it will hit the pyramids (weakness)
It will affect the medial lemniscus (sensory)
And the exiting hypoglossal nerves

12/So let’s look at what happens if we take out the medial part of our praying mantis:
You take out the antennae which are medial (hypoglossal)
And you take out the little arms that are always medial under his chin (so motor) as well as their little feelers (sensory).
You take out the antennae which are medial (hypoglossal)
And you take out the little arms that are always medial under his chin (so motor) as well as their little feelers (sensory).

13/Now let’s talk lateral medullary syndrome. It takes out both the lateral & posterior territories supplied by the PICA
It is complex, but the main tracts involved are the spinothalamic, sympathetic tracts, spinal trigeminal, and CN 9 & 10.
How to remember these?
It is complex, but the main tracts involved are the spinothalamic, sympathetic tracts, spinal trigeminal, and CN 9 & 10.
How to remember these?
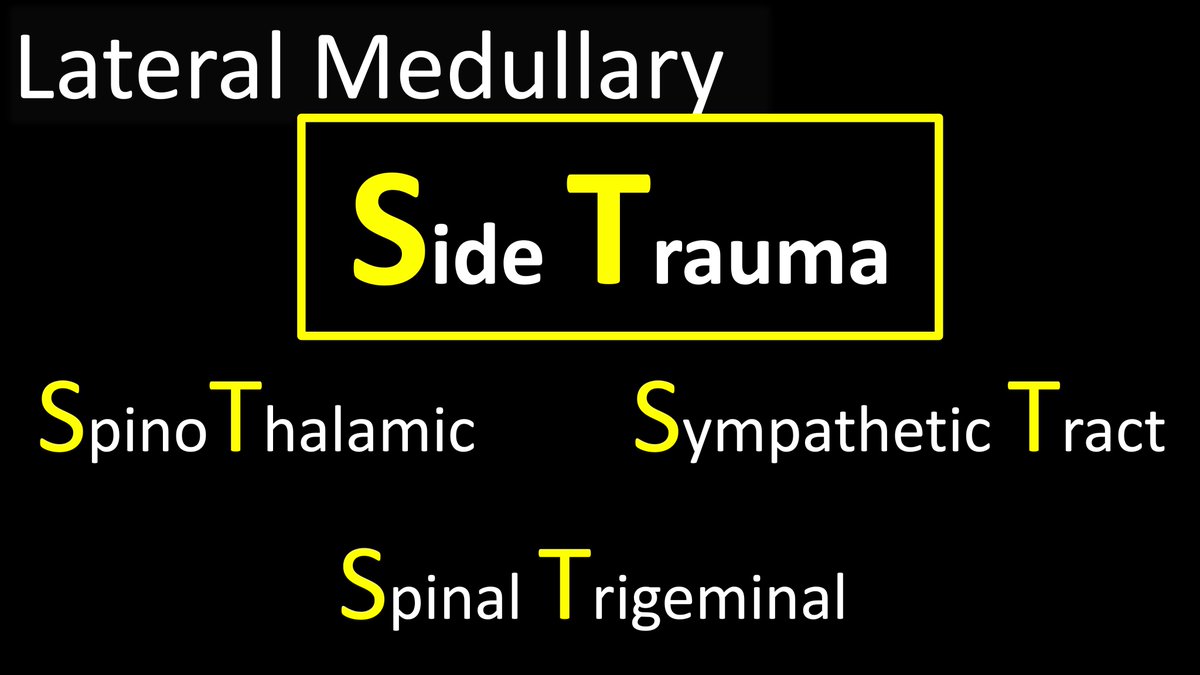
14/I remember the tracts bc lateral medullary syndrome is a result of an injury to the lateral aspect or SIDE of the medulla—a Side Trauma
And the tracts involved start w/S & T just like Side Trauma
And the tracts involved start w/S & T just like Side Trauma
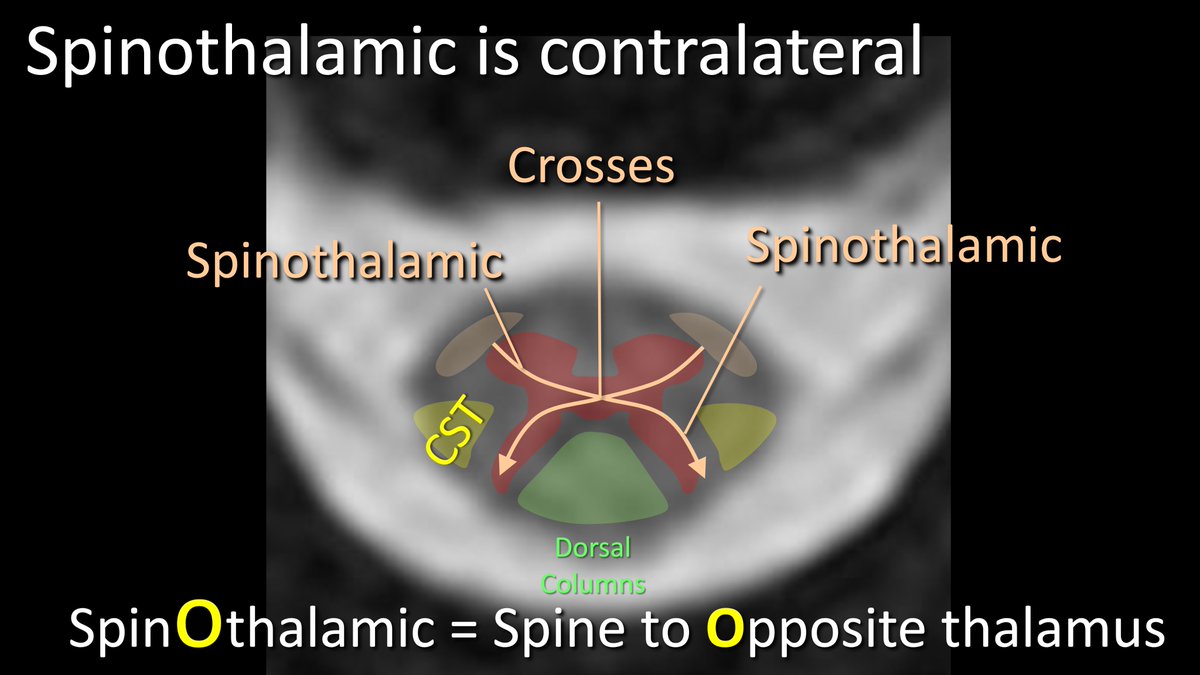
15/While the spinal trigeminal & sympathetic tracts are ipsilateral, the spinothalamic tract is contralateral.
I remember that it crosses b/c it has an O in the middle for OPPOSITE side
I call it the SPINE to OPPOSITE THALAMUS tract
I remember that it crosses b/c it has an O in the middle for OPPOSITE side
I call it the SPINE to OPPOSITE THALAMUS tract
16/To remember what is involved in lateral medullary syndrome—look what is involved on our praying mantis face:
his far lateral eyes = horner’s from sympathetics
his face = spinal trigeminal
his jowls/chewing mechanisms = dysphagia from CN 9 & 10 dysfunction
his far lateral eyes = horner’s from sympathetics
his face = spinal trigeminal
his jowls/chewing mechanisms = dysphagia from CN 9 & 10 dysfunction

17/And then, remember, the lateral/posterior medullary infarct looks like a punch to the face—so that burns!
That can help you to remember spinothalamic pain & temperature sensation loss
Other tracts are involved as well, but these main ones will help you get to the diagnosis!
That can help you to remember spinothalamic pain & temperature sensation loss
Other tracts are involved as well, but these main ones will help you get to the diagnosis!

18/So now you know the arterial territories of the medulla & how to remember the associated syndromes
So next time you have a medullary infarct, just remember the praying mantis face & you won’t have to bug anyone to help you!
So next time you have a medullary infarct, just remember the praying mantis face & you won’t have to bug anyone to help you!

• • •
Missing some Tweet in this thread? You can try to
force a refresh





















