COVID VACCINE: COST EFFECTIVENESS ASSESSMENT
For the first time ever, the UK government used a ‘bespoke non-standard cost-effectiveness assessment’ to decide who would be eligible for the Covid booster this Autumn.
In this 🧵, I explore how this assessment was undertaken…
For the first time ever, the UK government used a ‘bespoke non-standard cost-effectiveness assessment’ to decide who would be eligible for the Covid booster this Autumn.
In this 🧵, I explore how this assessment was undertaken…

It turns out that the government sensibly purchased enough doses of the updated Covid booster to give it to exactly the same cohort as last year - ie. everyone aged over 50 or in a risk group.
These doses had already been paid for upfront so they were treated as ‘sunk costs’.
These doses had already been paid for upfront so they were treated as ‘sunk costs’.

However, the UK government subsequently decided to only offer the vaccine to over 65s & at risk groups following their cost-effectiveness assessment.
This strategy is in stark contrast to the approach taken by many other countries, like US & Canada, where EVERYONE is eligible.
This strategy is in stark contrast to the approach taken by many other countries, like US & Canada, where EVERYONE is eligible.
https://twitter.com/CDCgov/status/1703859962449969553

Due to this decision to reduce eligibility for the Autumn booster, there are now 8.5 million people aged between 50-64 years but not considered ‘at risk’ who have been unable to get a booster this Autumn…
…despite the fact that vaccine doses have already been bought for them!
…despite the fact that vaccine doses have already been bought for them!

So what’s going to happen to the MILLIONS of purchased doses which now won’t be used?
Well, here’s the real kicker… it seems they’re destined for the bin!
A number of alternative uses have been considered but the conclusion is:
‘THESE DOSES HAVE NO FEASIBLE ALTERNATIVE USE’
Well, here’s the real kicker… it seems they’re destined for the bin!
A number of alternative uses have been considered but the conclusion is:
‘THESE DOSES HAVE NO FEASIBLE ALTERNATIVE USE’

So how did the gov come to this decision that it’s better to waste millions of doses instead of using them?
It all comes back to that ‘bespoke non-standard cost-effectiveness methodology’… the first time they’ve factored cost-effectiveness into their advice on Covid vaccines.
It all comes back to that ‘bespoke non-standard cost-effectiveness methodology’… the first time they’ve factored cost-effectiveness into their advice on Covid vaccines.

Using this ‘bespoke non-standard cost-effectiveness methodology’, the government looked at 3 different policy options to evaluate their cost-effectiveness and determine which option to proceed with.
Frustratingly, most of the cost-effectiveness figures are redacted.
However…
Frustratingly, most of the cost-effectiveness figures are redacted.
However…
…the trail of breadcrumbs is there if you look hard enough!
I’ve been through the 62 page ‘Impact Assessment’ document with a fine tooth comb and tried to fill in the gaps where I can to gain a better understanding of how they reached their decision. 👇🏻
assets.publishing.service.gov.uk/media/650ade0f…
I’ve been through the 62 page ‘Impact Assessment’ document with a fine tooth comb and tried to fill in the gaps where I can to gain a better understanding of how they reached their decision. 👇🏻
assets.publishing.service.gov.uk/media/650ade0f…

In summary, 3 options were considered:
OPTION 1:
📍all adults >65 yrs
📍all at risk or immunosuppressed >6 months
OPTION 2:
📍all adults >80 yrs
📍all at risk >45 yrs
📍all immunosuppressed >6 months
OPTION 3:
📍all adults >50 yrs
📍all at risk or immunosuppressed >6 months
OPTION 1:
📍all adults >65 yrs
📍all at risk or immunosuppressed >6 months
OPTION 2:
📍all adults >80 yrs
📍all at risk >45 yrs
📍all immunosuppressed >6 months
OPTION 3:
📍all adults >50 yrs
📍all at risk or immunosuppressed >6 months

Option 1 is the one they ultimately went for.
Option 3 would have been the same as last year’s Autumn booster.
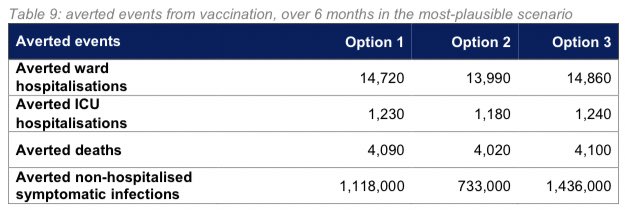
For each option, they modelled how many hospitalisations & deaths would be averted by vaccinating that particular cohort.
These figures underpin the whole analysis.
Option 3 would have been the same as last year’s Autumn booster.
For each option, they modelled how many hospitalisations & deaths would be averted by vaccinating that particular cohort.
These figures underpin the whole analysis.

By going for Option 3 instead of Option 1 (ie. an additional 8.5 million people aged 50-65 yrs), they estimate that it would avert an additional:
📍140 ward hospitalisations
📍10 ICU hospitalisations
📍10 deaths
📍318,000 non-hospitalised symptomatic infections.
📍140 ward hospitalisations
📍10 ICU hospitalisations
📍10 deaths
📍318,000 non-hospitalised symptomatic infections.
The modelling for this can be found here:
With the data I have, it’s impossible to verify these models, but the hospitalisation figures in particular seem low given that Covid hospitalisations in the 18-64 year olds ran into tens of thousands last Winter. gov.uk/government/pub…
With the data I have, it’s impossible to verify these models, but the hospitalisation figures in particular seem low given that Covid hospitalisations in the 18-64 year olds ran into tens of thousands last Winter. gov.uk/government/pub…

So, having estimated the number of averted hospitalisations & deaths using their model, how did they then assess the cost-effectiveness of each option?
It seems they looked at 3 main types of benefits to assess how much monetary benefit would accrue from each over 6 months.
It seems they looked at 3 main types of benefits to assess how much monetary benefit would accrue from each over 6 months.

A) DIRECT BENEFITS TO THE INDIVIDUAL VACCINATED:
This is measured in QALY’s (quality adjusted life years) based on the number of hospitalisations & deaths averted.
QALYs are converted into £ using the formula:
📍1 QALY = £20,000.
I’ve added the £ figures in red below.
This is measured in QALY’s (quality adjusted life years) based on the number of hospitalisations & deaths averted.
QALYs are converted into £ using the formula:
📍1 QALY = £20,000.
I’ve added the £ figures in red below.

B) FINANCIAL SAVINGS TO THE NHS:
NHS cost savings are calculated as follows:
📍each ward hospitalisation: £2,592;
📍each ICU hospitalisation: an additional £1,787 PER DAY (but they don’t say how many days);

📍each post-hospitalisation Long Covid sufferer: £1,134.
NHS cost savings are calculated as follows:
📍each ward hospitalisation: £2,592;
📍each ICU hospitalisation: an additional £1,787 PER DAY (but they don’t say how many days);

📍each post-hospitalisation Long Covid sufferer: £1,134.

It’s important to note that, although they did factor some Long Covid costs into the equation, they ONLY factored it in for those who had been hospitalised.
They assumed ZERO benefit to those who weren’t hospitalised from reduced incidence of Long Covid after vaccination.
They assumed ZERO benefit to those who weren’t hospitalised from reduced incidence of Long Covid after vaccination.

C) INDIRECT HEALTH BENEFITS TO WIDER POPULATION:
The analysis also factors in benefits to the wider population from averted Covid hospitalisations freeing up NHS resources for elective care operations instead.
This is also measured in QALYs which I’ve converted to £ below:
The analysis also factors in benefits to the wider population from averted Covid hospitalisations freeing up NHS resources for elective care operations instead.
This is also measured in QALYs which I’ve converted to £ below:

D) NON-HEALTH BENEFITS
The analysis also acknowledges that there are other non-health benefits, such as preventing work absences and supporting productivity in the economy - however these sorts of benefits were NOT appraised in the analysis for the reasons detailed below 👇🏻
The analysis also acknowledges that there are other non-health benefits, such as preventing work absences and supporting productivity in the economy - however these sorts of benefits were NOT appraised in the analysis for the reasons detailed below 👇🏻

So we now have all the pieces of the jigsaw to recreate the redacted monetised benefits table. 👇🏻
The next step is to work out which of these options are cost-effective when compared to the vaccine deployment costs…
The next step is to work out which of these options are cost-effective when compared to the vaccine deployment costs…

To work out if the vaccine is cost-effective for each option, the total monetised QALY benefits + NHS Savings are summed & then divided by total doses estimated to be delivered (factoring in uptake rates).
This gives the “Willingness to Pay’ (WTP) price per dose for deployment…
This gives the “Willingness to Pay’ (WTP) price per dose for deployment…

The table below shows my calculation of the Willingness to Pay (WTP) price for each option:
📍Option 1: £29.38 per dose
📍Option 2: £40.93 per dose
📍Option 3: £23.37 per dose
To determine which options are cost-effective, this is then compared to the deployment cost per dose.
📍Option 1: £29.38 per dose
📍Option 2: £40.93 per dose
📍Option 3: £23.37 per dose
To determine which options are cost-effective, this is then compared to the deployment cost per dose.

The lower estimate vaccine deployment cost is £10 per dose…
Good news! All 3 options exceed this deployment cost threshold!
Even for Option 3, once the £10 per dose deployment cost has been deducted, there’s still £263 MILLION of monetised benefits left over (£13.37 x 19.7m).
Good news! All 3 options exceed this deployment cost threshold!
Even for Option 3, once the £10 per dose deployment cost has been deducted, there’s still £263 MILLION of monetised benefits left over (£13.37 x 19.7m).

Now what about the higher estimate vaccine deployment cost, which includes “all capital & one-off costs of setting up a pandemic response programme”?
This figure is redacted. 🙄
But perhaps the £263 million surplus from the calculation above would be sufficient to cover this?
This figure is redacted. 🙄
But perhaps the £263 million surplus from the calculation above would be sufficient to cover this?

But there’s more…
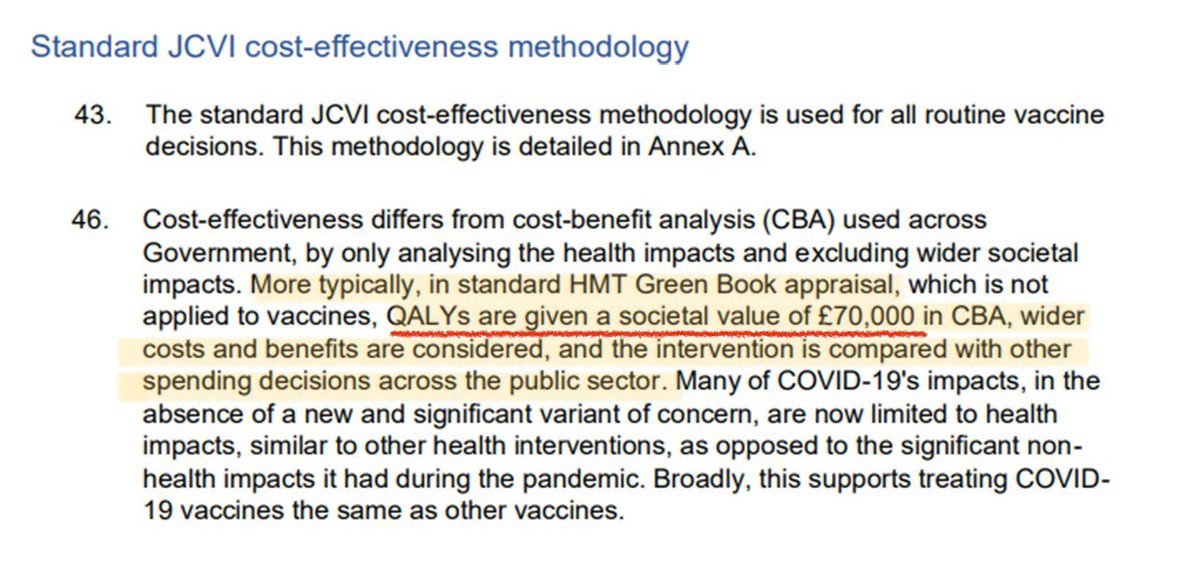
Hidden within the doc, I found this comment:
“More typically, in standard HMT Green Book appraisal… QALYs are given a societal value of £70,000”.
Given the wider impact on society that Covid has, would it not be more appropriate to use this QALY figure?
Hidden within the doc, I found this comment:
“More typically, in standard HMT Green Book appraisal… QALYs are given a societal value of £70,000”.
Given the wider impact on society that Covid has, would it not be more appropriate to use this QALY figure?
I’ve re-run the Willingness to Pay (WTP) calculation using this revised QALY conversion rate of 1 QALY = £70,000.
Obviously this makes all the options considerably more cost-effective:
📍Option 1: £92.74 per dose
📍Option 2: £128.92 per dose
📍Option 3: £73.93 per dose
Obviously this makes all the options considerably more cost-effective:
📍Option 1: £92.74 per dose
📍Option 2: £128.92 per dose
📍Option 3: £73.93 per dose

Having run these calculations, I couldn’t quite figure out how they had come to the conclusion that Option 3 (vax for ALL over 50s) was not cost effective.
Perhaps the higher estimated cost for deployment was greater than £23?
But then I realised there was a different reason…
Perhaps the higher estimated cost for deployment was greater than £23?
But then I realised there was a different reason…
I’ve done my calculations based on the cost-effectiveness of each option as a WHOLE.
Therefore a surplus of monetised benefits in some of the older/higher risk sub-groups means a slightly lower cost-effectiveness can be accepted in other sub-groups.
They balance each other out!
Therefore a surplus of monetised benefits in some of the older/higher risk sub-groups means a slightly lower cost-effectiveness can be accepted in other sub-groups.
They balance each other out!
But reading between the redacted lines, it appears that the government’s methodology differs from mine in one key regard…
Rather than looking at cost-effectiveness for each option as a WHOLE, they calculated the WTP within highly stratified age brackets for each risk profile.
Rather than looking at cost-effectiveness for each option as a WHOLE, they calculated the WTP within highly stratified age brackets for each risk profile.

As soon as a single sub-group fell below the cost-effective threshold, that’s where they drew the line.
Large surplus benefits from some sub-groups were not used to offset against other sub-groups who fell just slightly below the threshold.
Large surplus benefits from some sub-groups were not used to offset against other sub-groups who fell just slightly below the threshold.
The specific WTP figures are again redacted & I don’t have the data I’d need to recreate them but the colour coding tells us all we need to know...
🔴Red = NOT cost effective, even at marginal £10 deployment cost per dose
🟡Yellow = cost effective at £10 cost per dose
🔴Red = NOT cost effective, even at marginal £10 deployment cost per dose
🟡Yellow = cost effective at £10 cost per dose

Please don’t stop reading here - the most interesting part is yet to come!
Click “Show replies” to see rest of the thread).
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
Click “Show replies” to see rest of the thread).
⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️⬇️
So, as you can see from the colour coding, ALL age groups under 80 & not at risk now fall short of being cost-effective.
Using this approach, the government was cleverly able to spin the cost-effectiveness analysis to say that NEITHER option 1 or option 3 were cost-effective.
Using this approach, the government was cleverly able to spin the cost-effectiveness analysis to say that NEITHER option 1 or option 3 were cost-effective.

By agreeing to go for Option 1, they were then able to position it as going above & beyond a pure cost-effectiveness calculation and claim to be acting on a “precautionary basis”.
It’s a masterclass in gaslighting! 🔥
It’s a masterclass in gaslighting! 🔥

Quite frankly, I find the whole concept of this cost-effectiveness analysis extremely concerning and not just because of the questionable number crunching…
The fundamental question is whether the vaccine strategy for Covid should be underpinned by cost-effectiveness at all.
The fundamental question is whether the vaccine strategy for Covid should be underpinned by cost-effectiveness at all.
Shouldn’t we ALL have the choice to be vaccinated, given what we now know about the harms it can cause?
Covid is not just a ‘mild cold’.
The CDC estimate that ~1 in 5 adults now have a health condition that may be related to their previous Covid infection.
That’s 20% of us!
Covid is not just a ‘mild cold’.
The CDC estimate that ~1 in 5 adults now have a health condition that may be related to their previous Covid infection.
That’s 20% of us!

Covid can damage your lungs, heart, brain, kidneys & basically every other organ of your body.
Even if it doesn’t kill you, it can leave you with serious long-term health problems.
You just might not know it yet.
nature.com/articles/s4157…
Even if it doesn’t kill you, it can leave you with serious long-term health problems.
You just might not know it yet.
nature.com/articles/s4157…

And the risk of severe health outcomes increases with each successive reinfection.
Just because you’ve had Covid before and were fine, it doesn’t mean you’ll be fine next time.
You roll the dice every single time you get infected…
nature.com/articles/s4159…
Just because you’ve had Covid before and were fine, it doesn’t mean you’ll be fine next time.
You roll the dice every single time you get infected…
nature.com/articles/s4159…

We’re also seeing worrying high figures for excess deaths in the under 65’s.
The % increase in registered deaths versus expected deaths so far this year is:
0-24 yrs: 11%
25-49 yrs: 10%
50-64 yrs: 14%
These are the age groups NOT eligible for vaccination!
The % increase in registered deaths versus expected deaths so far this year is:
0-24 yrs: 11%
25-49 yrs: 10%
50-64 yrs: 14%
These are the age groups NOT eligible for vaccination!
https://twitter.com/_CatintheHat/status/1720404171411628201
Now I’m not suggesting that vaccination is a silver bullet…
We know the current vaccines don’t always prevent infection but they certainly do reduce the severity of illness and also the risk of long Covid to some extent.
health.harvard.edu/diseases-and-c…
We know the current vaccines don’t always prevent infection but they certainly do reduce the severity of illness and also the risk of long Covid to some extent.
health.harvard.edu/diseases-and-c…

And it’s not just about risks to health.
As Prof Cruickshank (@sheencr) points out in this article:
“The more infections we have in a population, the greater the opportunity the virus has to keep mutating. Vaccination can, to an extent, reduce this.”
theguardian.com/commentisfree/…
As Prof Cruickshank (@sheencr) points out in this article:
“The more infections we have in a population, the greater the opportunity the virus has to keep mutating. Vaccination can, to an extent, reduce this.”
theguardian.com/commentisfree/…
@sheencr If the UK government are not prepared to pay for everyone to get vaccinated, surely we should at least have the chance to pay for it ourselves?
I’m sure there are many who would pay £10 to receive one of those vaccine doses currently sitting in storage fridges & about to expire.
I’m sure there are many who would pay £10 to receive one of those vaccine doses currently sitting in storage fridges & about to expire.
@sheencr Moving forwards, I fear this situation will only going to get worse…
It recently came to light that Covid funding is planned to be phased out entirely to £0 by the end of this year!
H/t @karamballes
gov.uk/government/pub…
It recently came to light that Covid funding is planned to be phased out entirely to £0 by the end of this year!
H/t @karamballes
gov.uk/government/pub…

Meanwhile, we’re destined to have to “live with Covid” for the foreseeable future.
But “living with Covid” just means getting sick with Covid, over & over again.
For anyone paying attention, it’s clear we’re headed for a crisis…
…a health crisis & an economic one too.
But “living with Covid” just means getting sick with Covid, over & over again.
For anyone paying attention, it’s clear we’re headed for a crisis…
…a health crisis & an economic one too.
https://twitter.com/_CatintheHat/status/1711746097331192176
One final point to add to this troubling tale…
Even for those who ARE eligible for the Covid booster… those who’ve been sent a letter acknowledging their ‘high risk’ status and invited to book their vaccination… they STILL don’t exactly make it easy for you!
Even for those who ARE eligible for the Covid booster… those who’ve been sent a letter acknowledging their ‘high risk’ status and invited to book their vaccination… they STILL don’t exactly make it easy for you!
https://twitter.com/_CatintheHat/status/1722258703334986055
EDIT: It’s been brought to my attention by @JCoffinhal that the fee paid to vax centres was actually REDUCED from £10.06 to £7.54 in early Sept.
Once this reduced deployment cost has been deducted, Option 3 now gives surplus benefits of £311.9 MILLION.
bma.org.uk/advice-and-sup…
Once this reduced deployment cost has been deducted, Option 3 now gives surplus benefits of £311.9 MILLION.
bma.org.uk/advice-and-sup…
https://twitter.com/JCoffinhal/status/1725955800303108116

@JCoffinhal It’s now emerged that the 25% reduction in the ‘Item Service Fee’ paid to vax centres was first announced on 4 Aug.
That’s over 6 weeks BEFORE Maria Caulfield signed the Impact Assessment on 19 Sept confirming she was “satisfied it represents a reasonable view of likely costs”.
That’s over 6 weeks BEFORE Maria Caulfield signed the Impact Assessment on 19 Sept confirming she was “satisfied it represents a reasonable view of likely costs”.
https://twitter.com/JCoffinhal/status/1727034818976694329

@JCoffinhal UPDATE: Prompted by comments that the eligibility criteria for the flu & Covid vaccine are “quite similar”, I’ve done another thread below which demonstrates how different they actually are.
They say: “Treat it like the flu”…
…so why don’t *they* treat it like the flu?!
They say: “Treat it like the flu”…
…so why don’t *they* treat it like the flu?!
https://twitter.com/_CatintheHat/status/1728080737734115468
• • •
Missing some Tweet in this thread? You can try to
force a refresh