Minimize the number of times you get Covid. Your body will thank you.
Not only can repeat infections inflict Long Covid, they also, as @zalaly has shown, increase the risk of a multitude of ailments, such as cardiovascular events.
1/5
Not only can repeat infections inflict Long Covid, they also, as @zalaly has shown, increase the risk of a multitude of ailments, such as cardiovascular events.
1/5
https://twitter.com/zalaly/status/1733960130298077438
Cardiovascular events are the largest factor behind the continuing Covid-era excess deaths in the UK.
In light of such statistics, the decision of many governments to deny access to updated booster shots to much of the population staggers the mind.
2/5
In light of such statistics, the decision of many governments to deny access to updated booster shots to much of the population staggers the mind.
2/5
https://twitter.com/ActuaryByDay/status/1731580524236280077
You'll repeatedly acquire immunity one way or another. The more you get through vaccination, the less you'll get through infection.
Would you like to suffer more illness & higher risk of long-term health issues? Or would you prefer less of both? It's not a hard call. 3/5
Would you like to suffer more illness & higher risk of long-term health issues? Or would you prefer less of both? It's not a hard call. 3/5
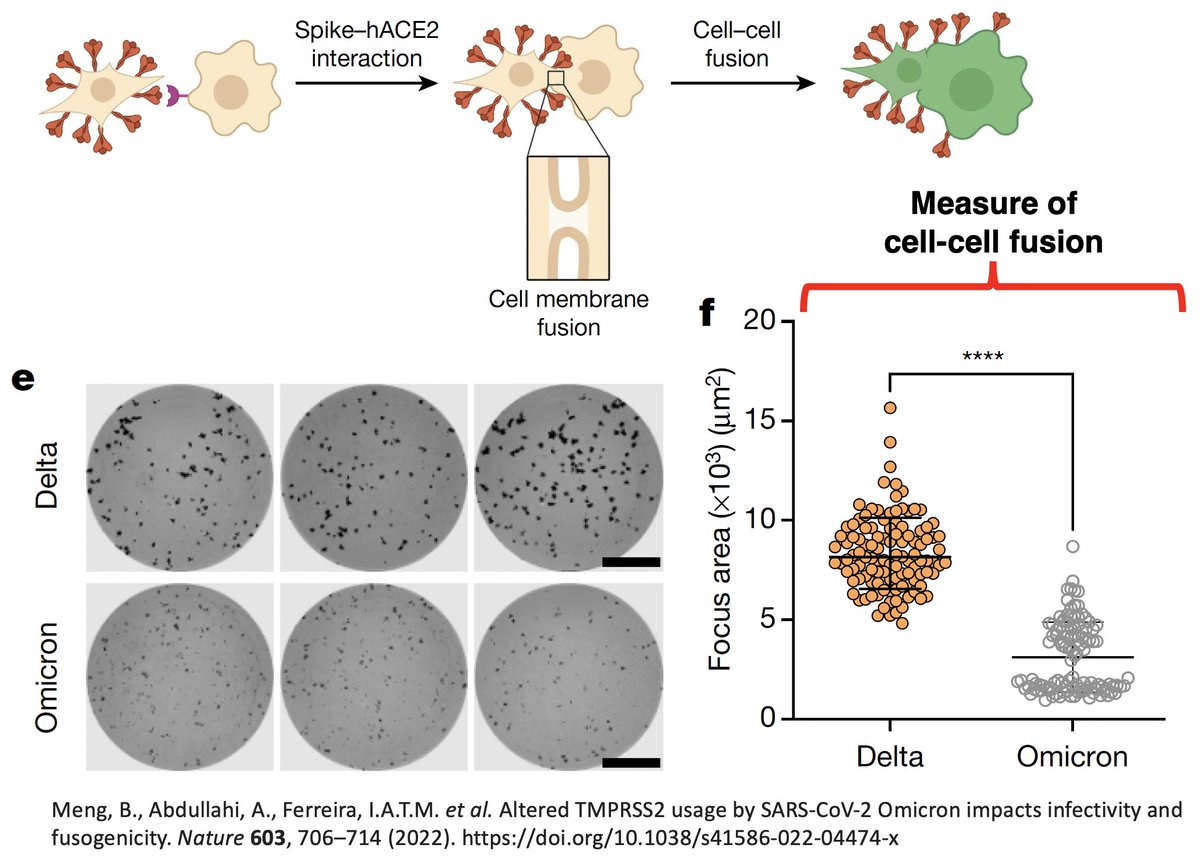
And thanks to the magic of affinity maturation, even an imperfect shot is valuable. Exposure to a large variety of spike can, over the long term, grant you an effective antibody response even against variants that don't yet exist.
4/5
4/5
https://twitter.com/LongDesertTrain/status/1566482826865909767
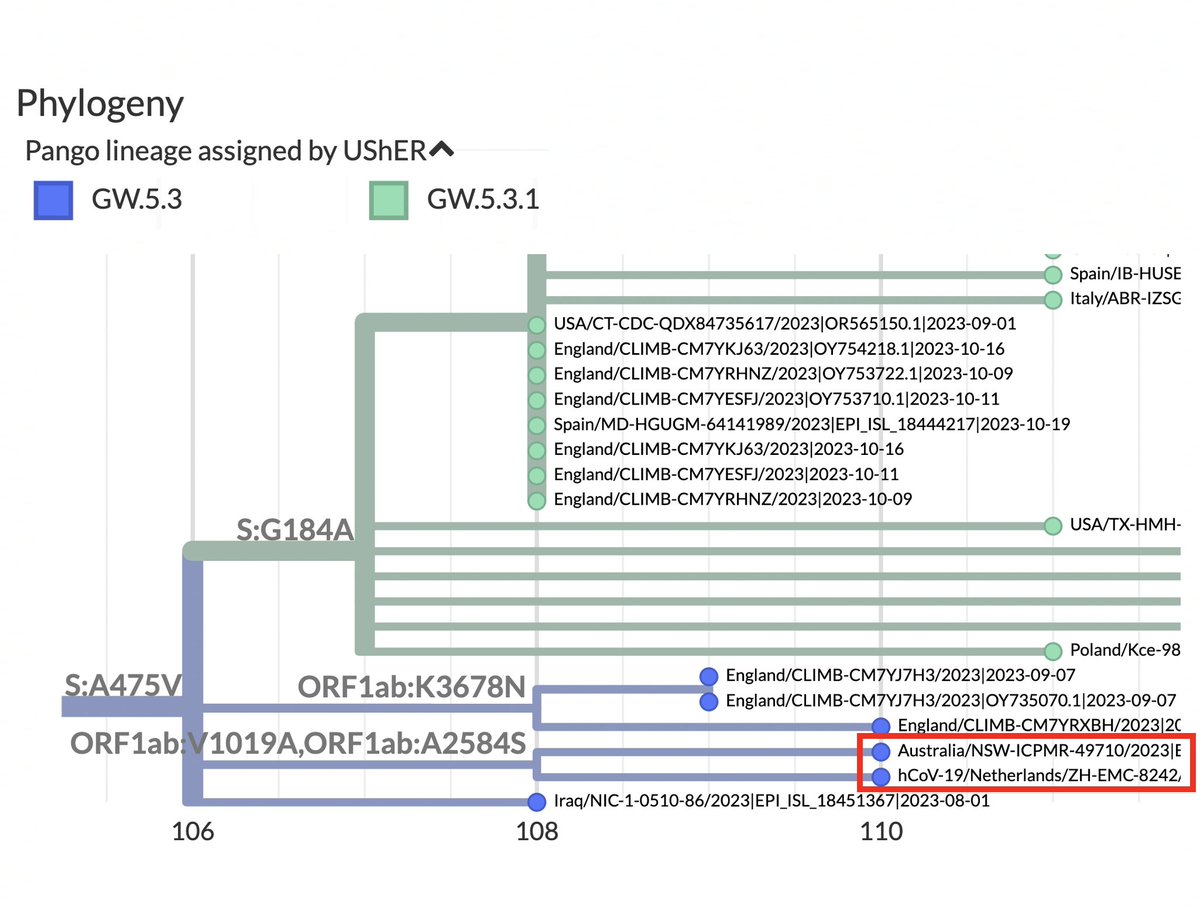
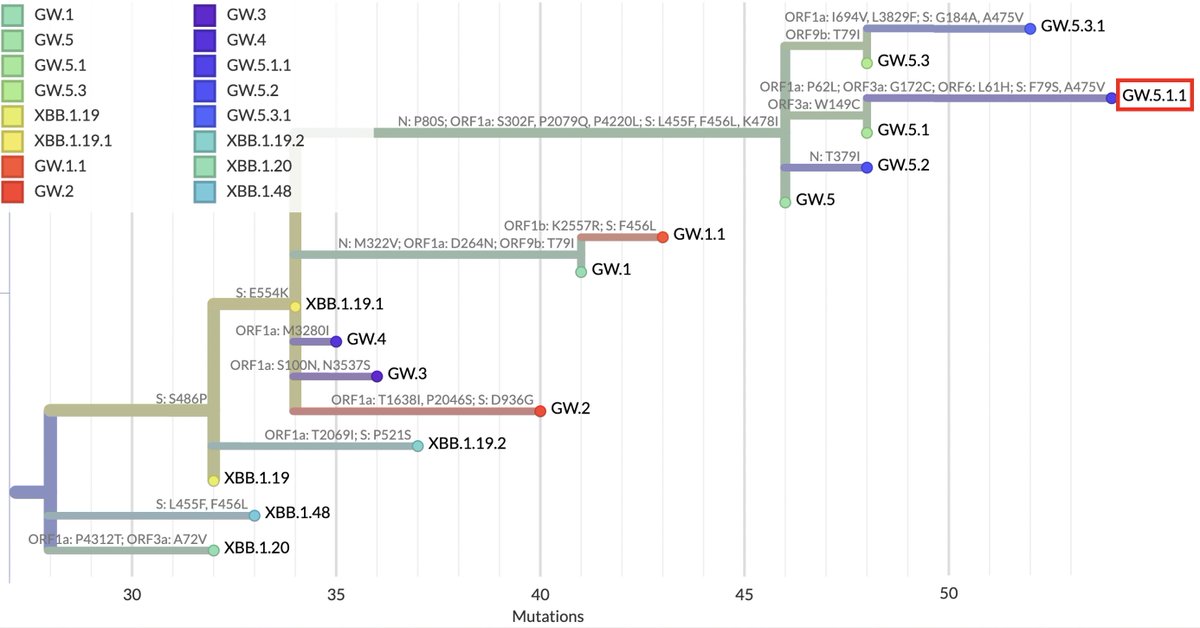
Ideally, we'd have a JN.1 shot by January. If you want to reduce infections, it's an easy call. Sadly, that's not on the table.
But the XBB.1.5 booster is the best-matched shot we've had in 2 years—even considering imminent JN.1 dominance. It would be foolish not to get it. 5/5
But the XBB.1.5 booster is the best-matched shot we've had in 2 years—even considering imminent JN.1 dominance. It would be foolish not to get it. 5/5
• • •
Missing some Tweet in this thread? You can try to
force a refresh