Broad-Spectrum #COVID-19 #Therapeutics and #Prophylactics
An interesting presentation by Yunlong Richard Cao @yunlong_cao talking about their development of broadly #neutralizing #antibodies based on prediction of #viral #evolution ( ). 🧵1/

An interesting presentation by Yunlong Richard Cao @yunlong_cao talking about their development of broadly #neutralizing #antibodies based on prediction of #viral #evolution ( ). 🧵1/

Read on to find out how their research team developed a neutralizing antibody solution (injection & nose spray) that works with all current variants, including the older SARS1 virus from 2003 and the currently globally dominant BA.2.86 Pirola clan of variants. 2/


An unrolled one-page web view for this long thread that may be easier to read or share can be found here ( ). 3/
https://twitter.com/jeffgilchrist/status/1744881989956616467
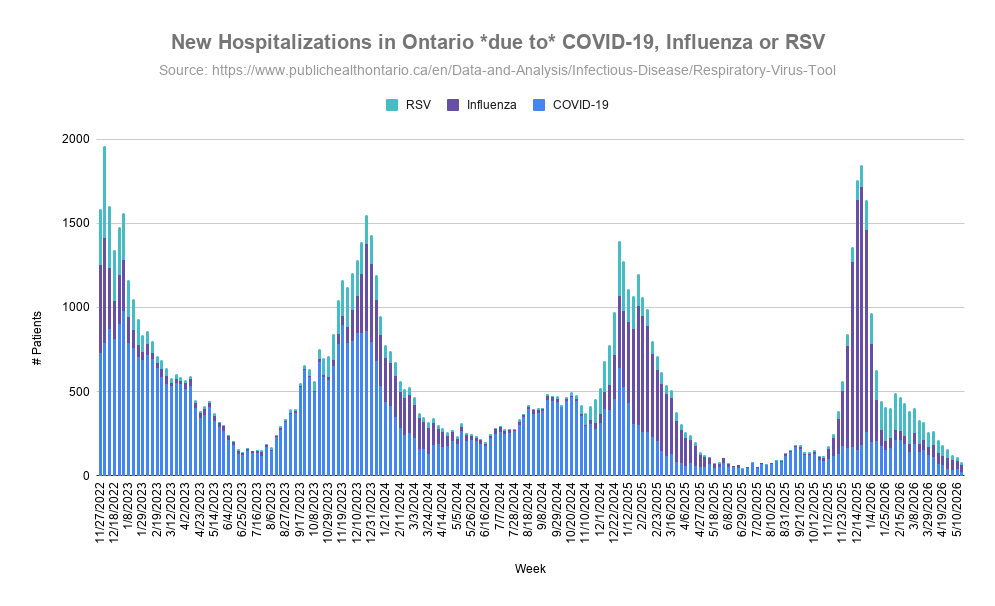
The COVID-19 virus is evolving so quickly with such massive unmitigated transmission that clinical development of vaccines and antibody drug development is too slow and can't keep pace. 4/
Even if updated vaccines can be designed quickly, they still take 4+ months to deploy and by then the variant landscape has already changed. 5/
Back in 2020 Dr. Cao found 300 human neutralizing antibodies and their team picked the 2 most potent antibodies to develop therapeutics. 6/
They passed phase 2 clinical trials but before they were ready to be used, the Omicron variant could already escape the antibodies, wasting about $150M. 7/

What is really interesting, there are still several of those original 300 neutralizing antibodies that remain potent to all variants to date, so they chose the wrong antibodies to develop. 8/
Dr. Cao wanted to find out how you identify the most broad-spectrum antibodies instead of the most potent ones so they are more likely to remain effective even with viral evolution. 9/
If you can try to predict viral evolution you might be able to select or design the best antibodies that will work long-term. 10/
For the past few years, Dr. Cao has been working on predicting the evolution of the SARS-CoV-2 virus. While mutations in the virus happen randomly, only the fittest survive and become successful which usually means they need to follow two criteria:
11/
11/
1) maintain high binding efficiency to the ACE2 receptor to ensure viral replication
2) escape human neutralizing antibodies to evade immunity
12/
2) escape human neutralizing antibodies to evade immunity
12/

Following that hypothesis, Dr. Cao's team did high-throughput experiments to measure the impact of each mutation on the virus' infectivity and immune escape capability to predict the "optimal solution" for viral evolution. 13/
Using techniques developed over time they published a predictive model and highly immune evasive variant sequences in Sept. 2022. 14/
One month later in Oct. 2022 the BQ.1.1 and CH.1.1 variants that emerged XBB variant in Nov. 2022 sequentially gained the top 3 predicted mutations (346, 444, 460) and 490 for XBB. 15/

Now it was time to try again to develop another solution but this time based on their virus evolution prediction model. 16/
They started with people who had been infected with SARS1 in 2003 who also had a COVID-19 vaccination in 2021 to screen 1400 antibodies and selected 1 for development. 17/
The neutralizing antibody they developed is called SA55 which can also neutralize SARS1 and many sarbecoviruses. 18/
You can see from the table that over time as new variants emerged, the other antibody therapeutics all stopped working since the virus evolved to escape those antibodies, while SA55 continues to neutralize even the latest BA.2.86 Pirola variants that are dominating globally. 19/
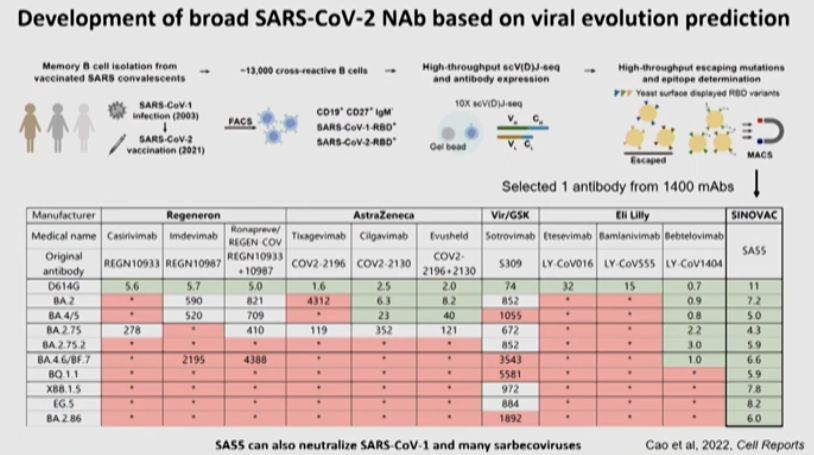
Previously, the most potent antibodies were selected which has already proven to be a bad strategy, instead you need to screen for the most broad ones. 20/
The reason they selected SA55 was by doing the mutation screening they found that SA55 can only be escaped by mutations on 503 and 504. 21/

From their prediction model they know there is currently no immune pressure at locations 503 and 504 at all so choosing this antibody was a very safe choice. 22/
It is very difficult for a virus carrying mutations in location 503 and 504 to successfully transmit among a population which helps explain why after 2.5 years this antibody has not yet been evaded. 23/
SA55 has been made into multiple tools already. One is an injection for immunocompromised people to act as a long-term prophylactic with an 80-90 day half-life or therapeutic. It has already been used to treat 2,000 elderly patients in Beijing during the outbreak in December. 24/

The second tool is a SA55 nasal spray that is supposed to be low cost and provide short-term prophylactics (3 sprays per day) with 8-12h protection per spray providing high neutralization in the mucosa. 25/

It has been used by over 200,000 people and provides about 80% protection against symptomatic infection. 26/
The real challenge is future vaccines. Choosing the XBB.1.5 variant for this fall's vaccine dose selection was not the optimal solution but a practical solution. 27/
From the time the XBB.1.5 variant was chosen in May to when the vaccine was deployed in the USA (September), there was already a 4x decrease in vaccine efficacy because variants had changed so much through natural evolution. 28/
Instead of always being behind, a new strategy is needed for COVID vaccine development and Dr. Cao suggests creating a broad-spectrum vaccine based on viral evolution prediction. 29/

Instead of basing vaccines on already existing naturally occurring variants, design them based on mutation prediction from current variants to determine what the most likely mutations are going to be. 30/
Hopefully vaccine manufacturers will start using better strategies like this in the future than always chasing variants and being left behind. 31/
@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh