1/ Today's 🧵 is about the #Sgarbossa Criteria and #Concordance vs #Discordance in simple words.
The objective of this post is to clarify any doubts in a simple, graphic and didactic way. #CardioTwitter @ekgdx
The objective of this post is to clarify any doubts in a simple, graphic and didactic way. #CardioTwitter @ekgdx

2/ The Sgarbossa criteria were initially introduced over two decades ago to enhance the diagnostic precision for MI in the setting of LBBB. This criteria is widely accepted as one of the most valuable tools to assist in the diagnosis of MI when LBBB is present.
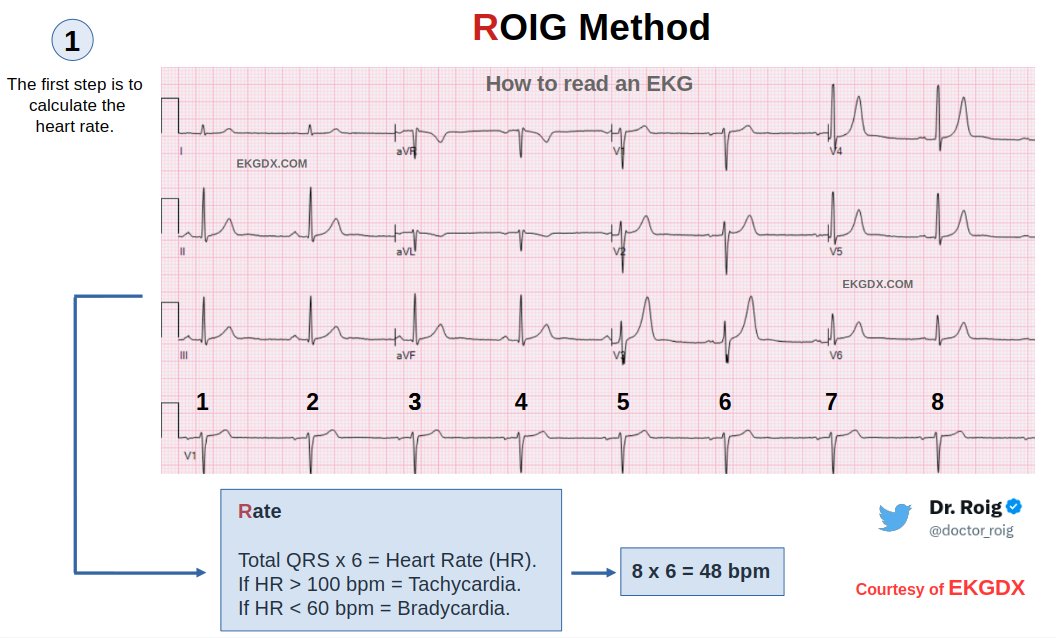
Here you can see a classic example with graphic explanations that will facilitate understanding.
Here you can see a classic example with graphic explanations that will facilitate understanding.

3/ The Sgarbossa Criteria were initially introduced in 1996 by @ElenaSgarbossa et al. They used data from the famous GUSTO-1 trial.
Article🔗 nejm.org/doi/10.1056/NE…
Article🔗 nejm.org/doi/10.1056/NE…
4/ Subsequent modifications by other authors have aimed to improve sensitivity.
Modified Sgarbossa Criteria by @smithECGBlog et al. 2012.
Article 🔗 annemergmed.com/article/S0196-…
Modified Sgarbossa Criteria by @smithECGBlog et al. 2012.
Article 🔗 annemergmed.com/article/S0196-…


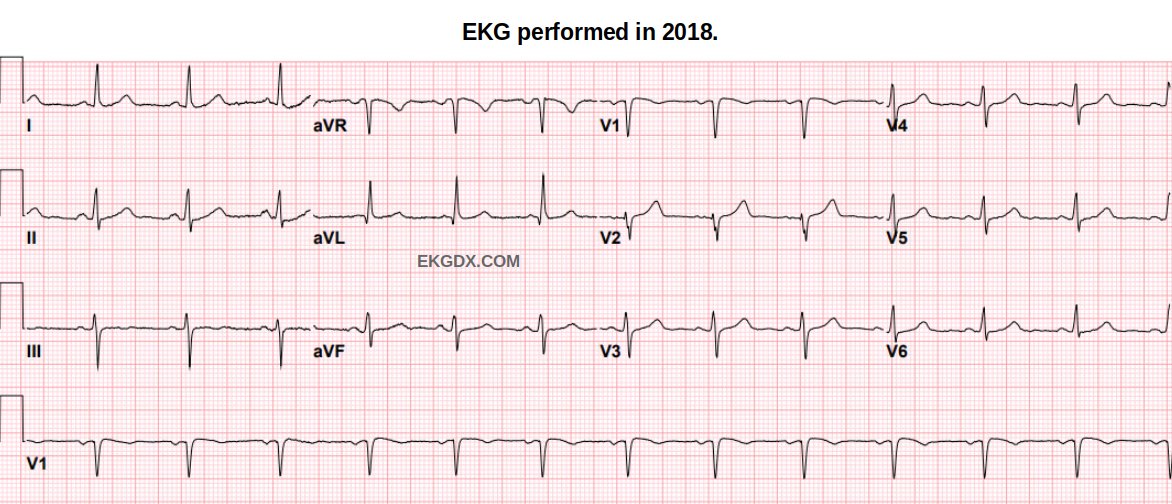
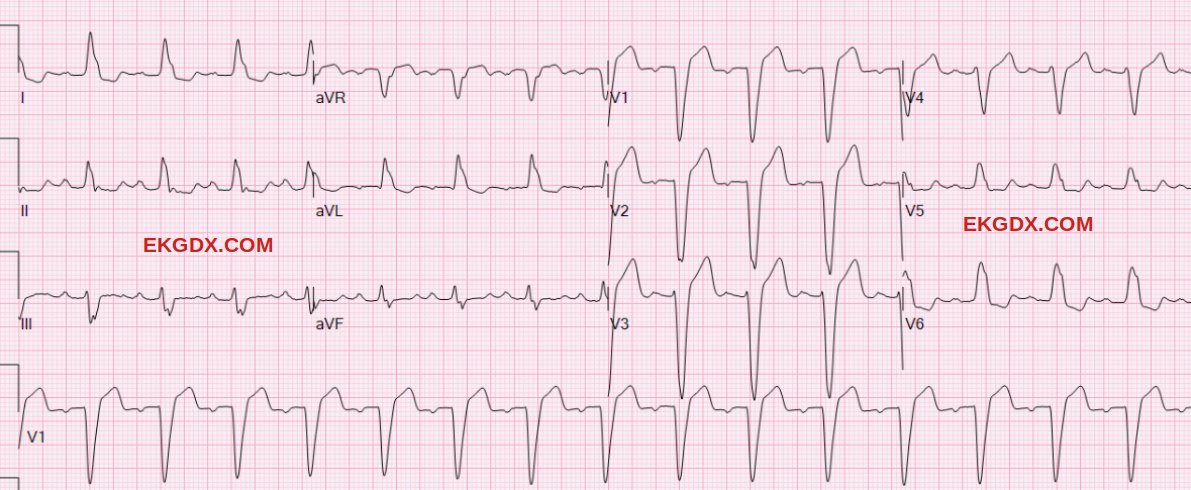
6/ Here an EKG with classic LBBB and no acute MI.
7/ Below are few examples of acute myocardial infarction in the setting of LBBB.
Courtesy of @syamkumarmd
Courtesy of @syamkumarmd
https://x.com/syamkumarmd/status/1484341176765321220?s=20
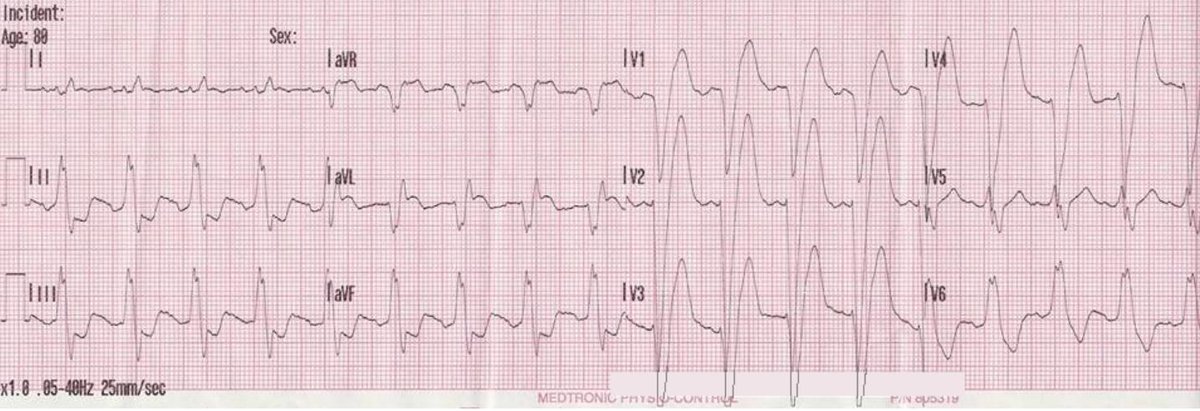
8/ Another sample of acute MI in the setting of LBBB.
Courtesy of ECG Medical Training.
Courtesy of ECG Medical Training.
9/ Another sample of acute MI in the setting of LBBB.
Red circle shows concordant ST segment elevation. Courtesy of Dr. Carlos Pineda from ECG Weekly.
Red circle shows concordant ST segment elevation. Courtesy of Dr. Carlos Pineda from ECG Weekly.

10/ Regarding diagnostic accuracy and sensitivity-specificity for each criteria, please consult the references.
🔗 ekgdx.com/references/#Sg…
🔗 ekgdx.com/references/#Sg…

11/ Who or what is Sgarbossa?
Elena B. Sgarbossa, MD (@ElenaSgarbossa ), is an American cardiologist, author, and medical translator, originally from Argentina. This criteria is widely accepted as one of the most valuable tools to assist in the diagnosis of MI when LBBB is present.
Elena B. Sgarbossa, MD (@ElenaSgarbossa ), is an American cardiologist, author, and medical translator, originally from Argentina. This criteria is widely accepted as one of the most valuable tools to assist in the diagnosis of MI when LBBB is present.
12/ Take this home
✅ Sgarbossa criteria was a game changer.
✅ Subsequent modifications by other authors have aimed to improve sensitivity. You must study all of them.
✅ You can’t rule out an acute myocardial infarction if the criteria are absent.
✅ Sgarbossa criteria was a game changer.
✅ Subsequent modifications by other authors have aimed to improve sensitivity. You must study all of them.
✅ You can’t rule out an acute myocardial infarction if the criteria are absent.
14/ End
Thanks for reading this 🧵.
If you find this content helpful, please:
1- Follow @doctor_roig and @ekgdx for more.
2- Repost the first tweet for support.
Thanks for reading this 🧵.
If you find this content helpful, please:
1- Follow @doctor_roig and @ekgdx for more.
2- Repost the first tweet for support.
• • •
Missing some Tweet in this thread? You can try to
force a refresh