1/Do questions about brainstem anatomy cause you to suddenly get a case of locked in syndrome?!
Feeling brain dead when trying to localize in the brain stem?
Do you try to localize the lesion or just wait for the MR?
Here’s a thread to help w/brainstem anatomy & localization!
Feeling brain dead when trying to localize in the brain stem?
Do you try to localize the lesion or just wait for the MR?
Here’s a thread to help w/brainstem anatomy & localization!

2/First some gross anatomy.
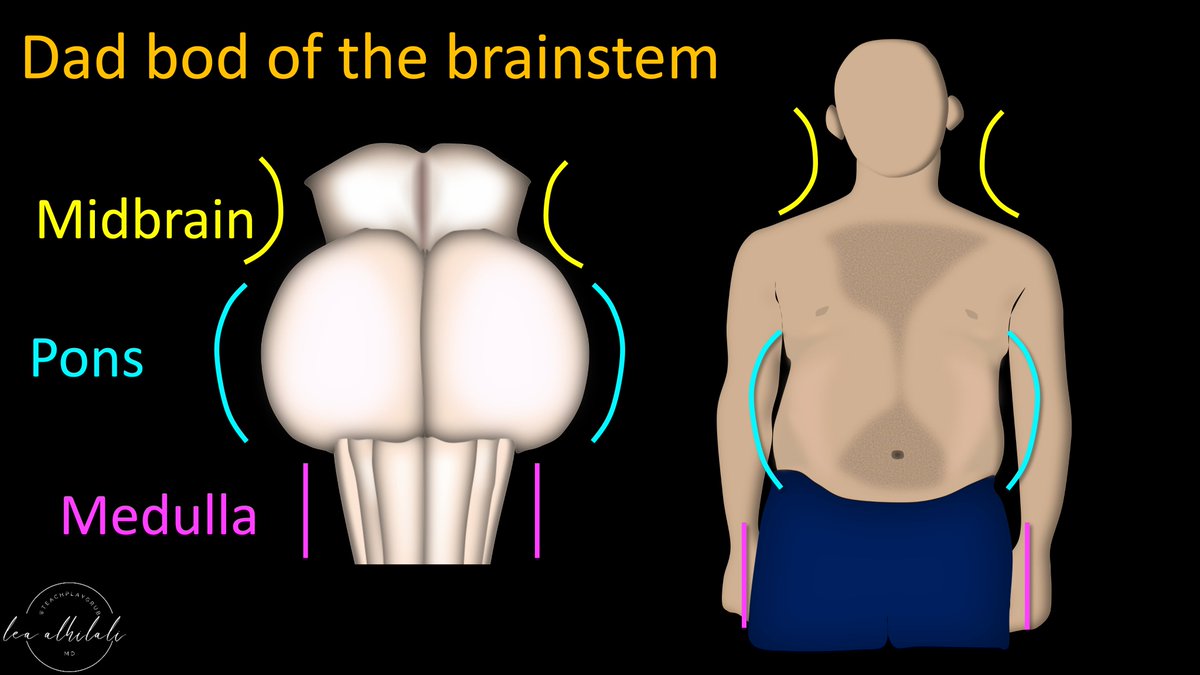
Brainstem from the side looks like a dad-bod--the body you get after kids wear you down & you don’t exercise anymore.
Head & shoulders are the midbrain, potbelly is the pons, & fat thighs are the medulla
Brainstem from the side looks like a dad-bod--the body you get after kids wear you down & you don’t exercise anymore.
Head & shoulders are the midbrain, potbelly is the pons, & fat thighs are the medulla

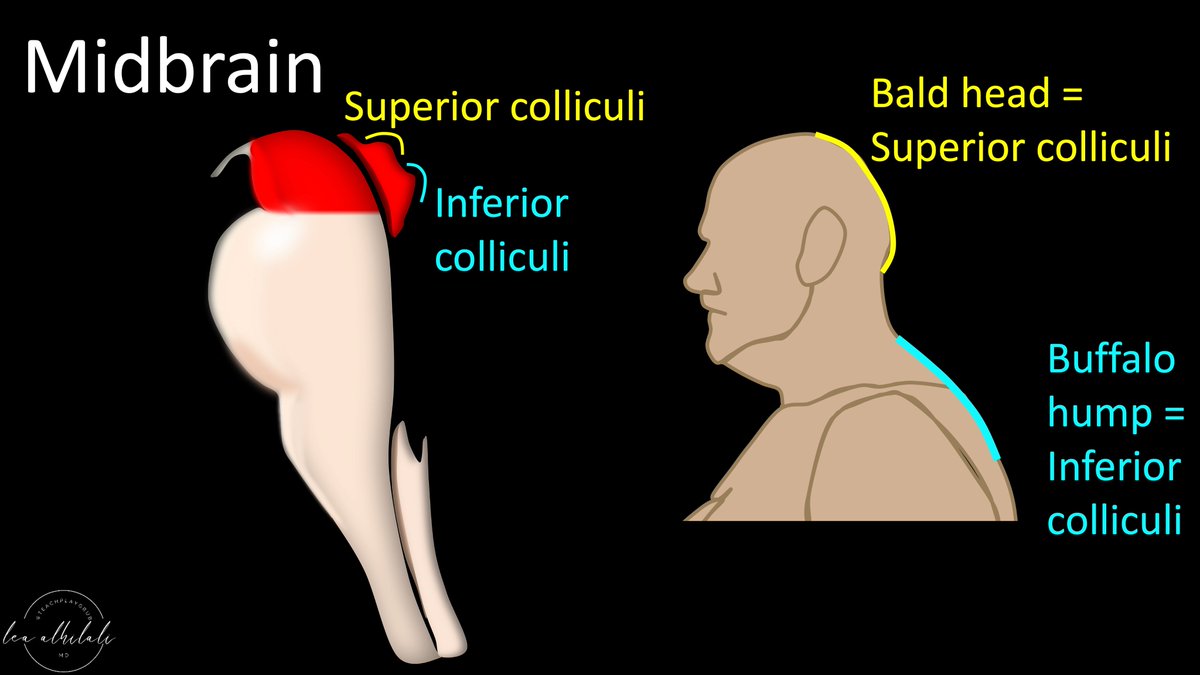
3/Midbrain is the head & shoulders.
This makes sense b/c the name “midbrain”—brains should be in the head.
Midbrain also has the cerebral peduncles which look like classic Mickey Mouse ears—and dads classically have big, usually hairy, ears
This makes sense b/c the name “midbrain”—brains should be in the head.
Midbrain also has the cerebral peduncles which look like classic Mickey Mouse ears—and dads classically have big, usually hairy, ears

4/Back of the midbrain has 2 bumps—superior & inferior colliculi (parts of vision & auditory pathways, respectively)
You can see these bumps on the dad bod too
Back of the balding head is the superior colliculus & the buffalo hump from his obesity is the inferior colliculus
You can see these bumps on the dad bod too
Back of the balding head is the superior colliculus & the buffalo hump from his obesity is the inferior colliculus
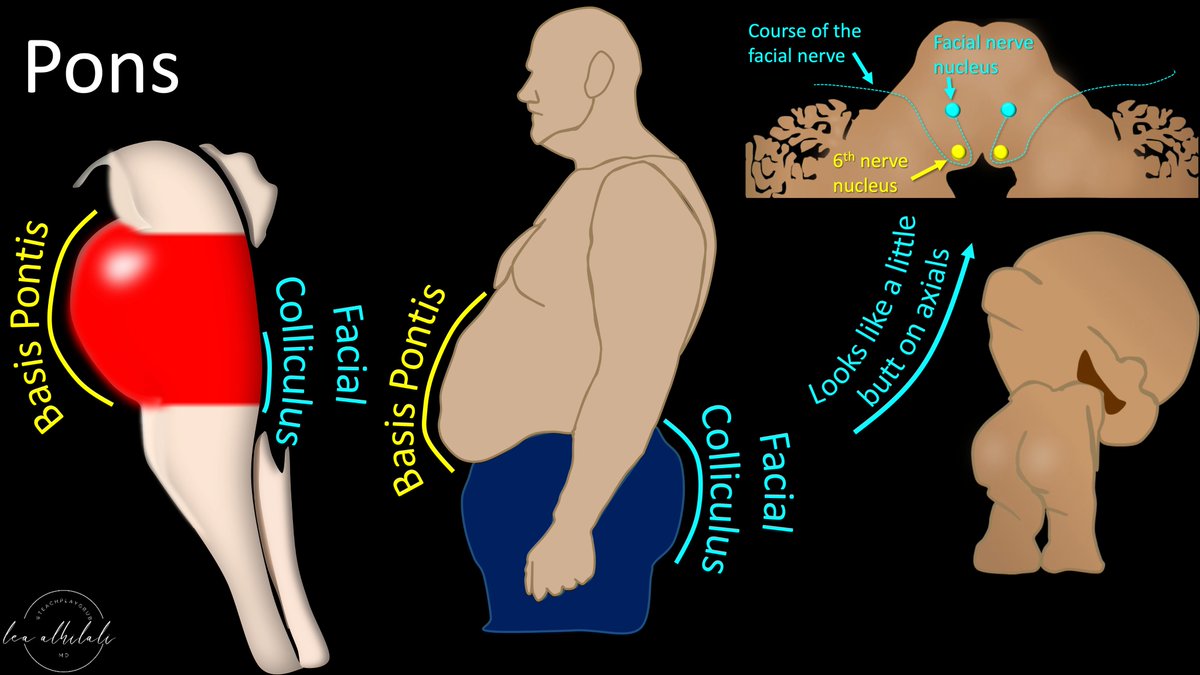
5/Next is the pons.
Dad potbelly is the basis pontis.
Dad’s butt is the facial colliculus—where the facial nerve bulges out as it goes around, behind the 6th nerve nucleus.
Facial colliculus looks like two little baby butt cheeks on the axial images as well!
Dad potbelly is the basis pontis.
Dad’s butt is the facial colliculus—where the facial nerve bulges out as it goes around, behind the 6th nerve nucleus.
Facial colliculus looks like two little baby butt cheeks on the axial images as well!
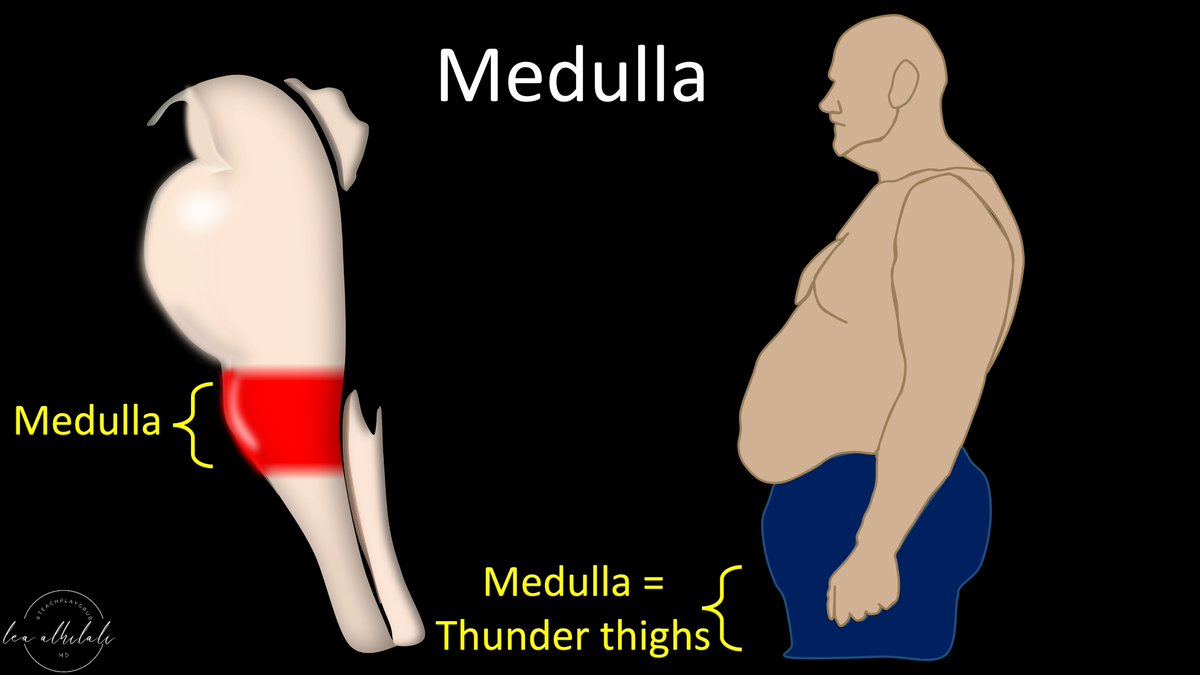
6/Finally, is the medulla, which are the dad’s thunder thighs before heading down into the thinner legs of the spinal cord.
7/You can see this dad bod looking at the brainstem from the front too.
You have the head of the midbrain, which then bulges as you go down into the pons/potbelly
It then narrows as it goes down into the medulla/hips
You have the head of the midbrain, which then bulges as you go down into the pons/potbelly
It then narrows as it goes down into the medulla/hips
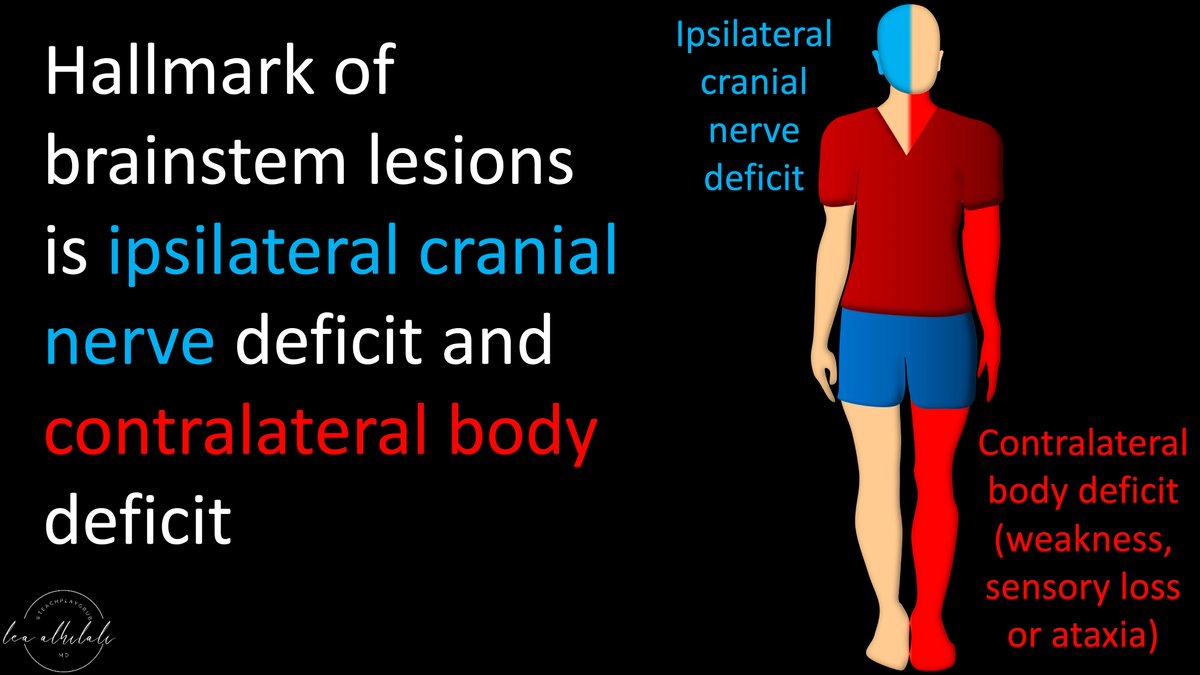
8/The hallmark of a brainstem lesion/syndrome is an ipsilateral cranial nerve deficit & contralateral body deficit (be it weakness, sensory loss, or ataxia)
9/You can remember this split b/c it common that your head wants to do one thing (work out) but your body feels like doing another (relaxing).
So it is not uncommon that things in the head & neck (cranial nerves) will be the opposite of the body
So it is not uncommon that things in the head & neck (cranial nerves) will be the opposite of the body
10/This is true not only for motor (ie, exercising), but also for sensory.
Often your head has certain feelings that do not match up with the feelings in your heart/body.
This split between head and body is key for recognizing brainstem syndromes
Often your head has certain feelings that do not match up with the feelings in your heart/body.
This split between head and body is key for recognizing brainstem syndromes
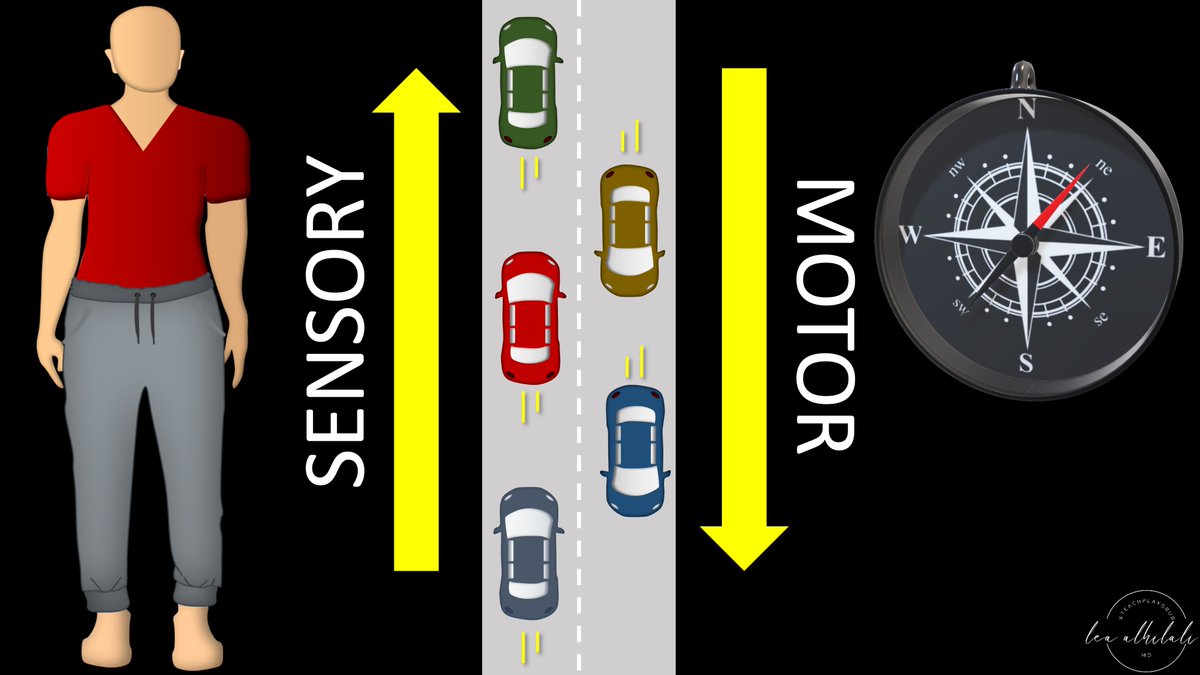
11/Brainstem is basically a highway between the brain & spinal cord.
Motor information is traveling south on the highway to the cord & sensory information is traveling north from the cord to the brain
Motor information is traveling south on the highway to the cord & sensory information is traveling north from the cord to the brain
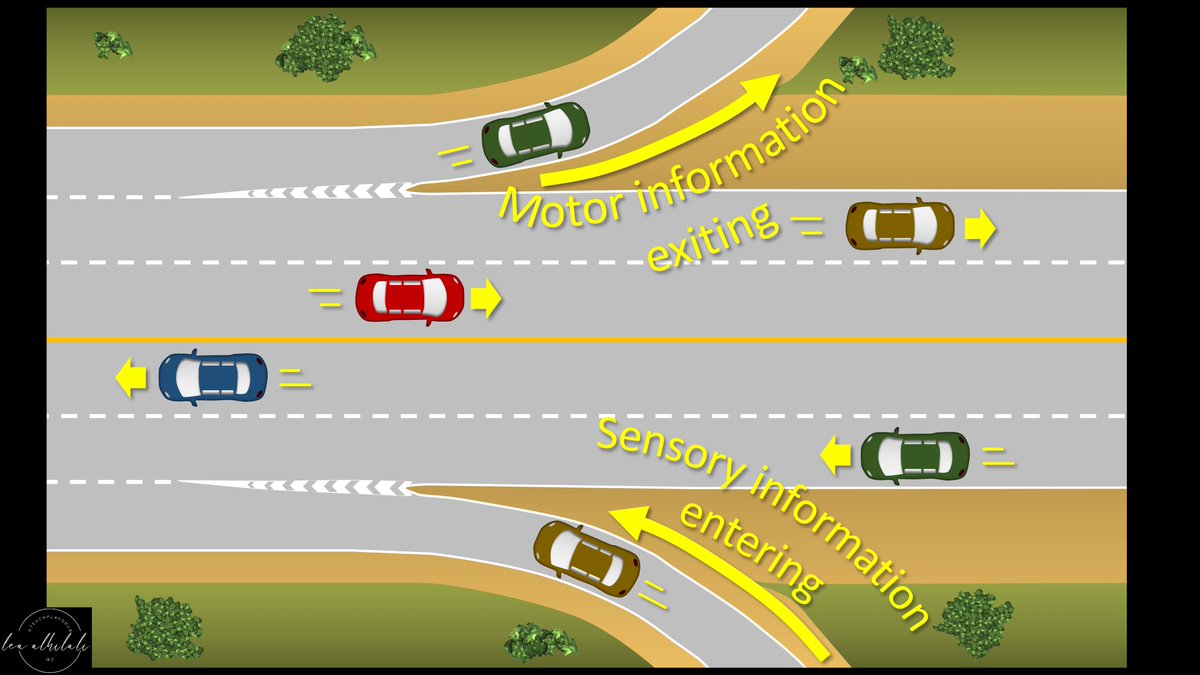
12/Like any highway, there are on ramps & off ramps.
Motor information exits at the off ramps & sensory information comes in through the on ramps.
These on ramps & exits in the brainstem are the cranial nerves
Motor information exits at the off ramps & sensory information comes in through the on ramps.
These on ramps & exits in the brainstem are the cranial nerves
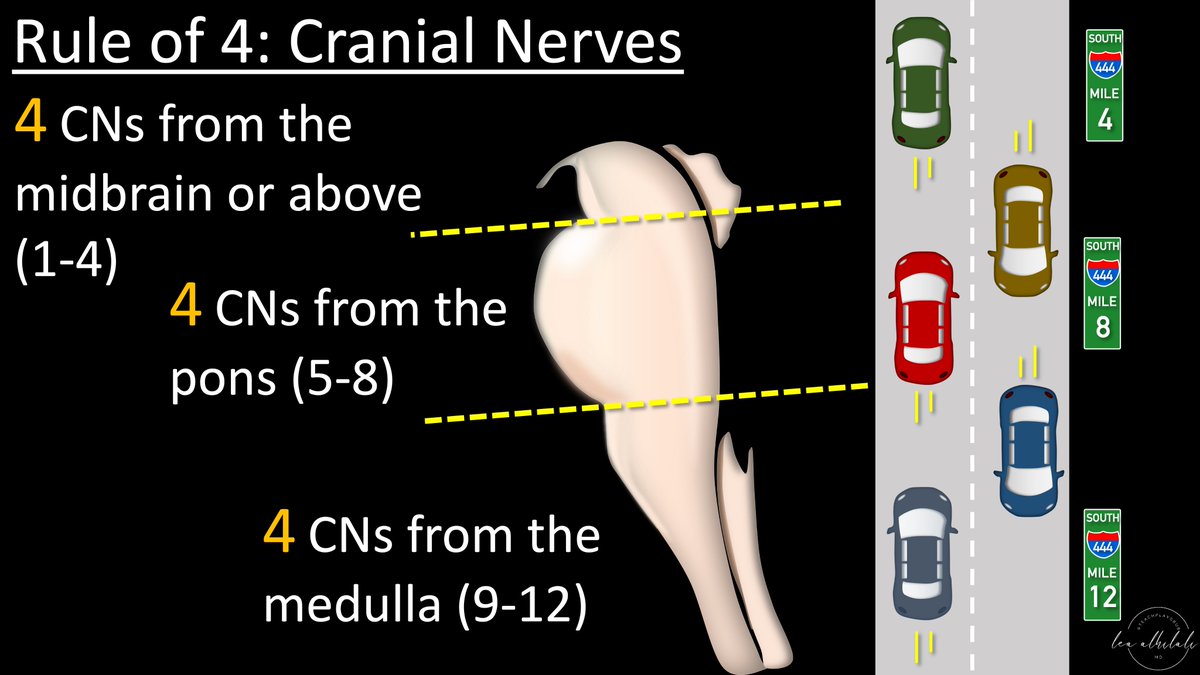
13/On a highway, we know where we are by what exit we are near—they act like mile markers.
We localize how far we are on the highway by the exit we are at.
Same w/the brainstem. We know where we are in the brainstem by which exit or cranial nerve we are near
We localize how far we are on the highway by the exit we are at.
Same w/the brainstem. We know where we are in the brainstem by which exit or cranial nerve we are near

14/We know where the brainstem exits are using the rule of 4s:
There are 4 CNs in each section (medulla, pons, & above the pons).
Counting up from 12, we can see that 9-12 are in the medulla, 5-8 in the pons, and 3 & 4 in the midbrain (1&2 are supratentorial)
There are 4 CNs in each section (medulla, pons, & above the pons).
Counting up from 12, we can see that 9-12 are in the medulla, 5-8 in the pons, and 3 & 4 in the midbrain (1&2 are supratentorial)
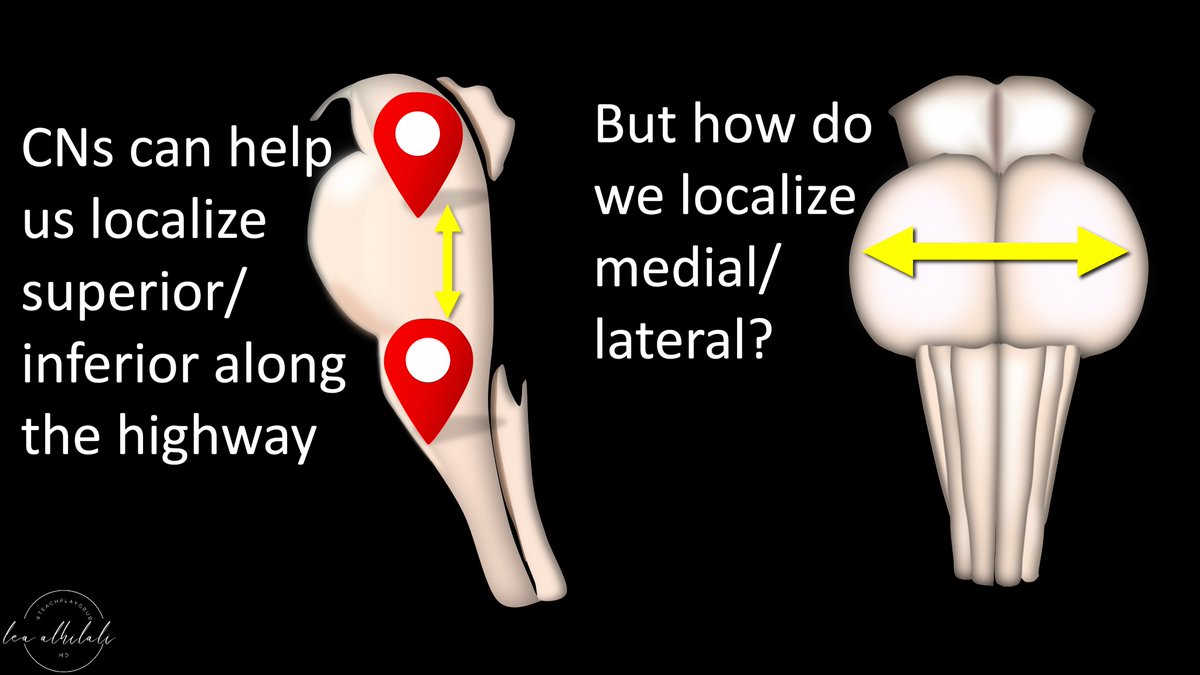
15/Determining which CN is involved by a lesion & using the rule of 4s can tell us where we are in the brainstem top to bottom.
But how do we localize in the transverse plane (medial or lateral)?
But how do we localize in the transverse plane (medial or lateral)?
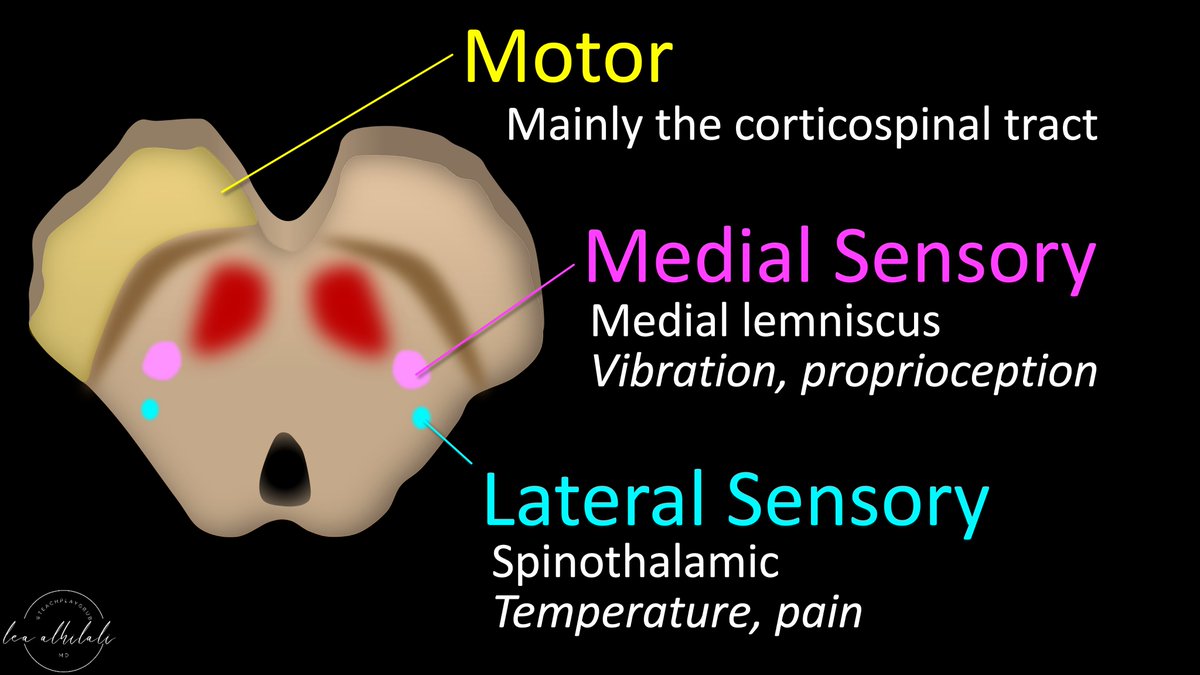
16/We can do this by determining whether it involves the motor tracts or the two major sensory tracts: the medial lemniscus, well medially, and the spinothalamic tract laterally.
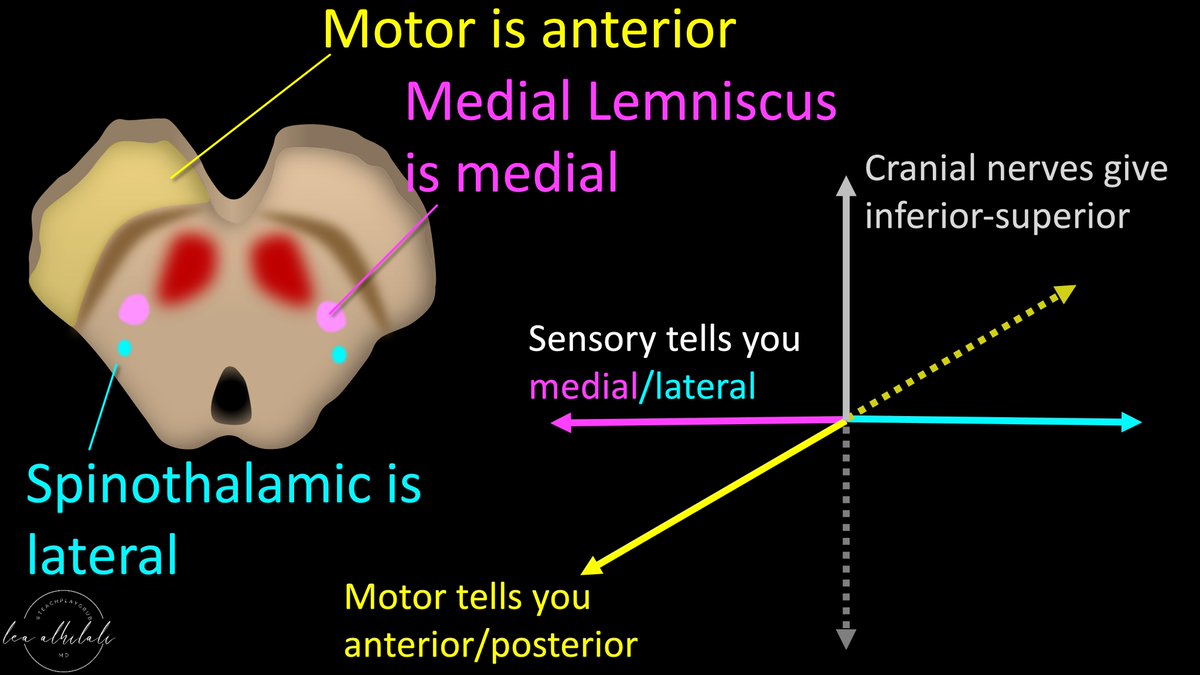
17/Motor is anterior.
Motor involvement tells you if the lesion is anterior or posterior.
Medial lemniscus is medial, so its involvement suggests medial location, while spinothalamic injury suggests lateral location.
Together w/CN involvement, you can now localize in 3 planes
Motor involvement tells you if the lesion is anterior or posterior.
Medial lemniscus is medial, so its involvement suggests medial location, while spinothalamic injury suggests lateral location.
Together w/CN involvement, you can now localize in 3 planes
18/You can remember motor is anterior b/c that’s where motors are usually in a car.
So motor involvement equals an anterior lesion, while sparing of it suggests a more posterior location
So motor involvement equals an anterior lesion, while sparing of it suggests a more posterior location
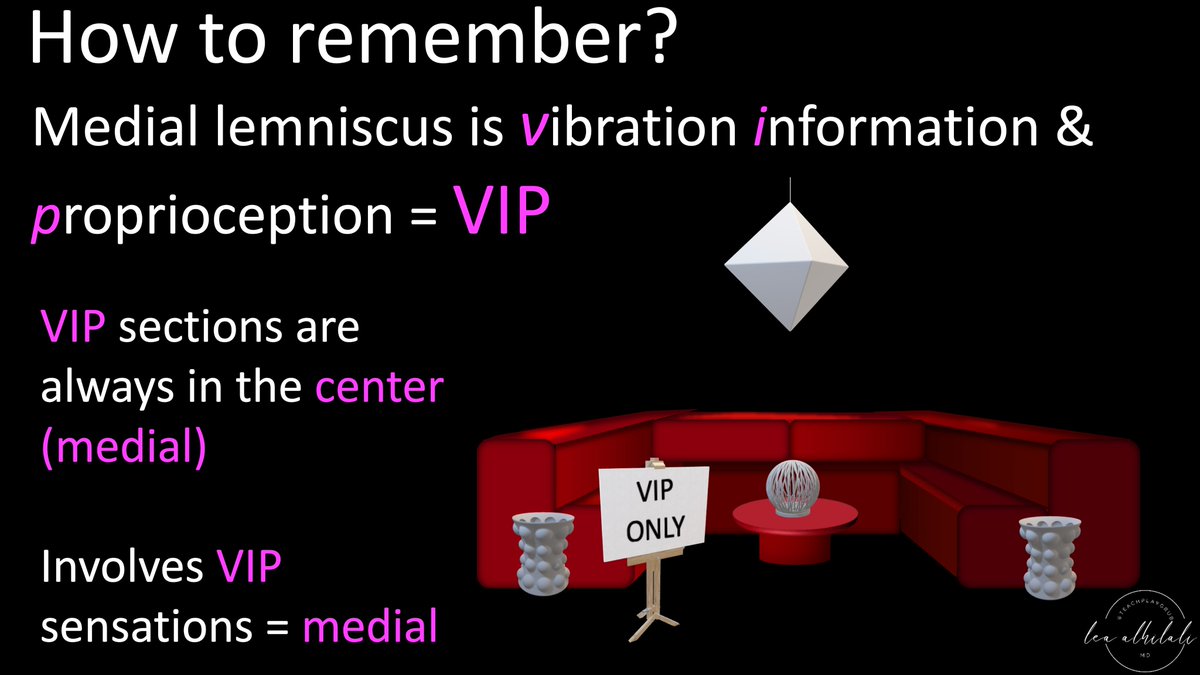
19/How to remember which sensory deficits are medial & which are lateral?
Well, medial lemniscus is vibration information & proprioception. I abbreviate it VIP—& all VIPs are the center of attention (center = medial), so vibration & proprioception loss indicates medial location
Well, medial lemniscus is vibration information & proprioception. I abbreviate it VIP—& all VIPs are the center of attention (center = medial), so vibration & proprioception loss indicates medial location
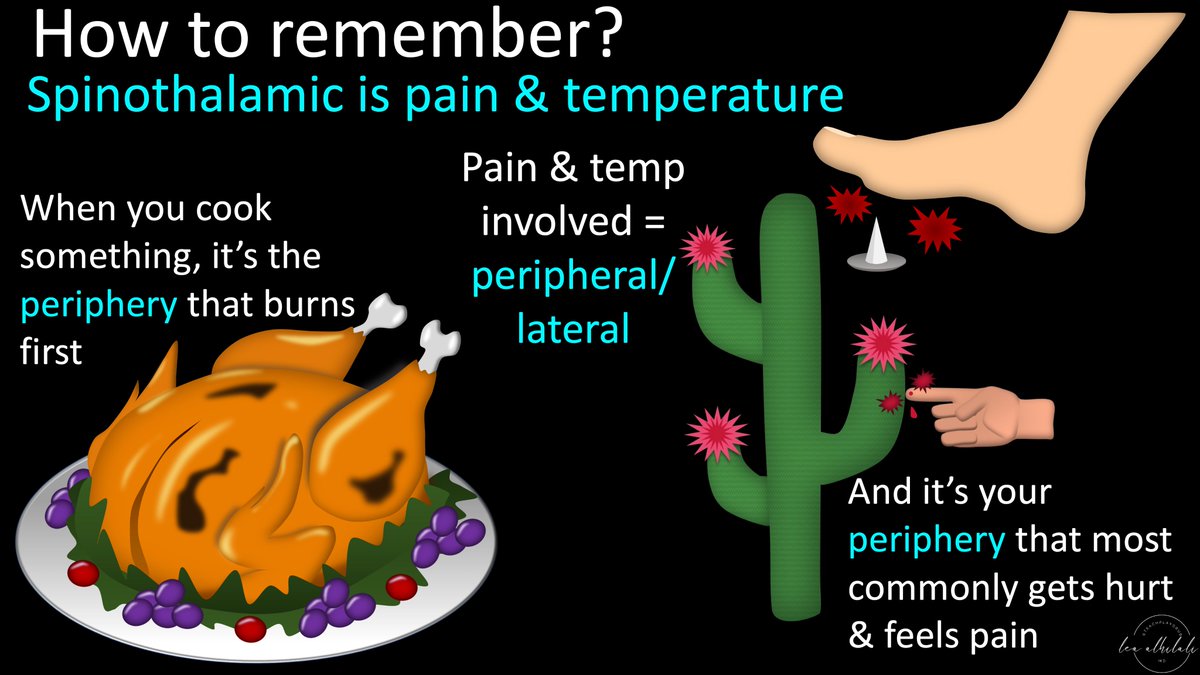
20/Spinothalamic is pain & temperature.
You can remember that w/temperature, the first thing that burns is the skin or periphery—so temperature is peripheral or lateral.
Same w/pain—it is always your extremities or periphery that get hurt, so pain is peripheral/lateral
You can remember that w/temperature, the first thing that burns is the skin or periphery—so temperature is peripheral or lateral.
Same w/pain—it is always your extremities or periphery that get hurt, so pain is peripheral/lateral
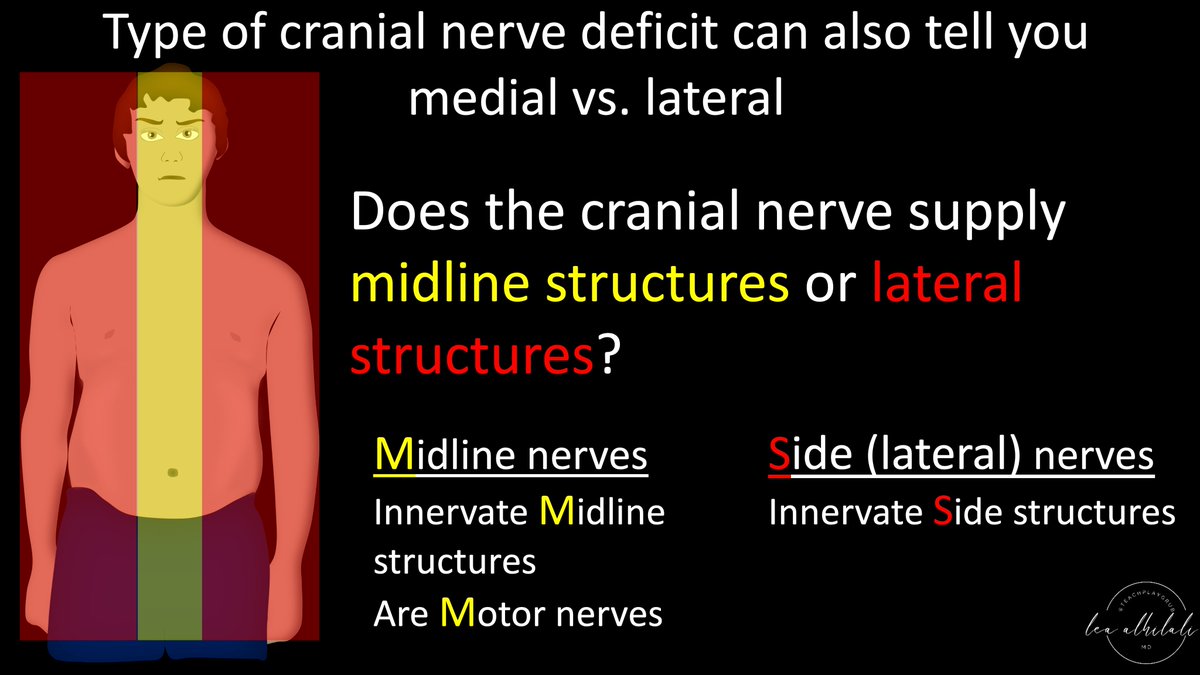
21/CN involvement also indicates medial or lateral position.
CNs located in the midline innervate midline structures.
CNs located laterally in the brainstem innervate lateral structures.
So yourself ask—does the CN involved innervate medial or lateral structures?
CNs located in the midline innervate midline structures.
CNs located laterally in the brainstem innervate lateral structures.
So yourself ask—does the CN involved innervate medial or lateral structures?
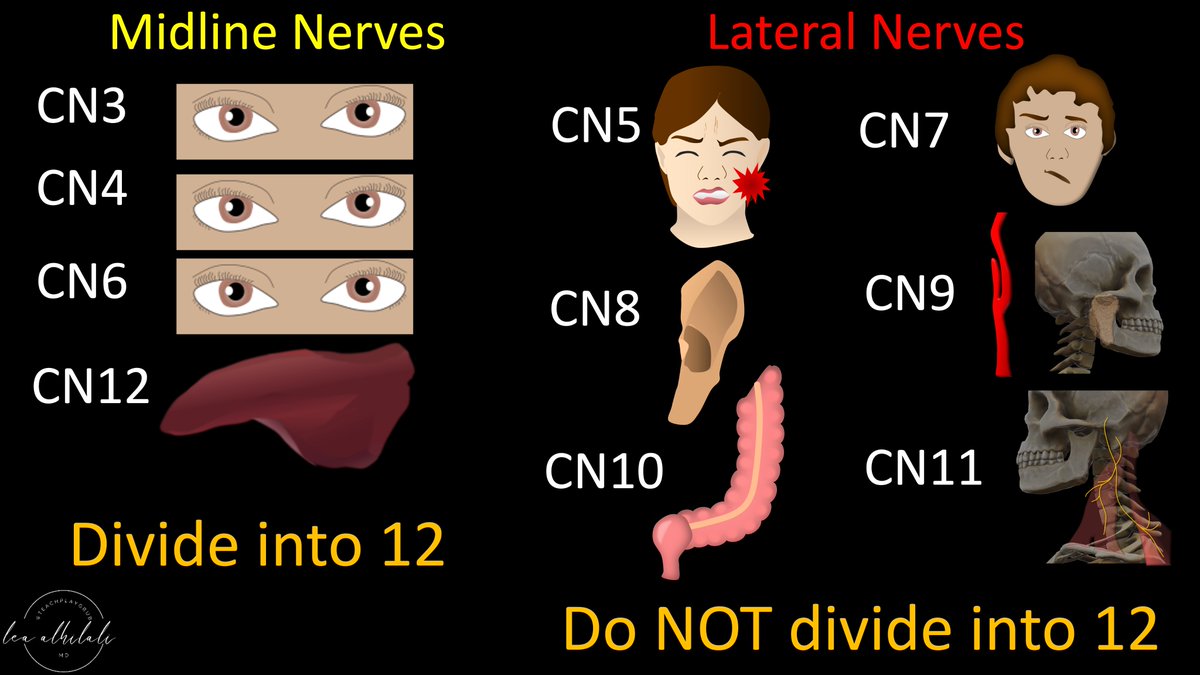
22/Medial structures are eyes & tongue.
All other CNs innervate a lateral object (lat face, ear, parotid, carotid, abdom viscera, shoulder musc)
If CN innervates eyes/tongue, it’s medial in the brainstem—& is also divisible into 12.
Opposite is true for lateral located CNs
All other CNs innervate a lateral object (lat face, ear, parotid, carotid, abdom viscera, shoulder musc)
If CN innervates eyes/tongue, it’s medial in the brainstem—& is also divisible into 12.
Opposite is true for lateral located CNs
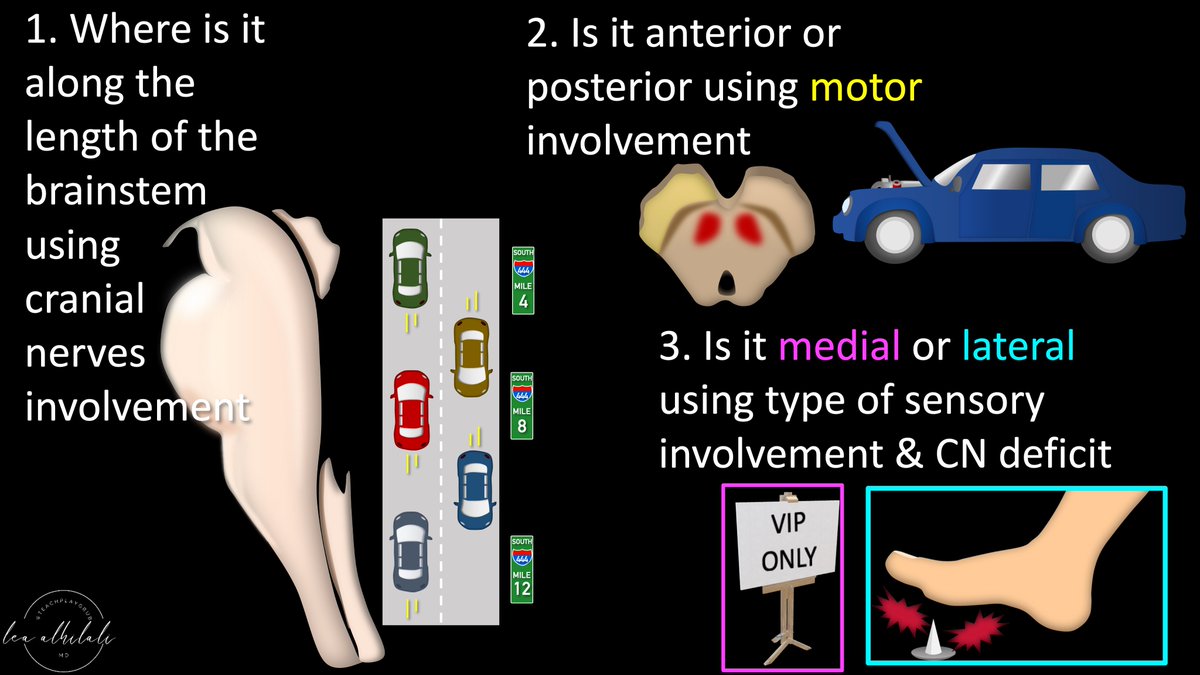
23/So for every brainstem lesion, do 3 things:
1. Find where it is along the length of the brainstem using CN involvement
2. Determine if it’s ant or post based on whether motor is involved
3. Determine if it’s med or lat based on type of sensory deficit & CN involvement
1. Find where it is along the length of the brainstem using CN involvement
2. Determine if it’s ant or post based on whether motor is involved
3. Determine if it’s med or lat based on type of sensory deficit & CN involvement
24/Now you can localize brainstem lesions in all 3 planes based on their clinical presentation!
Hopefully now when confronted w/a brainstem syndrome, you will no longer be locked in, but instead handle it like a VIP!
Hopefully now when confronted w/a brainstem syndrome, you will no longer be locked in, but instead handle it like a VIP!

• • •
Missing some Tweet in this thread? You can try to
force a refresh