🧵1/
Many try to monitor LV function using #POCUS or #EchoFirst, but echo does not work for monitoring.
Let's understand why #POCUS fails at monitoring LV function and how #AutoMAPSE can help.
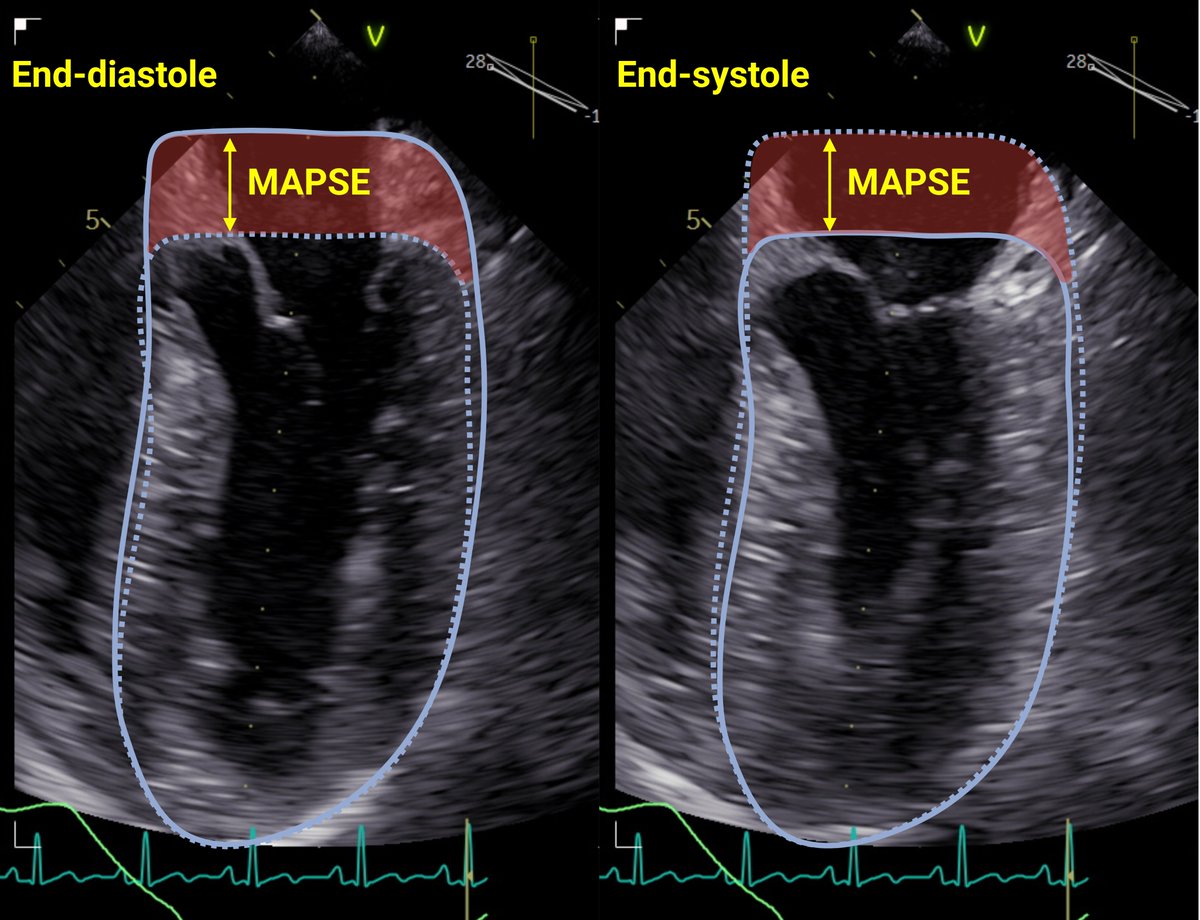
#MAPSE
🔓
@JcmcSoMe #FOAMcc #FOAMed #CardioTwitter rdcu.be/dw7fT

Many try to monitor LV function using #POCUS or #EchoFirst, but echo does not work for monitoring.
Let's understand why #POCUS fails at monitoring LV function and how #AutoMAPSE can help.
#MAPSE
🔓
@JcmcSoMe #FOAMcc #FOAMed #CardioTwitter rdcu.be/dw7fT

2/
The goal of monitoring is
1⃣to detecting small and early changes
2⃣so that therapies can help patients.
For successful monitoring, the measurements must be precise and acquired rapidly and effortlessly. Neither #EchoFirst nor #POCUS fulfil these criteria.
The goal of monitoring is
1⃣to detecting small and early changes
2⃣so that therapies can help patients.
For successful monitoring, the measurements must be precise and acquired rapidly and effortlessly. Neither #EchoFirst nor #POCUS fulfil these criteria.
3/
Eyeballing is rapid, effortless, and OK for diagnosing LV dysfunction.
But eyeballing is NOT precise because it categorises LV function.
Changes in LVEF from 45 to 30% are important, yet still in the same category ➡️ undetectable by categorical assessment.
Eyeballing is rapid, effortless, and OK for diagnosing LV dysfunction.
But eyeballing is NOT precise because it categorises LV function.
Changes in LVEF from 45 to 30% are important, yet still in the same category ➡️ undetectable by categorical assessment.
4/
The monitored measurements must be quantitative to be precise.
Manual measurements in #EchoFirst are quantitative, but human variability still render them imprecise.
📜
Imprecision causes 2⃣ problems during monitoring. rdcu.be/dw7fT
The monitored measurements must be quantitative to be precise.
Manual measurements in #EchoFirst are quantitative, but human variability still render them imprecise.
📜
Imprecision causes 2⃣ problems during monitoring. rdcu.be/dw7fT

5/
Problem1⃣: Busy doctors may be fooled by imprecision.
Its easy to misinterpret random changes as real and react to this randomness with interventions. Of course, the patient has no chance of benefitting from those interventions, and can only be harmed.
Problem1⃣: Busy doctors may be fooled by imprecision.
Its easy to misinterpret random changes as real and react to this randomness with interventions. Of course, the patient has no chance of benefitting from those interventions, and can only be harmed.
6/
Problem2⃣: When we use imprecise tools like #POCUS, we need much larger changes to be confident that the observed changes are real. Changes of that magnitude tend to be clinically obvious. Also, they tend to occur late. Either way, the point of monitoring is lost.
Problem2⃣: When we use imprecise tools like #POCUS, we need much larger changes to be confident that the observed changes are real. Changes of that magnitude tend to be clinically obvious. Also, they tend to occur late. Either way, the point of monitoring is lost.
7/
Precision is always improved by averaging several measurements. Unfortunately, this requires more tedious measurements and is seldomly done in real life. #AutoMAPSE can easily take several measurements of LV function and improve the precision needed for effective monitoring.
Precision is always improved by averaging several measurements. Unfortunately, this requires more tedious measurements and is seldomly done in real life. #AutoMAPSE can easily take several measurements of LV function and improve the precision needed for effective monitoring.

8/
Monitoring must be effortless, and #POCUS/#Echofirst is not. Manual measurements takes too much effort. This effort is better spent on important decision-making.
Monitoring must be effortless, and #POCUS/#Echofirst is not. Manual measurements takes too much effort. This effort is better spent on important decision-making.
9/
#AutoMAPSE alleviates the effort in quantifying LV function by using AI. #AutoMAPSE also reduces the effort in image acquisition by using #TEE.
📜
This even allows for continuous, hands-free imaging: rdcu.be/dw7fT
#AutoMAPSE alleviates the effort in quantifying LV function by using AI. #AutoMAPSE also reduces the effort in image acquisition by using #TEE.
📜
This even allows for continuous, hands-free imaging: rdcu.be/dw7fT
https://twitter.com/dritsyk/status/1711267015195836636

10/
Finally, LV function must also be quantified rapidly.
Measurements by #EchoFirst or #POCUS are too slow for #ICU, where changes in LV function can occur very fast. #AutoMAPSE helps by providing instantaneous measurements.
📜rdcu.be/dw7fT
Finally, LV function must also be quantified rapidly.
Measurements by #EchoFirst or #POCUS are too slow for #ICU, where changes in LV function can occur very fast. #AutoMAPSE helps by providing instantaneous measurements.
📜rdcu.be/dw7fT
11/
Effective monitoring of LV function requires precise, rapid and effortless measurements. Current practices fails to achieve this in #CriticalCare.
Our paper show that #autoMAPSE can rapidly quantify LV function and fill this need. #MAPSE
📜 rdcu.be/dw7fT
Effective monitoring of LV function requires precise, rapid and effortless measurements. Current practices fails to achieve this in #CriticalCare.
Our paper show that #autoMAPSE can rapidly quantify LV function and fill this need. #MAPSE
📜 rdcu.be/dw7fT

unroll @threadreaderapp
• • •
Missing some Tweet in this thread? You can try to
force a refresh