I wanted to share a few slides from my talk @dropthedisorder on Wednesday.
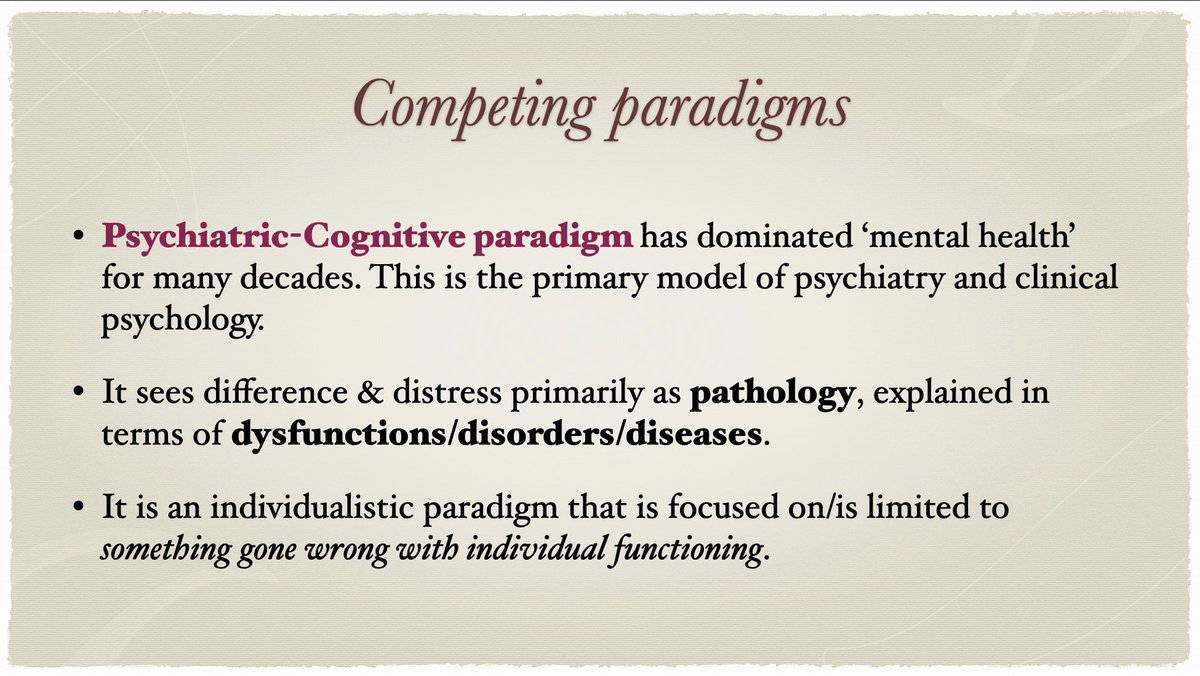
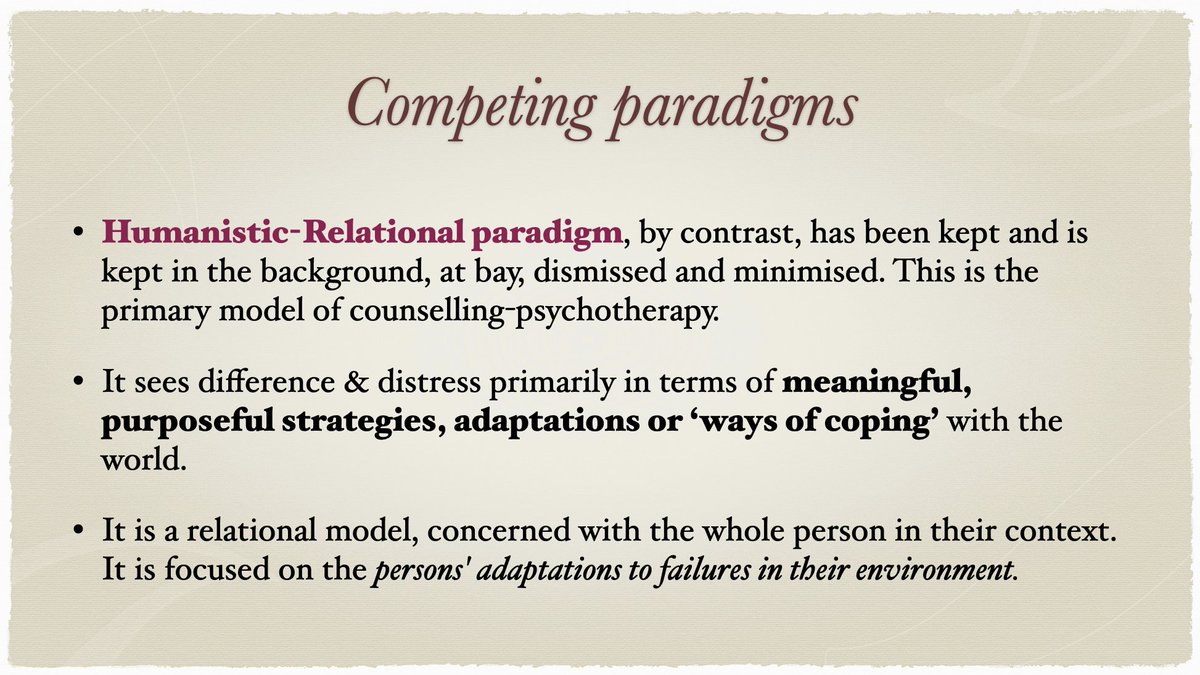
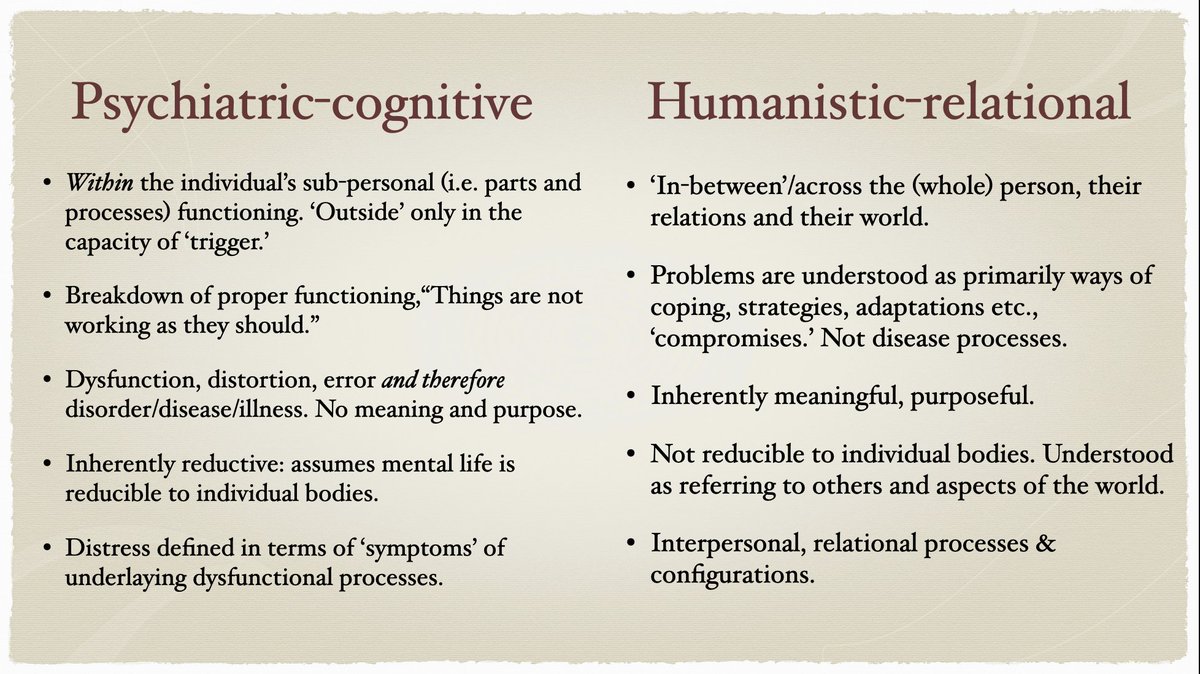
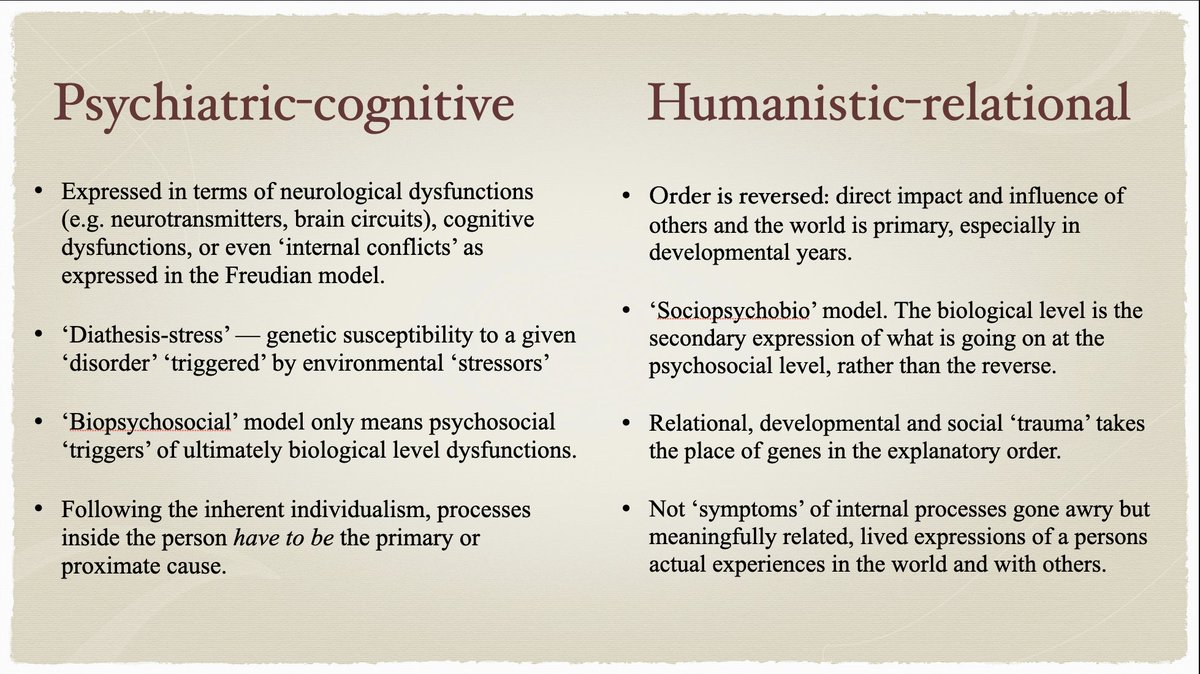
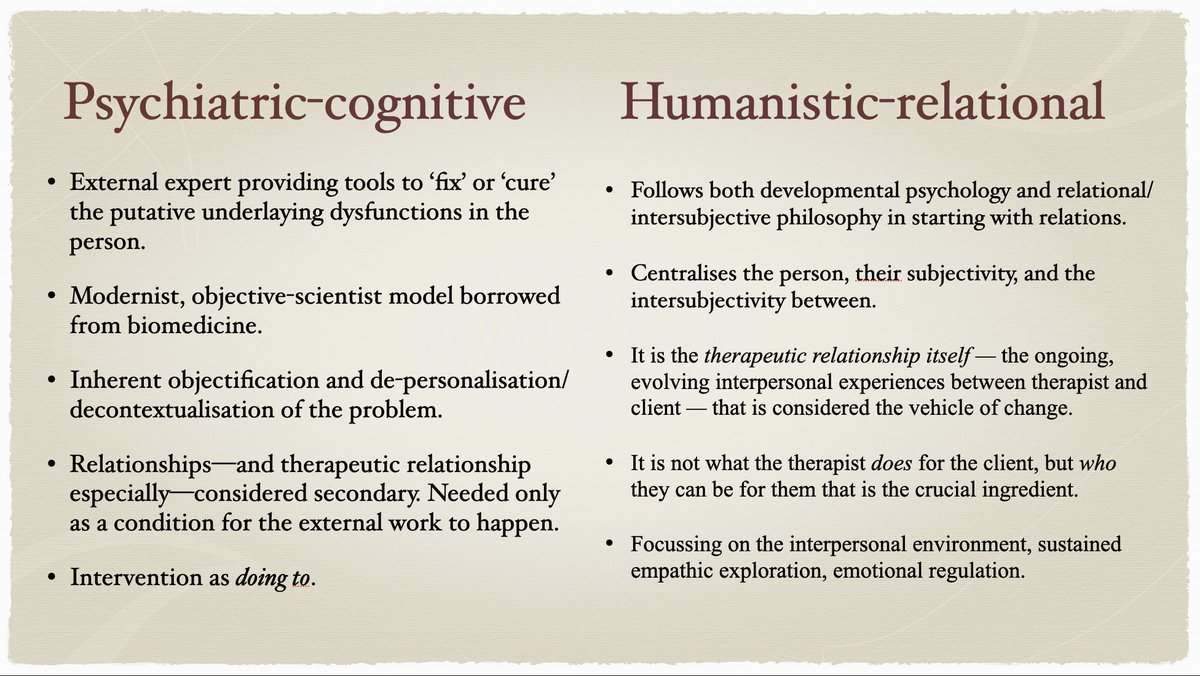
These give definition to what I call the 'Psychiatric-Cognitive' paradigm of psychiatry & cognitive clinical psychology, and the 'Humanistic-Relational' one of counselling-psychotherapy (1/5)
These give definition to what I call the 'Psychiatric-Cognitive' paradigm of psychiatry & cognitive clinical psychology, and the 'Humanistic-Relational' one of counselling-psychotherapy (1/5)
• • •
Missing some Tweet in this thread? You can try to
force a refresh