Apparently many in the Canadian ID community on this platform are weighing in that paxlovid should no longer be recommended to high-risk (elderly, immunocompromised) outpatients with confirmed covid.
I think we should take a look at the evidence they've presented.
(a thread)
1/
I think we should take a look at the evidence they've presented.
(a thread)
1/
https://twitter.com/TheSGEM/status/1760696149592207733
So far there has been no evidence presented, none, except for the blogpost posted in the first tweet.
No peer reviewed science. At all.
And a reminder that there are still >500 inpts in Alberta with covid, and 10-20 patients dying each week (all likely high risk patients).
2/
No peer reviewed science. At all.
And a reminder that there are still >500 inpts in Alberta with covid, and 10-20 patients dying each week (all likely high risk patients).
2/
Another reminder is I reviewed the paxlovid evidence in a thread a few weeks ago, in response to a paxlovid-minimizing news story by @LaurenPelley of @CBCNews.
You can check out the thread here:
3/
You can check out the thread here:
3/
https://x.com/jvipondmd/status/1748815723630391702?s=20
So let's dig into the blogpost by @First10EM, and see what evidence is presented. And how it informs the discussion.
4/
first10em.com/paxlovid-evide…
4/
first10em.com/paxlovid-evide…
Before we dive deep, it is important to understand the pt population that is supposed to benefit from paxlovid.
High-risk (elderly, immunocompromised) outpatients with a positive covid test within 5 days of infection onset.
See Alberta criteria here:
5/albertahealthservices.ca/topics/Page177…
High-risk (elderly, immunocompromised) outpatients with a positive covid test within 5 days of infection onset.
See Alberta criteria here:
5/albertahealthservices.ca/topics/Page177…
The TLDR summary of the blogpost is that most of the studies are observational, industry-funded and therefore can't be trusted. So even if there is evidence, it isn't good.
6/
6/
The blog starts with Hammond (2022), the original NEJM trial that started it all.
Zero deaths vs. 7 for placebo.
NNT of 17 for combination of hosp/death. Not bad!
7/ pubmed.ncbi.nlm.nih.gov/35172054/

Zero deaths vs. 7 for placebo.
NNT of 17 for combination of hosp/death. Not bad!
7/ pubmed.ncbi.nlm.nih.gov/35172054/

His strongest evidence for ineffectiveness is of an unpublished study that can be found here:
An RCT that is undeniably negative. There you go! case closed.
8/ classic.clinicaltrials.gov/ct2/show/resul…
An RCT that is undeniably negative. There you go! case closed.
8/ classic.clinicaltrials.gov/ct2/show/resul…
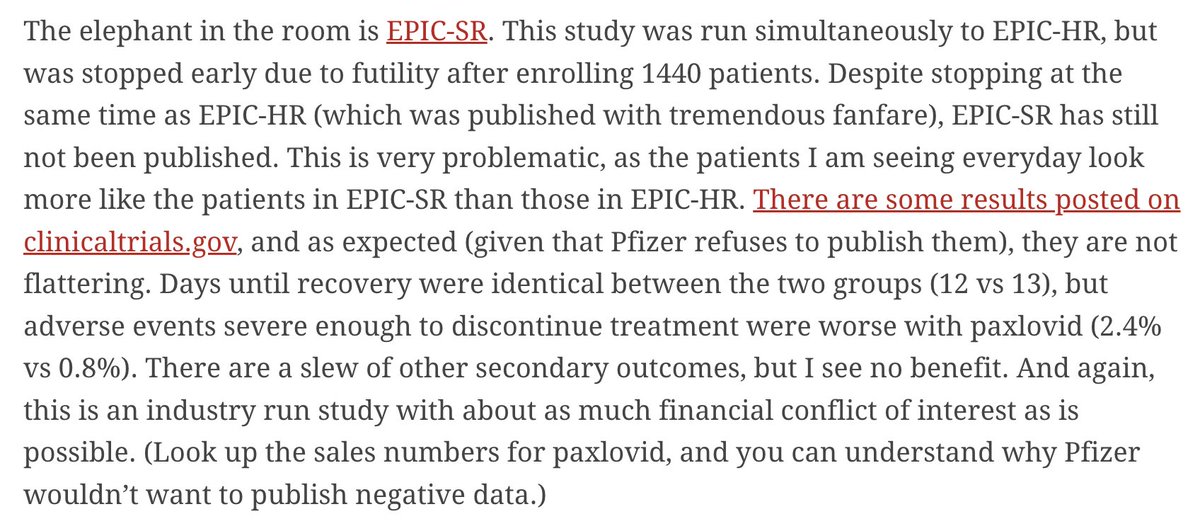
But what was the study population? All comers. Anyone with a positive covid test.
So not the population that we are discussing.
And indeed, many of the observational trials also note the lack of effectiveness in this population.
I would not prescribe Px to this popul'n
9/
So not the population that we are discussing.
And indeed, many of the observational trials also note the lack of effectiveness in this population.
I would not prescribe Px to this popul'n
9/

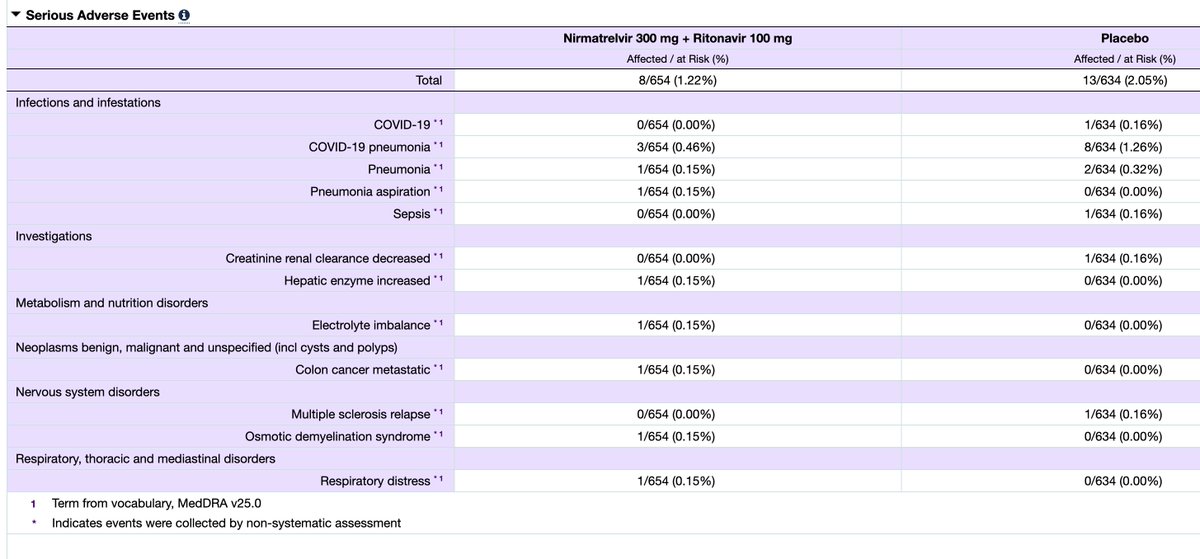
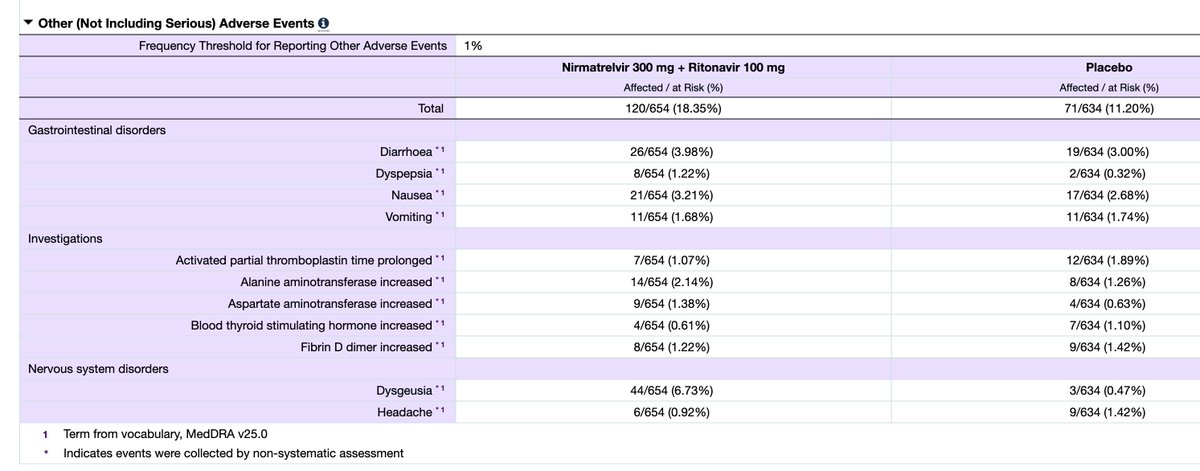
The other criticism is the high # of adverse events in the paxlovid group, some bad enough to cause participants to drop out.
The majority of these were a bad taste in the mouth dysguesia), and upset stomach (dyspepsia).
For serious adverse events, 50% less in Px group.
10/
The majority of these were a bad taste in the mouth dysguesia), and upset stomach (dyspepsia).
For serious adverse events, 50% less in Px group.
10/
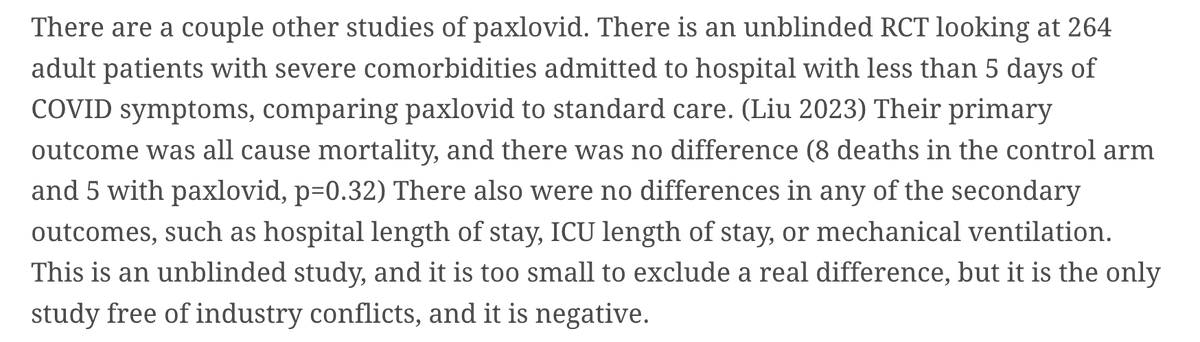
Next negative study is on inpatients.
Again a reminder that there is no evidence for paxlovid in inpatients with COVID.
So this is irrelevant to our patient population.
(see tweet 5).
11/
Again a reminder that there is no evidence for paxlovid in inpatients with COVID.
So this is irrelevant to our patient population.
(see tweet 5).
11/
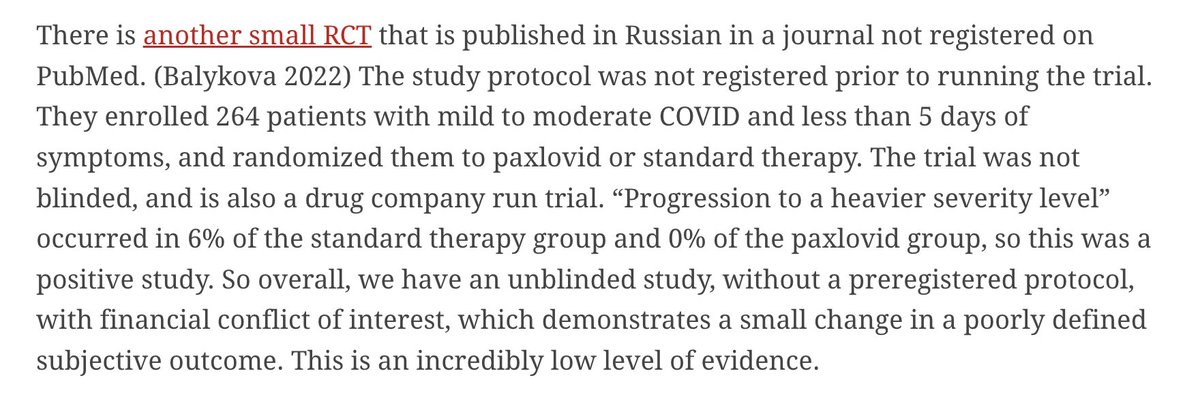
And a 2nd RCT looking at our patient popul'n, positive but deemed irrelevant due to non-blinded, industry funded.
Small effect= NNT of 18 for progression to more severe illness. (seems large to me).
12/
Small effect= NNT of 18 for progression to more severe illness. (seems large to me).
12/
He then focuses on a metanalysis (Tian, 2023) (strangely not in the references but you can find here: )
He states that the effect on death is zero, therefore this is a negative study.
13/pubmed.ncbi.nlm.nih.gov/37485774/
He states that the effect on death is zero, therefore this is a negative study.
13/pubmed.ncbi.nlm.nih.gov/37485774/
But what about the other outcomes?
From the abstract:
"Overall results showed that for death, hospital'n, death or hospital'n, ED visit, ICU admission, and extra oxygen requirement outcomes, every odds ratio (OR) was <1 and p < 0.05."
How is this a -ve metanalysis?
14/
From the abstract:
"Overall results showed that for death, hospital'n, death or hospital'n, ED visit, ICU admission, and extra oxygen requirement outcomes, every odds ratio (OR) was <1 and p < 0.05."
How is this a -ve metanalysis?
14/

So, this -ve blogpost cites 4 RCTs, 2 of which are positive and 2 of which are irrelevant to our patient population.
And a metanalysis that is unequivocably positive, but spun as negative.
This is non-systematic, non-peer reviewed evidence spin
15/
And a metanalysis that is unequivocably positive, but spun as negative.
This is non-systematic, non-peer reviewed evidence spin
15/
So this is the best evidence being used by Canadian ID physicians to withhold a life-saving treatment from atrisk immunocompromised, elderly patients, that continue to die and be hospitalized from COVID-19.
And it is not good.
This is ableism.
16/
And it is not good.
This is ableism.
16/
so it's no wonder that Paxlovid is being underused in the patient population most likely to benefit.
I wonder if the same evidence was available for another non-covid disease, if the rejection would be so strong.
17/ forbes.com/sites/judyston…
I wonder if the same evidence was available for another non-covid disease, if the rejection would be so strong.
17/ forbes.com/sites/judyston…
A CDC analysis suggests that billions of dollars (and many lives and hospitalizations) could be saved with more equitable use of Paxlovid, even in a low transmission scenario.
Please, MDs, rx this med to the at-risk populations that would benefit.
fin/
.wwwnc.cdc.gov/eid/article/30…
Please, MDs, rx this med to the at-risk populations that would benefit.
fin/
.wwwnc.cdc.gov/eid/article/30…
@davidcarr333 @BogochIsaac @TheSGEM @First10EM @DrToddLee @sumona24 @LaurenPelley @AntibioticDoc feel free to weigh in.
@threadreaderapp unroll please
• • •
Missing some Tweet in this thread? You can try to
force a refresh