🚨NEW Report presents findings from a review of Long Covid to guide New Zealand’s Public Health response.
Report concludes that “preventative action is urgently needed”.
Let’s dive into the details as the findings are relevant for ALL countries.
🔗
/1 phcc.org.nz/briefing/long-…

Report concludes that “preventative action is urgently needed”.
Let’s dive into the details as the findings are relevant for ALL countries.
🔗
/1 phcc.org.nz/briefing/long-…

Below are some of the key findings of the report:
▪️Changes in health status following SARS-CoV-2 infection are common and can occur at any age.
▪️Symptoms are frequently experienced for months or years and can increase over time.
/2
▪️Changes in health status following SARS-CoV-2 infection are common and can occur at any age.
▪️Symptoms are frequently experienced for months or years and can increase over time.
/2

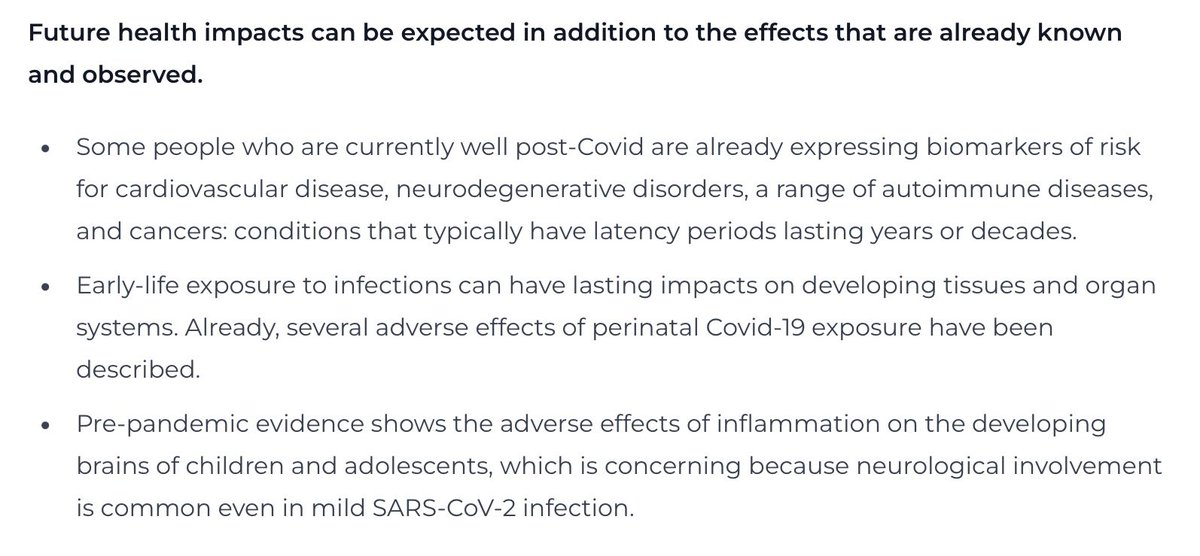
▪️Future health impacts can be expected in addition to the effects that are already observed.
▪️ Some people who are currently well post-Covid are already expressing biomarkers of risk for cardiovascular disease, neurodegenerative disorders, autoimmune diseases & cancers.
/3
▪️ Some people who are currently well post-Covid are already expressing biomarkers of risk for cardiovascular disease, neurodegenerative disorders, autoimmune diseases & cancers.
/3
▪️Society, sector & workforce effects of Long Covid are costly and disruptive, and they worsen existing inequities.
▪️ The frequency of (often undiagnosed) cognitive impairment after a mild infection indicates a need for risk assessment of impacts on occupational safety.
/4
▪️ The frequency of (often undiagnosed) cognitive impairment after a mild infection indicates a need for risk assessment of impacts on occupational safety.
/4

▪️Because of rapid viral evolution, Covid-19 waves are not showing a consistent pattern of improvement over time.
▪️Without intervention to reduce cases, the prevalence of Long Covid is more likely to increase than to decrease.
/5
▪️Without intervention to reduce cases, the prevalence of Long Covid is more likely to increase than to decrease.
/5

▪️When an infectious disease is common in the population, its long-term effects become common too.
▪️At a population level, modest-looking proportions of a post-infectious health risk readily translate into very large numbers.
/6
▪️At a population level, modest-looking proportions of a post-infectious health risk readily translate into very large numbers.
/6

The report concludes that:
“Our evidence summary strongly suggests that Long Covid is a major threat to individual health, societal wellbeing and economic performance.”
/7
“Our evidence summary strongly suggests that Long Covid is a major threat to individual health, societal wellbeing and economic performance.”
/7

The Appendix of the report expands further on this important point:
“Choosing to ignore potential harms is indefensible when the risk can be reduced using a combination of new knowledge and well-established public-health approaches.”
/8
“Choosing to ignore potential harms is indefensible when the risk can be reduced using a combination of new knowledge and well-established public-health approaches.”
/8

The authors recommend 3 immediate actions:
▪️Conducting a comprehensive Long Covid risk assessment.
▪️Rapidly reduce infection & reinfection rates using well-established public health & social measures.
▪️Expand Covid-19 vaccine eligibility and coverage.
/9
▪️Conducting a comprehensive Long Covid risk assessment.
▪️Rapidly reduce infection & reinfection rates using well-established public health & social measures.
▪️Expand Covid-19 vaccine eligibility and coverage.
/9

Appendix 2 provides further details of the proposed components for Covid mitigation, including:
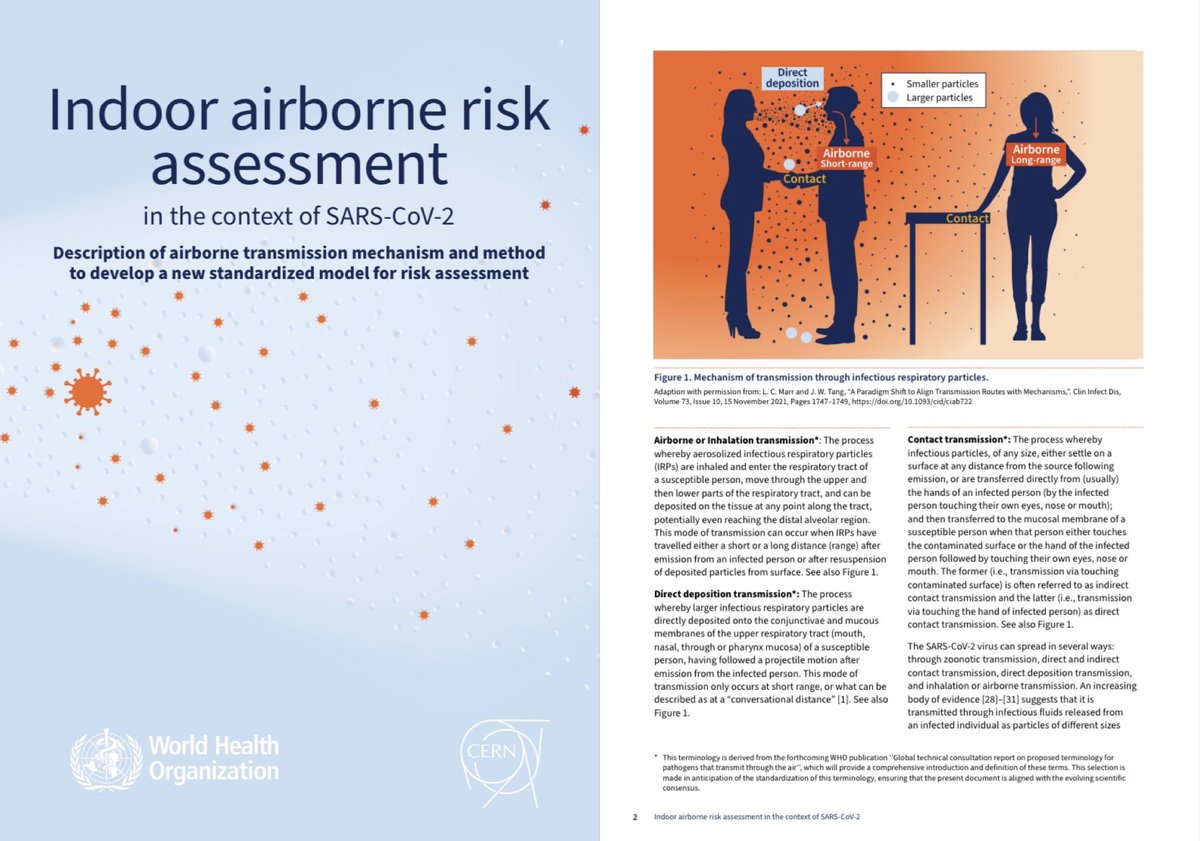
▪️Support for self-isolation of infected cases
▪️Improve indoor air quality
▪️Maintain mask use in high-risk indoor environments eg health care
▪️High & equitable vax coverage
/10
▪️Support for self-isolation of infected cases
▪️Improve indoor air quality
▪️Maintain mask use in high-risk indoor environments eg health care
▪️High & equitable vax coverage
/10

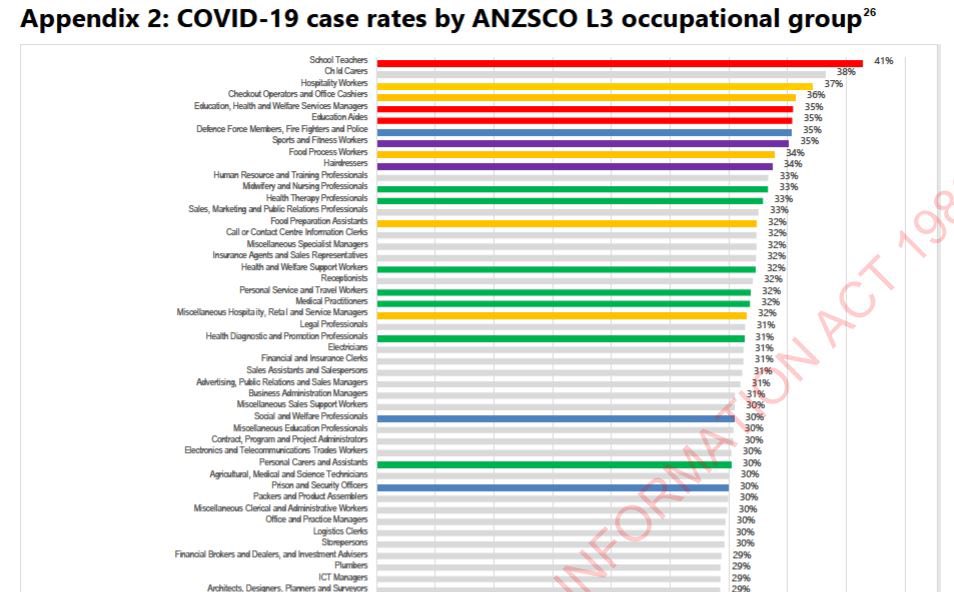
Below is a press article about this report, highlighting the fact that, in terms of occupational risk, teachers are the most vulnerable to getting Covid - and, in turn, most at risk of getting Long Covid.
🔗
/11 rnz.co.nz/news/national/…
🔗
/11 rnz.co.nz/news/national/…

Below is another press article which includes comments from NZ Education Institute president Mark Potter.

Potter revealed that his union had heard from a lot of teachers who were struggling to continue in the profession due to Long Covid.
🔗
/12 rnz.co.nz/news/national/…

Potter revealed that his union had heard from a lot of teachers who were struggling to continue in the profession due to Long Covid.
🔗
/12 rnz.co.nz/news/national/…

The chart of Covid case rates by occupational group can be found in the chart below, showing that teachers are at significantly higher risk of Covid infection than any other occupation.
(Source: )
/13 fyi.org.nz/request/20877/…
(Source: )
/13 fyi.org.nz/request/20877/…
https://twitter.com/amandakvalsvig/status/1772911300525642029
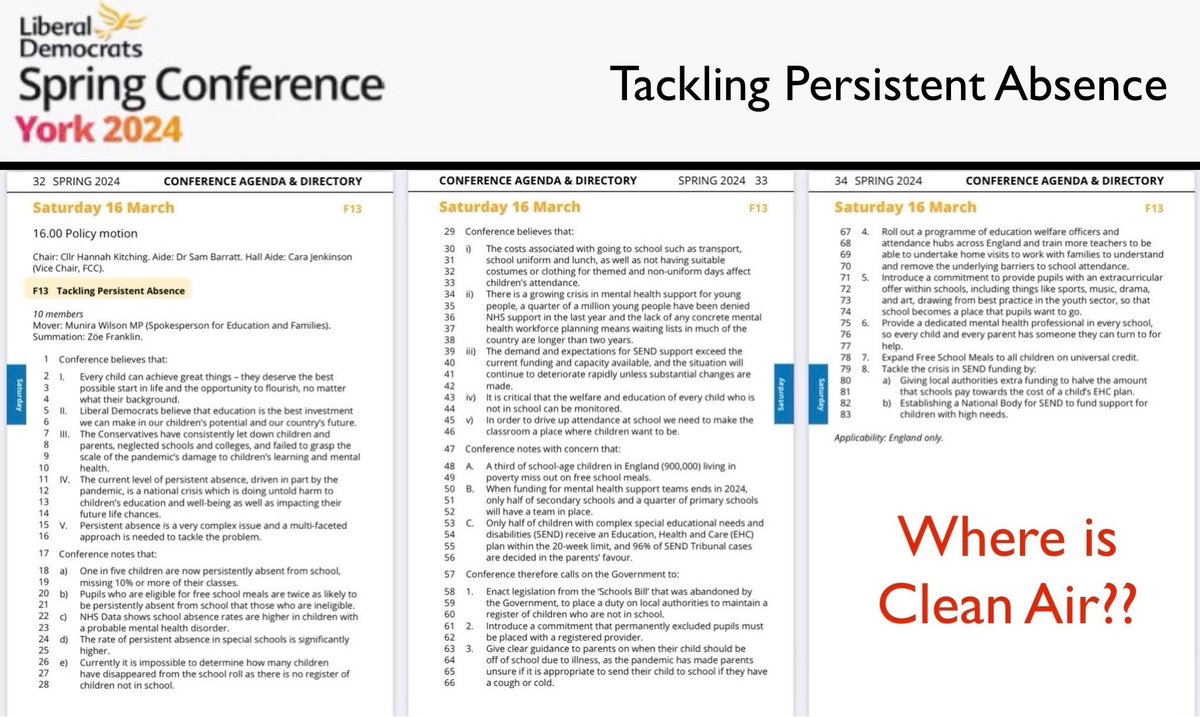
One of the authors, @AmandaKvalsvig, tweeted earlier that schools MUST be made safe since they’re the hubs of their communities, linking public settings & households.
The only effective way to reduce Long Covid is to reduce Covid cases.
Schools are a great place to start.
/14
The only effective way to reduce Long Covid is to reduce Covid cases.
Schools are a great place to start.
/14
https://twitter.com/amandakvalsvig/status/1772911309161431478

In a previous paper (March 2023) also co-authored by @AmandaKvalsvig, she helped outline 7 goals for healthy schools.
As stated in the report, “these actions are highly feasible if the government steps up with a commitment to resource healthy schools.”
/15
As stated in the report, “these actions are highly feasible if the government steps up with a commitment to resource healthy schools.”
/15
https://twitter.com/amandakvalsvig/status/1633911338094432256
This report is a truly outstanding piece of work and could form the blueprint for ANY government willing to confront the enormous health & economic challenges presented by repeated Covid infections and the resulting impact of Long Covid.
🔗
/16 phcc.org.nz/briefing/long-…
🔗
/16 phcc.org.nz/briefing/long-…

Meanwhile, in the UK 🇬🇧, a paper was recently published by @CambridgeEcon on the economic burden of Long Covid.
The report estimates that, if the UK prevalence of Long Covid increases to 4m people by 2030, there will be a £2.7 BILLION loss in GDP & 311k job losses PER YEAR.
17/
The report estimates that, if the UK prevalence of Long Covid increases to 4m people by 2030, there will be a £2.7 BILLION loss in GDP & 311k job losses PER YEAR.
17/
https://twitter.com/cambridgeecon/status/1770388326031282305

In the US 🇺🇸 , detailed evidence on the impact of Long Covid was presented a recent Senate Committee Hearing.
The opening speech below from @BernieSanders provided a compelling summary of the latest research.
More info at this link ⬇️
🔗
/18 sanders.senate.gov/op-eds/us-is-t…
The opening speech below from @BernieSanders provided a compelling summary of the latest research.
More info at this link ⬇️
🔗
/18 sanders.senate.gov/op-eds/us-is-t…
https://twitter.com/luckytran/status/1748025590152593825
And, in Canada 🇨🇦, a recent report from @StatCan_eng revealed that 1 in 9 Canadian adults have experienced the debilitating symptoms of Long Covid.
Of these, 7 in 10 Canadian adults with long term symptoms experience them on a daily or nearly daily basis.
/19
Of these, 7 in 10 Canadian adults with long term symptoms experience them on a daily or nearly daily basis.
/19
https://twitter.com/_catinthehat/status/1734224376206111057
Covid & its longer term impact on our nation’s health is not going away.
‘Living with Covid’ shouldn’t mean just ignoring it.
It should mean making environments as safe as possible so we can all live our lives with less risk… less illness… less absence from school/work.
20/
‘Living with Covid’ shouldn’t mean just ignoring it.
It should mean making environments as safe as possible so we can all live our lives with less risk… less illness… less absence from school/work.
20/

• • •
Missing some Tweet in this thread? You can try to
force a refresh