Translation of excerpt from September 2019 executive order:
"New platform needed - old platform not working/causing problems"
and/or
"Excuse needed to launch new platform"
➡️ Operation COVID-19
trumpwhitehouse.archives.gov/presidential-a…
"New platform needed - old platform not working/causing problems"
and/or
"Excuse needed to launch new platform"
➡️ Operation COVID-19
trumpwhitehouse.archives.gov/presidential-a…

February 28, 2019: Flu Shot Probs
Scientists have invested considerable time in recent years attempting to figure out why egg-grown vaccines seem to lag behind their cell-grown counterparts. Studies have shown that vaccine strains grown in eggs tend to mutate over time.
"Any influenza viruses produced in eggs have to adapt to growing in that environment and hence generate mutations to grow better," said Ian Wilson, DPhil, a professor of structural biology at the Scripps Research Institute, in California, in a press release.
Unfortunately, those adaptations mean the resulting vaccine is optimized to fight the egg-adapted version of influenza, and not necessarily the strain that is active in the area.
Wilson and colleagues published findings documenting the structural underpinnings of this phenomenon in October. Writing in PLOS Pathogens, Wilson and colleagues said the need to move beyond egg-based flu vaccines is urgent.
I'll bet it was. 🚩 cc: @jengleruk
Scientists have invested considerable time in recent years attempting to figure out why egg-grown vaccines seem to lag behind their cell-grown counterparts. Studies have shown that vaccine strains grown in eggs tend to mutate over time.
"Any influenza viruses produced in eggs have to adapt to growing in that environment and hence generate mutations to grow better," said Ian Wilson, DPhil, a professor of structural biology at the Scripps Research Institute, in California, in a press release.
Unfortunately, those adaptations mean the resulting vaccine is optimized to fight the egg-adapted version of influenza, and not necessarily the strain that is active in the area.
Wilson and colleagues published findings documenting the structural underpinnings of this phenomenon in October. Writing in PLOS Pathogens, Wilson and colleagues said the need to move beyond egg-based flu vaccines is urgent.
I'll bet it was. 🚩 cc: @jengleruk

Passaging human viruses in eggs and pushing injections on every man, woman, & child is a bad idea
"SARS-CoV-2" = Decoy in the mRNA platform launch
It wasn't the problem being solved
IMO, the countermeasures weren't for "novel coronavirus" cc: @jjcouey
"SARS-CoV-2" = Decoy in the mRNA platform launch
It wasn't the problem being solved
IMO, the countermeasures weren't for "novel coronavirus" cc: @jjcouey
https://x.com/Wood_House76/status/1736958719563386966?s=20
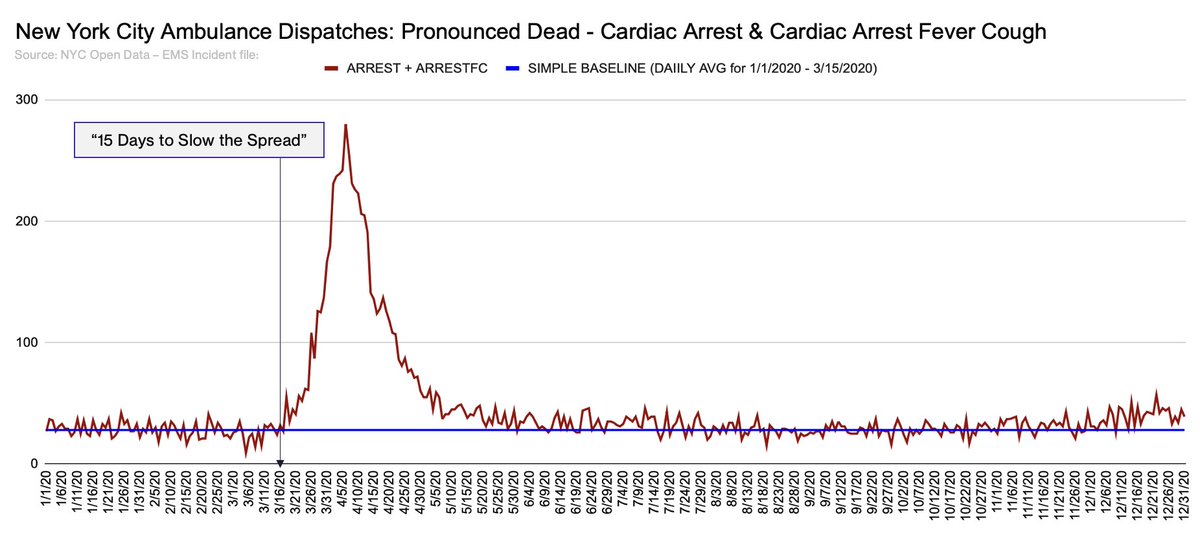
Here's a fun one from March 29, 2020
I'll say it again:
In my opinion, Operation COVID was, in part, an excuse to off-ramp the problematic egg method and launch mRNA
cnn.com/2020/03/27/hea…
I'll say it again:
In my opinion, Operation COVID was, in part, an excuse to off-ramp the problematic egg method and launch mRNA
cnn.com/2020/03/27/hea…

@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh