𝗪𝗵𝗮𝘁 𝗶𝘀 𝗰𝗮𝗻𝗰𝗲𝗿?
Why are we so bad at treating it?
Why do some tumors spontaneously regress?
What can we do to lessen our chances of getting cancer?
𝗧𝗵𝗿𝗲𝗮𝗱
Why are we so bad at treating it?
Why do some tumors spontaneously regress?
What can we do to lessen our chances of getting cancer?
𝗧𝗵𝗿𝗲𝗮𝗱

“𝙄𝙩’𝙨 𝙗𝙚𝙚𝙣 𝙣𝙚𝙖𝙧𝙡𝙮 50 𝙮𝙚𝙖𝙧𝙨 𝙨𝙞𝙣𝙘𝙚 𝙩𝙝𝙚 𝙒𝙖𝙧 𝙤𝙣 𝘾𝙖𝙣𝙘𝙚𝙧 𝙬𝙖𝙨 𝙙𝙚𝙘𝙡𝙖𝙧𝙚𝙙, 𝙖𝙣𝙙 𝙮𝙚𝙩 𝙢𝙤𝙧𝙚 𝙥𝙚𝙤𝙥𝙡𝙚 𝙖𝙧𝙚 𝙙𝙞𝙖𝙜𝙣𝙤𝙨𝙚𝙙 𝙬𝙞𝙩𝙝 𝙘𝙖𝙣𝙘𝙚𝙧 𝙖𝙣𝙙 𝙙𝙮𝙞𝙣𝙜 𝙛𝙧𝙤𝙢 𝙩𝙝𝙚 𝙙𝙞𝙨𝙚𝙖𝙨𝙚 𝙩𝙝𝙖𝙣 𝙚𝙫𝙚𝙧 𝙗𝙚𝙛𝙤𝙧𝙚.[1]
𝘐 𝘧𝘪𝘯𝘥 𝘪𝘵 𝘦𝘹𝘵𝘳𝘢𝘰𝘳𝘥𝘪𝘯𝘢𝘳𝘪𝘭𝘺 𝘥𝘪𝘧𝘧𝘪𝘤𝘶𝘭𝘵 𝘵𝘰 𝘣𝘦𝘭𝘪𝘦𝘷𝘦 𝘵𝘩𝘢𝘵 𝘢𝘧𝘵𝘦𝘳 𝘴𝘱𝘦𝘯𝘥𝘪𝘯𝘨 $500 𝘣𝘪𝘭𝘭𝘪𝘰𝘯 𝘥𝘰𝘭𝘭𝘢𝘳𝘴 𝘰𝘯 𝘤𝘢𝘯𝘤𝘦𝘳 𝘳𝘦𝘴𝘦𝘢𝘳𝘤𝘩 𝘴𝘪𝘯𝘤𝘦 1970,[2] 𝘵𝘩𝘦 𝘤𝘢𝘯𝘤𝘦𝘳 𝘦𝘴𝘵𝘢𝘣𝘭𝘪𝘴𝘩𝘮𝘦𝘯𝘵 𝘩𝘢𝘴 𝘤𝘰𝘮𝘦 𝘶𝘱 𝘸𝘪𝘵𝘩 𝘭𝘪𝘵𝘦𝘳𝘢𝘭𝘭𝘺 𝘯𝘰𝘵𝘩𝘪𝘯𝘨 𝘶𝘴𝘦𝘧𝘶𝘭 𝘧𝘰𝘳 𝘱𝘳𝘦𝘷𝘦𝘯𝘵𝘪𝘯𝘨 𝘰𝘳 𝘤𝘶𝘳𝘪𝘯𝘨 𝘵𝘩𝘦 𝘥𝘪𝘴𝘦𝘢𝘴𝘦. 𝘐𝘧 𝘪𝘵’𝘴 𝘵𝘳𝘶𝘦, 𝘵𝘩𝘦𝘯 𝘵𝘩𝘦𝘺 𝘢𝘳𝘦 𝘪𝘯𝘤𝘰𝘮𝘱𝘦𝘵𝘦𝘯𝘵 𝘢𝘯𝘥 𝘵𝘩𝘦𝘪𝘳 𝘢𝘴𝘵𝘰𝘯𝘪𝘴𝘩𝘪𝘯𝘨 𝘭𝘢𝘤𝘬 𝘰𝘧 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘮𝘦𝘯𝘵 𝘪𝘴 𝘶𝘯𝘥𝘰𝘶𝘣𝘵𝘦𝘥𝘭𝘺 𝘵𝘩𝘦 𝘮𝘰𝘴𝘵 𝘴𝘱𝘦𝘤𝘵𝘢𝘤𝘶𝘭𝘢𝘳 𝘧𝘢𝘪𝘭𝘶𝘳𝘦 𝘪𝘯 𝘩𝘶𝘮𝘢𝘯 𝘩𝘪𝘴𝘵𝘰𝘳𝘺. 𝘉𝘶𝘵 𝘪𝘧 𝘤𝘶𝘳𝘦𝘴 𝘰𝘳 𝘦𝘧𝘧𝘦𝘤𝘵𝘪𝘷𝘦 𝘵𝘳𝘦𝘢𝘵𝘮𝘦𝘯𝘵𝘴 𝘩𝘢𝘷𝘦 𝘣𝘦𝘦𝘯 𝘴𝘺𝘴𝘵𝘦𝘮𝘢𝘵𝘪𝘤𝘢𝘭𝘭𝘺 𝘴𝘶𝘱𝘱𝘳𝘦𝘴𝘴𝘦𝘥 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤, 𝘵𝘩𝘦𝘯 𝘵𝘩𝘦𝘪𝘳 𝘢𝘤𝘵𝘪𝘰𝘯𝘴 𝘢𝘳𝘦 𝘤𝘳𝘪𝘮𝘪𝘯𝘢𝘭 𝘪𝘯 𝘯𝘢𝘵𝘶𝘳𝘦 𝘢𝘯𝘥 𝘣𝘭𝘰𝘰𝘥 𝘧𝘳𝘰𝘮 𝘰𝘷𝘦𝘳 530 𝘮𝘪𝘭𝘭𝘪𝘰𝘯 𝘱𝘦𝘰𝘱𝘭𝘦[3] 𝘤𝘰𝘶𝘭𝘥 𝘣𝘦 𝘰𝘯 𝘵𝘩𝘦𝘪𝘳 𝘩𝘢𝘯𝘥𝘴.”
—Mark Sloan
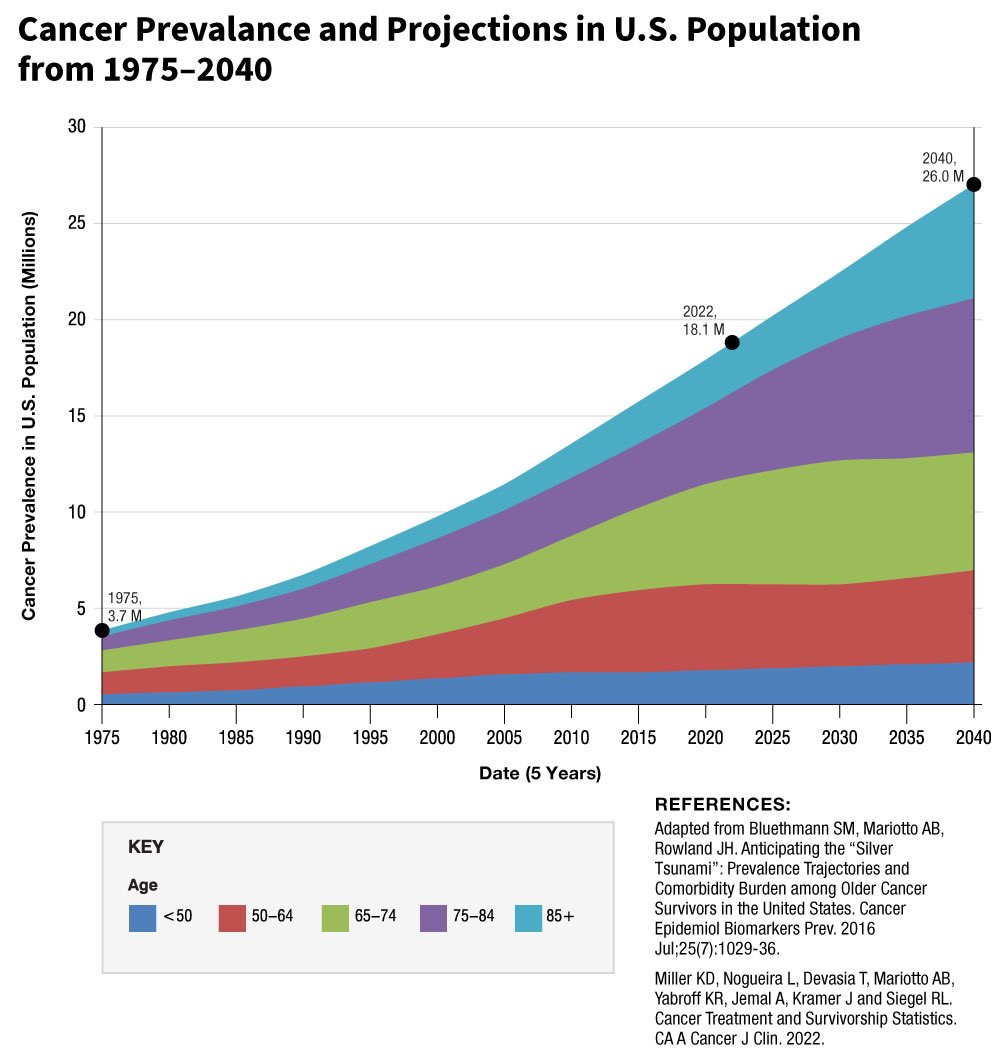
In the year 1900, 1 in 20 people would get cancer.
By 1970, 1 in 10.
By 2000, 1 in 3.
As @Outdoctrination has pointed out, if more people are getting cancer because we live longer, then why are cancer rates going up at every age group?
If we are winning this war, why have youth cancer rates increased 30% since the ‘70s?[4]
𝘐 𝘧𝘪𝘯𝘥 𝘪𝘵 𝘦𝘹𝘵𝘳𝘢𝘰𝘳𝘥𝘪𝘯𝘢𝘳𝘪𝘭𝘺 𝘥𝘪𝘧𝘧𝘪𝘤𝘶𝘭𝘵 𝘵𝘰 𝘣𝘦𝘭𝘪𝘦𝘷𝘦 𝘵𝘩𝘢𝘵 𝘢𝘧𝘵𝘦𝘳 𝘴𝘱𝘦𝘯𝘥𝘪𝘯𝘨 $500 𝘣𝘪𝘭𝘭𝘪𝘰𝘯 𝘥𝘰𝘭𝘭𝘢𝘳𝘴 𝘰𝘯 𝘤𝘢𝘯𝘤𝘦𝘳 𝘳𝘦𝘴𝘦𝘢𝘳𝘤𝘩 𝘴𝘪𝘯𝘤𝘦 1970,[2] 𝘵𝘩𝘦 𝘤𝘢𝘯𝘤𝘦𝘳 𝘦𝘴𝘵𝘢𝘣𝘭𝘪𝘴𝘩𝘮𝘦𝘯𝘵 𝘩𝘢𝘴 𝘤𝘰𝘮𝘦 𝘶𝘱 𝘸𝘪𝘵𝘩 𝘭𝘪𝘵𝘦𝘳𝘢𝘭𝘭𝘺 𝘯𝘰𝘵𝘩𝘪𝘯𝘨 𝘶𝘴𝘦𝘧𝘶𝘭 𝘧𝘰𝘳 𝘱𝘳𝘦𝘷𝘦𝘯𝘵𝘪𝘯𝘨 𝘰𝘳 𝘤𝘶𝘳𝘪𝘯𝘨 𝘵𝘩𝘦 𝘥𝘪𝘴𝘦𝘢𝘴𝘦. 𝘐𝘧 𝘪𝘵’𝘴 𝘵𝘳𝘶𝘦, 𝘵𝘩𝘦𝘯 𝘵𝘩𝘦𝘺 𝘢𝘳𝘦 𝘪𝘯𝘤𝘰𝘮𝘱𝘦𝘵𝘦𝘯𝘵 𝘢𝘯𝘥 𝘵𝘩𝘦𝘪𝘳 𝘢𝘴𝘵𝘰𝘯𝘪𝘴𝘩𝘪𝘯𝘨 𝘭𝘢𝘤𝘬 𝘰𝘧 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘮𝘦𝘯𝘵 𝘪𝘴 𝘶𝘯𝘥𝘰𝘶𝘣𝘵𝘦𝘥𝘭𝘺 𝘵𝘩𝘦 𝘮𝘰𝘴𝘵 𝘴𝘱𝘦𝘤𝘵𝘢𝘤𝘶𝘭𝘢𝘳 𝘧𝘢𝘪𝘭𝘶𝘳𝘦 𝘪𝘯 𝘩𝘶𝘮𝘢𝘯 𝘩𝘪𝘴𝘵𝘰𝘳𝘺. 𝘉𝘶𝘵 𝘪𝘧 𝘤𝘶𝘳𝘦𝘴 𝘰𝘳 𝘦𝘧𝘧𝘦𝘤𝘵𝘪𝘷𝘦 𝘵𝘳𝘦𝘢𝘵𝘮𝘦𝘯𝘵𝘴 𝘩𝘢𝘷𝘦 𝘣𝘦𝘦𝘯 𝘴𝘺𝘴𝘵𝘦𝘮𝘢𝘵𝘪𝘤𝘢𝘭𝘭𝘺 𝘴𝘶𝘱𝘱𝘳𝘦𝘴𝘴𝘦𝘥 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤, 𝘵𝘩𝘦𝘯 𝘵𝘩𝘦𝘪𝘳 𝘢𝘤𝘵𝘪𝘰𝘯𝘴 𝘢𝘳𝘦 𝘤𝘳𝘪𝘮𝘪𝘯𝘢𝘭 𝘪𝘯 𝘯𝘢𝘵𝘶𝘳𝘦 𝘢𝘯𝘥 𝘣𝘭𝘰𝘰𝘥 𝘧𝘳𝘰𝘮 𝘰𝘷𝘦𝘳 530 𝘮𝘪𝘭𝘭𝘪𝘰𝘯 𝘱𝘦𝘰𝘱𝘭𝘦[3] 𝘤𝘰𝘶𝘭𝘥 𝘣𝘦 𝘰𝘯 𝘵𝘩𝘦𝘪𝘳 𝘩𝘢𝘯𝘥𝘴.”
—Mark Sloan
In the year 1900, 1 in 20 people would get cancer.
By 1970, 1 in 10.
By 2000, 1 in 3.
As @Outdoctrination has pointed out, if more people are getting cancer because we live longer, then why are cancer rates going up at every age group?
If we are winning this war, why have youth cancer rates increased 30% since the ‘70s?[4]
𝗠𝗲𝗱𝗶𝗰𝗮𝗹 𝗱𝗼𝗴𝗺𝗮
The earliest form of chemotherapy, Mustargen, was derived from mustard gas during World War II and is still in use to this day.[5] This is unfortunately emblematic of western medicine’s war on the human body.
Essentially, the current allopathic view is that faulty genes cause cancer.
This medical fait accompli is convenient for the pharmaceutical industry, or for the doctor who lacks an explanation for how his patient got sick, but it is simply not true.
✺ 𝗘𝘃𝗶𝗱𝗲𝗻𝗰𝗲 𝘀𝘂𝗴𝗴𝗲𝘀𝘁𝘀 𝘁𝗵𝗮𝘁 𝗴𝗲𝗻𝗲𝘁𝗶𝗰 𝗺𝘂𝘁𝗮𝘁𝗶𝗼𝗻𝘀 𝗼𝗯𝘀𝗲𝗿𝘃𝗲𝗱 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿 𝗮𝗿𝗲 𝗱𝗼𝘄𝗻𝘀𝘁𝗿𝗲𝗮𝗺 𝗳𝗿𝗼𝗺 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝗰 𝗱𝗲𝗿𝗮𝗻𝗴𝗲𝗺𝗲𝗻𝘁𝘀.
There is no single gene, group of genes, nor genome-wide associations to suggest that specific genes determine health outcomes. In fact, it is the state of the mitochondria that determines health outcomes.
“𝘔𝘪𝘵𝘰𝘤𝘩𝘰𝘯𝘥𝘳𝘪𝘢 𝘱𝘳𝘰𝘥𝘶𝘤𝘦 𝘤𝘦𝘭𝘭𝘶𝘭𝘢𝘳 𝘦𝘯𝘦𝘳𝘨𝘺 𝘪𝘯 𝘵𝘩𝘦 𝘩𝘶𝘮𝘢𝘯 𝘣𝘰𝘥𝘺, 𝘢𝘯𝘥 𝘦𝘯𝘦𝘳𝘨𝘺 𝘢𝘷𝘢𝘪𝘭𝘢𝘣𝘪𝘭𝘪𝘵𝘺 𝘪𝘴 𝘵𝘩𝘦 𝘭𝘰𝘸𝘦𝘴𝘵 𝘤𝘰𝘮𝘮𝘰𝘯 𝘥𝘦𝘯𝘰𝘮𝘪𝘯𝘢𝘵𝘰𝘳 𝘯𝘦𝘦𝘥𝘦𝘥 𝘧𝘰𝘳 𝘵𝘩𝘦 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯𝘪𝘯𝘨 𝘰𝘧 𝘢𝘭𝘭 𝘣𝘪𝘰𝘭𝘰𝘨𝘪𝘤𝘢𝘭 𝘴𝘺𝘴𝘵𝘦𝘮𝘴.”
—David C. Geary, PhD
Healthy mitochondria transplanted into breast cancer cells were shown to reverse cancer, while cells paired with unhealthy mitochondria induced cancer.[6] Clearly, there’s more to the story than genes.
Genetic risk accounts for a very small percentage of disease risk onset,[7] and it turns out that disease expression within a family is highly variable.[8]
“𝘛𝘩𝘦 𝘥𝘪𝘴𝘤𝘰𝘳𝘥𝘢𝘯𝘤𝘦 𝘣𝘦𝘵𝘸𝘦𝘦𝘯 𝘨𝘦𝘯𝘰𝘵𝘺𝘱𝘦 𝘢𝘯𝘥 𝘱𝘩𝘦𝘯𝘰𝘵𝘺𝘱𝘦 𝘪𝘴 𝘱𝘢𝘳𝘵𝘪𝘤𝘶𝘭𝘢𝘳𝘭𝘺 𝘣𝘳𝘰𝘢𝘥 𝘸𝘪𝘵𝘩 𝘮𝘪𝘵𝘰𝘤𝘩𝘰𝘯𝘥𝘳𝘪𝘢𝘭 𝘥𝘪𝘴𝘦𝘢𝘴𝘦𝘴,[9] 𝘢𝘯𝘥 𝘸𝘩𝘦𝘯 𝘸𝘦 𝘢𝘥𝘥 𝘵𝘩𝘦 𝘱𝘰𝘴𝘴𝘪𝘣𝘪𝘭𝘪𝘵𝘺 𝘰𝘧 𝘥𝘦 𝘯𝘰𝘷𝘰 𝘮𝘶𝘵𝘢𝘵𝘪𝘰𝘯𝘴,[10] 𝘵𝘩𝘦 𝘴𝘤𝘩𝘪𝘴𝘮 𝘨𝘳𝘰𝘸𝘴 𝘪𝘮𝘮𝘦𝘯𝘴𝘦𝘭𝘺,” writes Derrick Lonsdale, MD, FACN, CNS.
The earliest form of chemotherapy, Mustargen, was derived from mustard gas during World War II and is still in use to this day.[5] This is unfortunately emblematic of western medicine’s war on the human body.
Essentially, the current allopathic view is that faulty genes cause cancer.
This medical fait accompli is convenient for the pharmaceutical industry, or for the doctor who lacks an explanation for how his patient got sick, but it is simply not true.
✺ 𝗘𝘃𝗶𝗱𝗲𝗻𝗰𝗲 𝘀𝘂𝗴𝗴𝗲𝘀𝘁𝘀 𝘁𝗵𝗮𝘁 𝗴𝗲𝗻𝗲𝘁𝗶𝗰 𝗺𝘂𝘁𝗮𝘁𝗶𝗼𝗻𝘀 𝗼𝗯𝘀𝗲𝗿𝘃𝗲𝗱 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿 𝗮𝗿𝗲 𝗱𝗼𝘄𝗻𝘀𝘁𝗿𝗲𝗮𝗺 𝗳𝗿𝗼𝗺 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝗰 𝗱𝗲𝗿𝗮𝗻𝗴𝗲𝗺𝗲𝗻𝘁𝘀.
There is no single gene, group of genes, nor genome-wide associations to suggest that specific genes determine health outcomes. In fact, it is the state of the mitochondria that determines health outcomes.
“𝘔𝘪𝘵𝘰𝘤𝘩𝘰𝘯𝘥𝘳𝘪𝘢 𝘱𝘳𝘰𝘥𝘶𝘤𝘦 𝘤𝘦𝘭𝘭𝘶𝘭𝘢𝘳 𝘦𝘯𝘦𝘳𝘨𝘺 𝘪𝘯 𝘵𝘩𝘦 𝘩𝘶𝘮𝘢𝘯 𝘣𝘰𝘥𝘺, 𝘢𝘯𝘥 𝘦𝘯𝘦𝘳𝘨𝘺 𝘢𝘷𝘢𝘪𝘭𝘢𝘣𝘪𝘭𝘪𝘵𝘺 𝘪𝘴 𝘵𝘩𝘦 𝘭𝘰𝘸𝘦𝘴𝘵 𝘤𝘰𝘮𝘮𝘰𝘯 𝘥𝘦𝘯𝘰𝘮𝘪𝘯𝘢𝘵𝘰𝘳 𝘯𝘦𝘦𝘥𝘦𝘥 𝘧𝘰𝘳 𝘵𝘩𝘦 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯𝘪𝘯𝘨 𝘰𝘧 𝘢𝘭𝘭 𝘣𝘪𝘰𝘭𝘰𝘨𝘪𝘤𝘢𝘭 𝘴𝘺𝘴𝘵𝘦𝘮𝘴.”
—David C. Geary, PhD
Healthy mitochondria transplanted into breast cancer cells were shown to reverse cancer, while cells paired with unhealthy mitochondria induced cancer.[6] Clearly, there’s more to the story than genes.
Genetic risk accounts for a very small percentage of disease risk onset,[7] and it turns out that disease expression within a family is highly variable.[8]
“𝘛𝘩𝘦 𝘥𝘪𝘴𝘤𝘰𝘳𝘥𝘢𝘯𝘤𝘦 𝘣𝘦𝘵𝘸𝘦𝘦𝘯 𝘨𝘦𝘯𝘰𝘵𝘺𝘱𝘦 𝘢𝘯𝘥 𝘱𝘩𝘦𝘯𝘰𝘵𝘺𝘱𝘦 𝘪𝘴 𝘱𝘢𝘳𝘵𝘪𝘤𝘶𝘭𝘢𝘳𝘭𝘺 𝘣𝘳𝘰𝘢𝘥 𝘸𝘪𝘵𝘩 𝘮𝘪𝘵𝘰𝘤𝘩𝘰𝘯𝘥𝘳𝘪𝘢𝘭 𝘥𝘪𝘴𝘦𝘢𝘴𝘦𝘴,[9] 𝘢𝘯𝘥 𝘸𝘩𝘦𝘯 𝘸𝘦 𝘢𝘥𝘥 𝘵𝘩𝘦 𝘱𝘰𝘴𝘴𝘪𝘣𝘪𝘭𝘪𝘵𝘺 𝘰𝘧 𝘥𝘦 𝘯𝘰𝘷𝘰 𝘮𝘶𝘵𝘢𝘵𝘪𝘰𝘯𝘴,[10] 𝘵𝘩𝘦 𝘴𝘤𝘩𝘪𝘴𝘮 𝘨𝘳𝘰𝘸𝘴 𝘪𝘮𝘮𝘦𝘯𝘴𝘦𝘭𝘺,” writes Derrick Lonsdale, MD, FACN, CNS.
𝗖𝗮𝗻𝗰𝗲𝗿 𝘁𝗿𝗲𝗮𝘁𝗺𝗲𝗻𝘁𝘀: 𝗶𝗮𝘁𝗿𝗼𝗴𝗲𝗻𝗲𝘀𝗶𝘀
“𝘊𝘢𝘳𝘤𝘪𝘯𝘰𝘨𝘦𝘯𝘦𝘴𝘪𝘴 𝘢𝘯𝘥 𝘤𝘢𝘯𝘤𝘦𝘳 𝘵𝘩𝘦𝘳𝘢𝘱𝘺 𝘢𝘳𝘦 𝘵𝘸𝘰 𝘴𝘪𝘥𝘦𝘴 𝘰𝘧 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘤𝘰𝘪𝘯, 𝘴𝘶𝘤𝘩 𝘵𝘩𝘢𝘵 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘤𝘺𝘵𝘰𝘵𝘰𝘹𝘪𝘤 𝘢𝘨𝘦𝘯𝘵 𝘤𝘢𝘯 𝘤𝘢𝘶𝘴𝘦 𝘤𝘢𝘯𝘤𝘦𝘳 𝘢𝘯𝘥 𝘣𝘦 𝘶𝘴𝘦𝘥 𝘵𝘰 𝘵𝘳𝘦𝘢𝘵 𝘤𝘢𝘯𝘤𝘦𝘳.”
—Mikhail V. Blagosklonny, MD, PhD
In western medicine, we believe that for every one disease, there is one cure. One pharmaceutical, one enzyme that needs inhibition, one organ that needs removal, one biomarker that needs to be hammered back into a “normal” range, etc.
This is a very mechanical view of the body, and it fails to consider how many pleiotropic effects we see from simple vitamins and bioidentical hormones.
The pharmaceutical industry’s total disinterest in vitamins, minerals, diet, lifestyle, and youth-associated hormones is unsurprising since there is no money in these unpatentable treatments.
But this disinterest has serious consequences for those who still put their faith in doctors. Rather than guiding patients to health, doctors may be leading them into risky treatments that worsen their condition.
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗺𝗲𝘁𝗮𝘀𝘁𝗮𝘀𝗶𝘀 𝗶𝘀 𝘁𝗵𝗲 𝗽𝗿𝗶𝗺𝗮𝗿𝘆 𝗰𝗮𝘂𝘀𝗲 𝗼𝗳 𝗺𝗼𝘀𝘁 𝗰𝗮𝗻𝗰𝗲𝗿 𝗱𝗲𝗮𝘁𝗵𝘀.
Despite this, many people are unaware that surgically removing a tumor has been known to cause cancer metastasis for over a century.[11][12][13]
In fact, the stress of surgery alone can drastically increase the cancer metabolism while decreasing thyroid activity, perpetuating the exact conditions that brought about the tumor microenvironment in the first place. This applies to biopsies as well.[14]
“𝘊𝘢𝘳𝘤𝘪𝘯𝘰𝘨𝘦𝘯𝘦𝘴𝘪𝘴 𝘢𝘯𝘥 𝘤𝘢𝘯𝘤𝘦𝘳 𝘵𝘩𝘦𝘳𝘢𝘱𝘺 𝘢𝘳𝘦 𝘵𝘸𝘰 𝘴𝘪𝘥𝘦𝘴 𝘰𝘧 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘤𝘰𝘪𝘯, 𝘴𝘶𝘤𝘩 𝘵𝘩𝘢𝘵 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘤𝘺𝘵𝘰𝘵𝘰𝘹𝘪𝘤 𝘢𝘨𝘦𝘯𝘵 𝘤𝘢𝘯 𝘤𝘢𝘶𝘴𝘦 𝘤𝘢𝘯𝘤𝘦𝘳 𝘢𝘯𝘥 𝘣𝘦 𝘶𝘴𝘦𝘥 𝘵𝘰 𝘵𝘳𝘦𝘢𝘵 𝘤𝘢𝘯𝘤𝘦𝘳.”
—Mikhail V. Blagosklonny, MD, PhD
In western medicine, we believe that for every one disease, there is one cure. One pharmaceutical, one enzyme that needs inhibition, one organ that needs removal, one biomarker that needs to be hammered back into a “normal” range, etc.
This is a very mechanical view of the body, and it fails to consider how many pleiotropic effects we see from simple vitamins and bioidentical hormones.
The pharmaceutical industry’s total disinterest in vitamins, minerals, diet, lifestyle, and youth-associated hormones is unsurprising since there is no money in these unpatentable treatments.
But this disinterest has serious consequences for those who still put their faith in doctors. Rather than guiding patients to health, doctors may be leading them into risky treatments that worsen their condition.
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗺𝗲𝘁𝗮𝘀𝘁𝗮𝘀𝗶𝘀 𝗶𝘀 𝘁𝗵𝗲 𝗽𝗿𝗶𝗺𝗮𝗿𝘆 𝗰𝗮𝘂𝘀𝗲 𝗼𝗳 𝗺𝗼𝘀𝘁 𝗰𝗮𝗻𝗰𝗲𝗿 𝗱𝗲𝗮𝘁𝗵𝘀.
Despite this, many people are unaware that surgically removing a tumor has been known to cause cancer metastasis for over a century.[11][12][13]
In fact, the stress of surgery alone can drastically increase the cancer metabolism while decreasing thyroid activity, perpetuating the exact conditions that brought about the tumor microenvironment in the first place. This applies to biopsies as well.[14]

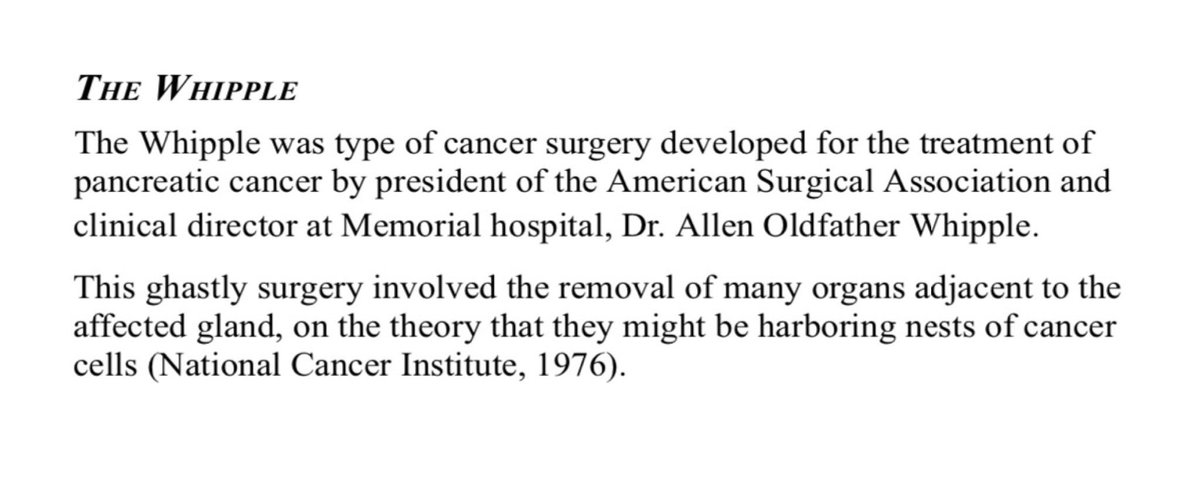
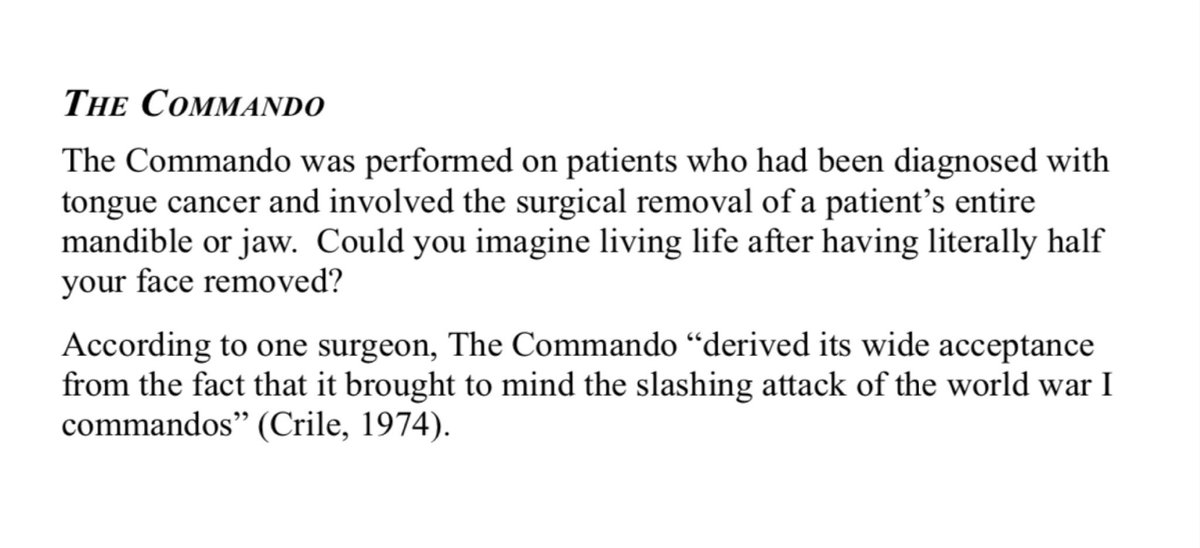
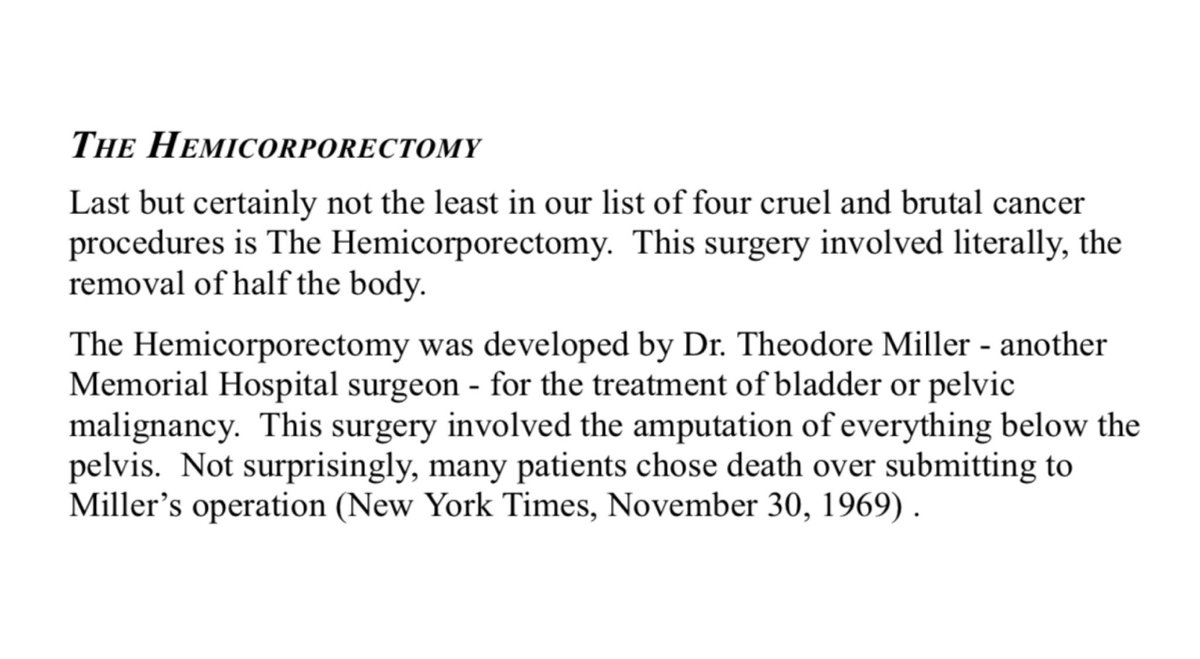
𝗙𝗼𝘂𝗿 𝗷𝗮𝘄-𝗱𝗿𝗼𝗽𝗽𝗶𝗻𝗴 𝗰𝗮𝗻𝗰𝗲𝗿 𝘀𝘂𝗿𝗴𝗲𝗿𝗶𝗲𝘀 𝘀𝘁𝗶𝗹𝗹 𝗶𝗻 𝘂𝘀𝗲 𝘁𝗼𝗱𝗮𝘆[15]

𝗧𝗵𝗲 𝗯𝗶𝗼𝗲𝗻𝗲𝗿𝗴𝗲𝘁𝗶𝗰 𝘃𝗶𝗲𝘄 𝗼𝗳 𝗰𝗮𝗻𝗰𝗲𝗿
“𝘌𝘷𝘦𝘳𝘺 𝘴𝘵𝘳𝘦𝘴𝘴 𝘭𝘦𝘢𝘷𝘦𝘴 𝘢𝘯 𝘪𝘯𝘥𝘦𝘭𝘪𝘣𝘭𝘦 𝘴𝘤𝘢𝘳, 𝘢𝘯𝘥 𝘵𝘩𝘦 𝘰𝘳𝘨𝘢𝘯𝘪𝘴𝘮 𝘱𝘢𝘺𝘴 𝘧𝘰𝘳 𝘪𝘵𝘴 𝘴𝘶𝘳𝘷𝘪𝘷𝘢𝘭 𝘢𝘧𝘵𝘦𝘳 𝘢 𝘴𝘵𝘳𝘦𝘴𝘴𝘧𝘶𝘭 𝘴𝘪𝘵𝘶𝘢𝘵𝘪𝘰𝘯 𝘣𝘺 𝘣𝘦𝘤𝘰𝘮𝘪𝘯𝘨 𝘢 𝘭𝘪𝘵𝘵𝘭𝘦 𝘰𝘭𝘥𝘦𝘳.”
—Hans Selye, endocrinologist and creator of the stress theory
Cancer is a metabolic derangement, a state characterized by the organism’s chronically reduced capacity to meet the environment’s energetic demands, and a big part of that is the inability to use oxygen.
“𝘓𝘪𝘧𝘦 𝘴𝘶𝘱𝘱𝘰𝘳𝘵𝘴 𝘭𝘪𝘧𝘦, 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯 𝘣𝘶𝘪𝘭𝘥𝘴 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦, 𝘢𝘯𝘥 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦 𝘱𝘳𝘰𝘥𝘶𝘤𝘦𝘴 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯. 𝘖𝘯𝘤𝘦 𝘵𝘩𝘦 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯 𝘤𝘦𝘢𝘴𝘦𝘴, 𝘵𝘩𝘦 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦 𝘤𝘰𝘭𝘭𝘢𝘱𝘴𝘦𝘴. 𝘐𝘵 𝘮𝘢𝘪𝘯𝘵𝘢𝘪𝘯𝘴 𝘪𝘵𝘴𝘦𝘭𝘧 𝘣𝘺 𝘸𝘰𝘳𝘬𝘪𝘯𝘨. 𝘈 𝘨𝘰𝘰𝘥 𝘸𝘰𝘳𝘬𝘪𝘯𝘨 𝘰𝘳𝘥𝘦𝘳 𝘪𝘴 𝘵𝘩𝘶𝘴 𝘵𝘩𝘦 𝘮𝘰𝘴𝘵 𝘴𝘵𝘢𝘣𝘭𝘦 𝘴𝘵𝘢𝘵𝘦.”
—Albert Szent-Györgyi, biochemist and Nobel laureate
Energy metabolism was not considered an important factor in the disease process until we began to understand mitochondrial activity.[16][17][18]
𝗔 𝗳𝗲𝘄 𝘄𝗮𝘆𝘀 𝘁𝗼 𝗱𝗲𝘀𝗰𝗿𝗶𝗯𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗳𝗿𝗼𝗺 𝗮 𝗯𝗶𝗼𝗲𝗻𝗲𝗿𝗴𝗲𝘁𝗶𝗰 𝗽𝗲𝗿𝘀𝗽𝗲𝗰𝘁𝗶𝘃𝗲:
✺ “Cancer metabolism”
✺ “Stress metabolism”
✺ “Glycolytic metabolism”
✺ “Pre-oxidative metabolism”
✺ “Lactic acid fermentation”
✺ “Wound overhealing”
These are all the same thing: a cellular reversion to an ancient process of inefficiently producing energy (ATP) by failing to use oxygen.
𝗧𝗵𝗲 𝗵𝘂𝗺𝗮𝗻 𝗯𝗼𝗱𝘆 𝗶𝘀 𝗰𝗼𝗺𝗽𝗿𝗶𝘀𝗲𝗱 𝗼𝗳 𝗮𝗻 𝗲𝘀𝘁𝗶𝗺𝗮𝘁𝗲𝗱 𝟯𝟳 𝘁𝗿𝗶𝗹𝗹𝗶𝗼𝗻 𝗰𝗲𝗹𝗹𝘀, 𝗮𝗻𝗱 𝘁𝗵𝗲𝘆 𝗮𝗹𝗹 𝗿𝗲𝗾𝘂𝗶𝗿𝗲 𝗲𝗻𝗲𝗿𝗴𝘆. 𝗔 𝗹𝗼𝘁 𝗰𝗮𝗻 𝗴𝗼 𝘄𝗿𝗼𝗻𝗴 𝗶𝗻 𝗮 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗲𝗻𝗲𝗿𝗴𝘆 𝗱𝗲𝗳𝗶𝗰𝗶𝘁.
Fuel + Oxygen + Catalyst = [𝘌𝘯𝘦𝘳𝘨𝘺 = 𝗦𝘁𝗿𝘂𝗰𝘁𝘂𝗿𝗲]
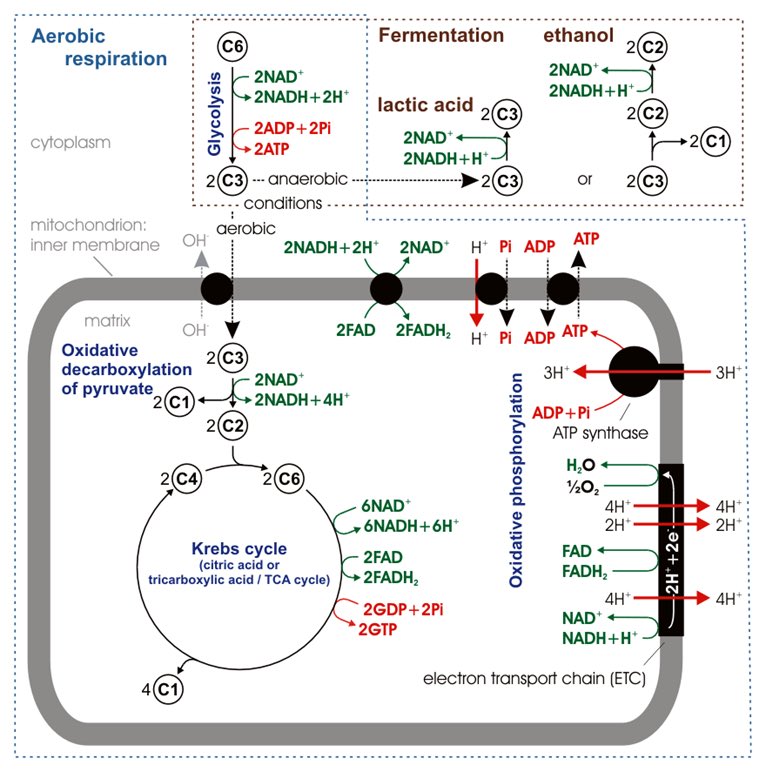
𝗚𝗹𝘂𝗰𝗼𝘀𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺:
1. Glycolysis
2. Pyruvate oxidation✶
3. Krebs cycle✶
4. Electron transport chain
✶These steps are thiamine-dependent.
✺ 𝗚𝗹𝘆𝗰𝗼𝗹𝘆𝘀𝗶𝘀 𝗶𝘀 𝗮𝗻 𝗮𝗻𝗮𝗲𝗿𝗼𝗯𝗶𝗰 𝗽𝗿𝗼𝗰𝗲𝘀𝘀, 𝗺𝗲𝗮𝗻𝗶𝗻𝗴 𝗶𝘁 𝗱𝗼𝗲𝘀𝗻’𝘁 𝘂𝘀𝗲 𝗼𝘅𝘆𝗴𝗲𝗻—𝗳𝗼𝗿 𝗲𝘃𝗲𝗿𝘆𝘁𝗵𝗶𝗻𝗴 𝗮𝗳𝘁𝗲𝗿 𝗴𝗹𝘆𝗰𝗼𝗹𝘆𝘀𝗶𝘀, 𝗼𝘅𝘆𝗴𝗲𝗻 𝗶𝘀 𝗰𝗿𝘂𝗰𝗶𝗮𝗹.
“𝘌𝘷𝘦𝘳𝘺 𝘴𝘵𝘳𝘦𝘴𝘴 𝘭𝘦𝘢𝘷𝘦𝘴 𝘢𝘯 𝘪𝘯𝘥𝘦𝘭𝘪𝘣𝘭𝘦 𝘴𝘤𝘢𝘳, 𝘢𝘯𝘥 𝘵𝘩𝘦 𝘰𝘳𝘨𝘢𝘯𝘪𝘴𝘮 𝘱𝘢𝘺𝘴 𝘧𝘰𝘳 𝘪𝘵𝘴 𝘴𝘶𝘳𝘷𝘪𝘷𝘢𝘭 𝘢𝘧𝘵𝘦𝘳 𝘢 𝘴𝘵𝘳𝘦𝘴𝘴𝘧𝘶𝘭 𝘴𝘪𝘵𝘶𝘢𝘵𝘪𝘰𝘯 𝘣𝘺 𝘣𝘦𝘤𝘰𝘮𝘪𝘯𝘨 𝘢 𝘭𝘪𝘵𝘵𝘭𝘦 𝘰𝘭𝘥𝘦𝘳.”
—Hans Selye, endocrinologist and creator of the stress theory
Cancer is a metabolic derangement, a state characterized by the organism’s chronically reduced capacity to meet the environment’s energetic demands, and a big part of that is the inability to use oxygen.
“𝘓𝘪𝘧𝘦 𝘴𝘶𝘱𝘱𝘰𝘳𝘵𝘴 𝘭𝘪𝘧𝘦, 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯 𝘣𝘶𝘪𝘭𝘥𝘴 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦, 𝘢𝘯𝘥 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦 𝘱𝘳𝘰𝘥𝘶𝘤𝘦𝘴 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯. 𝘖𝘯𝘤𝘦 𝘵𝘩𝘦 𝘧𝘶𝘯𝘤𝘵𝘪𝘰𝘯 𝘤𝘦𝘢𝘴𝘦𝘴, 𝘵𝘩𝘦 𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦 𝘤𝘰𝘭𝘭𝘢𝘱𝘴𝘦𝘴. 𝘐𝘵 𝘮𝘢𝘪𝘯𝘵𝘢𝘪𝘯𝘴 𝘪𝘵𝘴𝘦𝘭𝘧 𝘣𝘺 𝘸𝘰𝘳𝘬𝘪𝘯𝘨. 𝘈 𝘨𝘰𝘰𝘥 𝘸𝘰𝘳𝘬𝘪𝘯𝘨 𝘰𝘳𝘥𝘦𝘳 𝘪𝘴 𝘵𝘩𝘶𝘴 𝘵𝘩𝘦 𝘮𝘰𝘴𝘵 𝘴𝘵𝘢𝘣𝘭𝘦 𝘴𝘵𝘢𝘵𝘦.”
—Albert Szent-Györgyi, biochemist and Nobel laureate
Energy metabolism was not considered an important factor in the disease process until we began to understand mitochondrial activity.[16][17][18]
𝗔 𝗳𝗲𝘄 𝘄𝗮𝘆𝘀 𝘁𝗼 𝗱𝗲𝘀𝗰𝗿𝗶𝗯𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗳𝗿𝗼𝗺 𝗮 𝗯𝗶𝗼𝗲𝗻𝗲𝗿𝗴𝗲𝘁𝗶𝗰 𝗽𝗲𝗿𝘀𝗽𝗲𝗰𝘁𝗶𝘃𝗲:
✺ “Cancer metabolism”
✺ “Stress metabolism”
✺ “Glycolytic metabolism”
✺ “Pre-oxidative metabolism”
✺ “Lactic acid fermentation”
✺ “Wound overhealing”
These are all the same thing: a cellular reversion to an ancient process of inefficiently producing energy (ATP) by failing to use oxygen.
𝗧𝗵𝗲 𝗵𝘂𝗺𝗮𝗻 𝗯𝗼𝗱𝘆 𝗶𝘀 𝗰𝗼𝗺𝗽𝗿𝗶𝘀𝗲𝗱 𝗼𝗳 𝗮𝗻 𝗲𝘀𝘁𝗶𝗺𝗮𝘁𝗲𝗱 𝟯𝟳 𝘁𝗿𝗶𝗹𝗹𝗶𝗼𝗻 𝗰𝗲𝗹𝗹𝘀, 𝗮𝗻𝗱 𝘁𝗵𝗲𝘆 𝗮𝗹𝗹 𝗿𝗲𝗾𝘂𝗶𝗿𝗲 𝗲𝗻𝗲𝗿𝗴𝘆. 𝗔 𝗹𝗼𝘁 𝗰𝗮𝗻 𝗴𝗼 𝘄𝗿𝗼𝗻𝗴 𝗶𝗻 𝗮 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗲𝗻𝗲𝗿𝗴𝘆 𝗱𝗲𝗳𝗶𝗰𝗶𝘁.
Fuel + Oxygen + Catalyst = [𝘌𝘯𝘦𝘳𝘨𝘺 = 𝗦𝘁𝗿𝘂𝗰𝘁𝘂𝗿𝗲]
𝗚𝗹𝘂𝗰𝗼𝘀𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺:
1. Glycolysis
2. Pyruvate oxidation✶
3. Krebs cycle✶
4. Electron transport chain
✶These steps are thiamine-dependent.
✺ 𝗚𝗹𝘆𝗰𝗼𝗹𝘆𝘀𝗶𝘀 𝗶𝘀 𝗮𝗻 𝗮𝗻𝗮𝗲𝗿𝗼𝗯𝗶𝗰 𝗽𝗿𝗼𝗰𝗲𝘀𝘀, 𝗺𝗲𝗮𝗻𝗶𝗻𝗴 𝗶𝘁 𝗱𝗼𝗲𝘀𝗻’𝘁 𝘂𝘀𝗲 𝗼𝘅𝘆𝗴𝗲𝗻—𝗳𝗼𝗿 𝗲𝘃𝗲𝗿𝘆𝘁𝗵𝗶𝗻𝗴 𝗮𝗳𝘁𝗲𝗿 𝗴𝗹𝘆𝗰𝗼𝗹𝘆𝘀𝗶𝘀, 𝗼𝘅𝘆𝗴𝗲𝗻 𝗶𝘀 𝗰𝗿𝘂𝗰𝗶𝗮𝗹.
𝗪𝗵𝗮𝘁 𝘄𝗲 𝘀𝗲𝗲 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿:
- A cell’s inability to oxidize glucose.
- A resulting excess of lactate.[19]
- Impaired glucose metabolism means reduced ability to regenerate glutathione, leading to oxidative stress.[20]
- Low mitochondrial NAD/NADH ratio.[21][22]
- Up-regulation of pyruvate dehydrogenase kinase (PDK) which inhibits pyruvate dehydrogenase (PDH) thus blocking entry into the TCA cycle.[23]
- Lack of succinate dehydrogenase (SDH) which allows succinate to build up, activating hypoxia-inducible factor (HIF-1α).[24]
- Dependence on glycolysis for ATP generation.[25]
- Excess of nitric oxide, rising adaptively in a low CO2 state and triggering the adhesion of circulating tumor cells onto body tissues.[26]
- Evasion of apoptosis (programmed cell death).[27]
This promotes tissue hypoxia and a state of chronic, low-grade acidosis. The cancer cell is alkaline inside and acidic outside, rather than entirely acidic, as was previously thought.[28]
✺ 𝗔𝗹𝗹 𝘁𝗵𝗮𝘁 𝗶𝘀 𝗻𝗲𝗲𝗱𝗲𝗱 𝘁𝗼 𝗰𝗮𝘂𝘀𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝘀 𝘀𝘂𝗳𝗳𝗶𝗰𝗶𝗲𝗻𝘁 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝗰 𝘀𝘁𝗿𝗲𝘀𝘀 𝘀𝘂𝘀𝘁𝗮𝗶𝗻𝗲𝗱 𝗶𝗻 𝗮 𝗵𝘆𝗽𝗼𝘁𝗵𝘆𝗿𝗼𝗶𝗱 𝘀𝘁𝗮𝘁𝗲.
✺ 𝗔𝗹𝗹 𝘁𝗵𝗮𝘁 𝗶𝘀 𝗻𝗲𝗲𝗱𝗲𝗱 𝘁𝗼 𝗽𝗿𝗲𝘃𝗲𝗻𝘁 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝘀 𝗺𝗼𝗺𝗲𝗻𝘁𝘂𝗺 𝗶𝗻 𝘁𝗵𝗲 𝗼𝗽𝗽𝗼𝘀𝗶𝘁𝗲 𝗱𝗶𝗿𝗲𝗰𝘁𝗶𝗼𝗻, 𝘀𝘂𝘀𝘁𝗮𝗶𝗻𝗲𝗱 𝗶𝗻 𝗮 𝗲𝘂𝘁𝗵𝘆𝗿𝗼𝗶𝗱 𝘀𝘁𝗮𝘁𝗲.
𝗦𝗼𝗺𝗲 𝗸𝗲𝘆 𝘁𝗮𝗸𝗲𝗮𝘄𝗮𝘆𝘀:
- Pyruvate dehydrogenase (PDH) is the key to enter the Krebs cycle.
- PDH is thiamine and magnesium-dependent.
- Stimulating PDH triggers apoptosis in cancer cells.[29]
- Thiamine fights hypoxia.[30]
- Thiamine is a carbonic anhydrase inhibitor, meaning it improves the CO2/lactate ratio, oxygenating the tissue via the Bohr effect.
- High dose thiamine produces a growth-inhibitory effect in cancer.[31]
- Thiamine lowers serum lactate.[32][33][34][35]
- Metabolic health, i.e. high-functioning mitochondria, dictates health outcomes.[36]
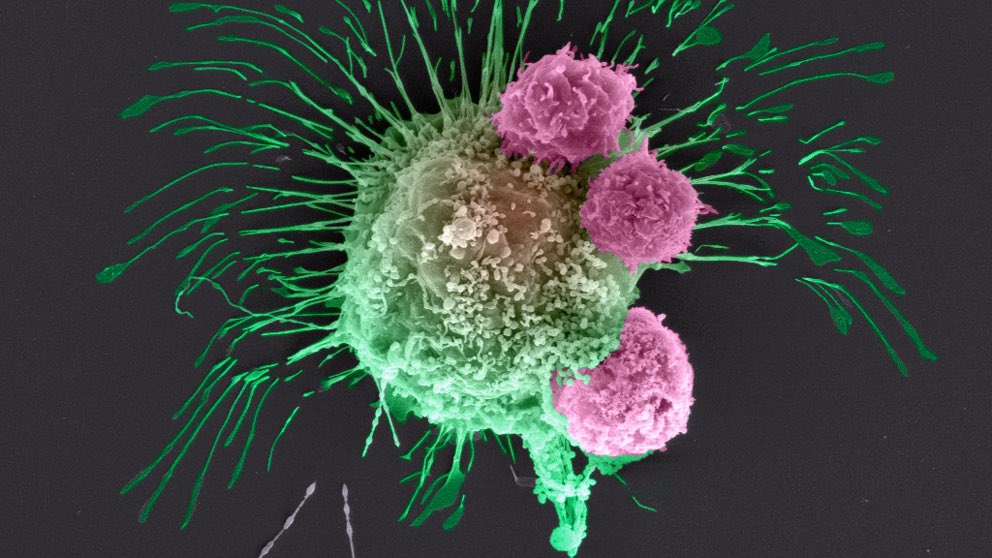
“𝘊𝘢𝘯𝘤𝘦𝘳, 𝘵𝘩𝘦 𝘥𝘪𝘴𝘦𝘢𝘴𝘦, 𝘪𝘴 𝘮𝘶𝘤𝘩 𝘮𝘰𝘳𝘦 𝘵𝘩𝘢𝘯 𝘢 𝘤𝘦𝘭𝘭𝘶𝘭𝘢𝘳 𝘥𝘦𝘧𝘦𝘤𝘵. 𝘔𝘰𝘴𝘵 𝘰𝘧 𝘵𝘩𝘦 𝘤𝘦𝘭𝘭𝘴 𝘪𝘯 𝘢 𝘵𝘶𝘮𝘰𝘳 𝘢𝘳𝘦 𝘴𝘰 𝘥𝘦𝘧𝘦𝘤𝘵𝘪𝘷𝘦 𝘵𝘩𝘢𝘵 𝘵𝘩𝘦𝘺 𝘢𝘳𝘦 𝘪𝘯 𝘵𝘩𝘦 𝘱𝘳𝘰𝘤𝘦𝘴𝘴 𝘰𝘧 𝘥𝘺𝘪𝘯𝘨, 𝘢𝘯𝘥 𝘪𝘯 𝘵𝘩𝘢𝘵 𝘱𝘳𝘰𝘤𝘦𝘴𝘴 𝘵𝘩𝘦𝘺 𝘳𝘦𝘤𝘳𝘶𝘪𝘵 𝘳𝘦𝘱𝘭𝘢𝘤𝘦𝘮𝘦𝘯𝘵 𝘤𝘦𝘭𝘭𝘴, 𝘸𝘩𝘪𝘤𝘩 𝘦𝘹𝘱𝘦𝘳𝘪𝘦𝘯𝘤𝘦 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘥𝘢𝘮𝘢𝘨𝘪𝘯𝘨 𝘤𝘰𝘯𝘥𝘪𝘵𝘪𝘰𝘯𝘴. 𝙏𝙝𝙚 𝙡𝙤𝙘𝙖𝙡 𝙖𝙣𝙙 𝙧𝙚𝙜𝙞𝙤𝙣𝙖𝙡 𝙚𝙭𝙩𝙧𝙖𝙘𝙚𝙡𝙡𝙪𝙡𝙖𝙧 𝙘𝙤𝙣𝙙𝙞𝙩𝙞𝙤𝙣𝙨, 𝙖𝙣𝙙 𝙩𝙝𝙚 𝙘𝙤𝙣𝙙𝙞𝙩𝙞𝙤𝙣 𝙤𝙛 𝙩𝙝𝙚 𝙝𝙤𝙨𝙩, 𝙖𝙧𝙚 𝙟𝙪𝙨𝙩 𝙖𝙨 𝙘𝙚𝙣𝙩𝙧𝙖𝙡 𝙩𝙤 𝙩𝙝𝙚 𝙙𝙞𝙨𝙚𝙖𝙨𝙚 𝙖𝙨 𝙩𝙝𝙚 𝙛𝙖𝙞𝙡𝙞𝙣𝙜 𝙢𝙞𝙩𝙤𝙘𝙝𝙤𝙣𝙙𝙧𝙞𝙖.”
—Ray Peat, PhD
- A cell’s inability to oxidize glucose.
- A resulting excess of lactate.[19]
- Impaired glucose metabolism means reduced ability to regenerate glutathione, leading to oxidative stress.[20]
- Low mitochondrial NAD/NADH ratio.[21][22]
- Up-regulation of pyruvate dehydrogenase kinase (PDK) which inhibits pyruvate dehydrogenase (PDH) thus blocking entry into the TCA cycle.[23]
- Lack of succinate dehydrogenase (SDH) which allows succinate to build up, activating hypoxia-inducible factor (HIF-1α).[24]
- Dependence on glycolysis for ATP generation.[25]
- Excess of nitric oxide, rising adaptively in a low CO2 state and triggering the adhesion of circulating tumor cells onto body tissues.[26]
- Evasion of apoptosis (programmed cell death).[27]
This promotes tissue hypoxia and a state of chronic, low-grade acidosis. The cancer cell is alkaline inside and acidic outside, rather than entirely acidic, as was previously thought.[28]
✺ 𝗔𝗹𝗹 𝘁𝗵𝗮𝘁 𝗶𝘀 𝗻𝗲𝗲𝗱𝗲𝗱 𝘁𝗼 𝗰𝗮𝘂𝘀𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝘀 𝘀𝘂𝗳𝗳𝗶𝗰𝗶𝗲𝗻𝘁 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝗰 𝘀𝘁𝗿𝗲𝘀𝘀 𝘀𝘂𝘀𝘁𝗮𝗶𝗻𝗲𝗱 𝗶𝗻 𝗮 𝗵𝘆𝗽𝗼𝘁𝗵𝘆𝗿𝗼𝗶𝗱 𝘀𝘁𝗮𝘁𝗲.
✺ 𝗔𝗹𝗹 𝘁𝗵𝗮𝘁 𝗶𝘀 𝗻𝗲𝗲𝗱𝗲𝗱 𝘁𝗼 𝗽𝗿𝗲𝘃𝗲𝗻𝘁 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝘀 𝗺𝗼𝗺𝗲𝗻𝘁𝘂𝗺 𝗶𝗻 𝘁𝗵𝗲 𝗼𝗽𝗽𝗼𝘀𝗶𝘁𝗲 𝗱𝗶𝗿𝗲𝗰𝘁𝗶𝗼𝗻, 𝘀𝘂𝘀𝘁𝗮𝗶𝗻𝗲𝗱 𝗶𝗻 𝗮 𝗲𝘂𝘁𝗵𝘆𝗿𝗼𝗶𝗱 𝘀𝘁𝗮𝘁𝗲.
𝗦𝗼𝗺𝗲 𝗸𝗲𝘆 𝘁𝗮𝗸𝗲𝗮𝘄𝗮𝘆𝘀:
- Pyruvate dehydrogenase (PDH) is the key to enter the Krebs cycle.
- PDH is thiamine and magnesium-dependent.
- Stimulating PDH triggers apoptosis in cancer cells.[29]
- Thiamine fights hypoxia.[30]
- Thiamine is a carbonic anhydrase inhibitor, meaning it improves the CO2/lactate ratio, oxygenating the tissue via the Bohr effect.
- High dose thiamine produces a growth-inhibitory effect in cancer.[31]
- Thiamine lowers serum lactate.[32][33][34][35]
- Metabolic health, i.e. high-functioning mitochondria, dictates health outcomes.[36]
“𝘊𝘢𝘯𝘤𝘦𝘳, 𝘵𝘩𝘦 𝘥𝘪𝘴𝘦𝘢𝘴𝘦, 𝘪𝘴 𝘮𝘶𝘤𝘩 𝘮𝘰𝘳𝘦 𝘵𝘩𝘢𝘯 𝘢 𝘤𝘦𝘭𝘭𝘶𝘭𝘢𝘳 𝘥𝘦𝘧𝘦𝘤𝘵. 𝘔𝘰𝘴𝘵 𝘰𝘧 𝘵𝘩𝘦 𝘤𝘦𝘭𝘭𝘴 𝘪𝘯 𝘢 𝘵𝘶𝘮𝘰𝘳 𝘢𝘳𝘦 𝘴𝘰 𝘥𝘦𝘧𝘦𝘤𝘵𝘪𝘷𝘦 𝘵𝘩𝘢𝘵 𝘵𝘩𝘦𝘺 𝘢𝘳𝘦 𝘪𝘯 𝘵𝘩𝘦 𝘱𝘳𝘰𝘤𝘦𝘴𝘴 𝘰𝘧 𝘥𝘺𝘪𝘯𝘨, 𝘢𝘯𝘥 𝘪𝘯 𝘵𝘩𝘢𝘵 𝘱𝘳𝘰𝘤𝘦𝘴𝘴 𝘵𝘩𝘦𝘺 𝘳𝘦𝘤𝘳𝘶𝘪𝘵 𝘳𝘦𝘱𝘭𝘢𝘤𝘦𝘮𝘦𝘯𝘵 𝘤𝘦𝘭𝘭𝘴, 𝘸𝘩𝘪𝘤𝘩 𝘦𝘹𝘱𝘦𝘳𝘪𝘦𝘯𝘤𝘦 𝘵𝘩𝘦 𝘴𝘢𝘮𝘦 𝘥𝘢𝘮𝘢𝘨𝘪𝘯𝘨 𝘤𝘰𝘯𝘥𝘪𝘵𝘪𝘰𝘯𝘴. 𝙏𝙝𝙚 𝙡𝙤𝙘𝙖𝙡 𝙖𝙣𝙙 𝙧𝙚𝙜𝙞𝙤𝙣𝙖𝙡 𝙚𝙭𝙩𝙧𝙖𝙘𝙚𝙡𝙡𝙪𝙡𝙖𝙧 𝙘𝙤𝙣𝙙𝙞𝙩𝙞𝙤𝙣𝙨, 𝙖𝙣𝙙 𝙩𝙝𝙚 𝙘𝙤𝙣𝙙𝙞𝙩𝙞𝙤𝙣 𝙤𝙛 𝙩𝙝𝙚 𝙝𝙤𝙨𝙩, 𝙖𝙧𝙚 𝙟𝙪𝙨𝙩 𝙖𝙨 𝙘𝙚𝙣𝙩𝙧𝙖𝙡 𝙩𝙤 𝙩𝙝𝙚 𝙙𝙞𝙨𝙚𝙖𝙨𝙚 𝙖𝙨 𝙩𝙝𝙚 𝙛𝙖𝙞𝙡𝙞𝙣𝙜 𝙢𝙞𝙩𝙤𝙘𝙝𝙤𝙣𝙙𝙧𝙞𝙖.”
—Ray Peat, PhD
𝗣𝗨𝗙𝗔, 𝗼𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝘀𝘁𝗿𝗲𝘀𝘀, 𝗮𝗻𝗱 𝗲𝘀𝘁𝗿𝗼𝗴𝗲𝗻
Cancer cannot exist unless there is a presence of polyunsaturated fatty acids (PUFA),[37][38] and carcinogenicity is correlated with the degree of unsaturation of the fatty acid.[39][40]
✺ 𝗪𝗵𝗲𝗻 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀 𝗿𝗲𝘀𝗽𝗼𝗻𝘀𝗲 𝗵𝗮𝗽𝗽𝗲𝗻𝘀 𝗶𝗻 𝘁𝗵𝗲 𝗽𝗿𝗲𝘀𝗲𝗻𝗰𝗲 𝗼𝗳 𝘀𝗮𝘁𝘂𝗿𝗮𝘁𝗲𝗱 𝗳𝗮𝘁𝘁𝘆 𝗮𝗰𝗶𝗱𝘀, 𝘁𝗵𝗲 𝗿𝗲𝘀𝗽𝗼𝗻𝘀𝗲 𝗶𝘀 𝘀𝗲𝗹𝗳-𝗹𝗶𝗺𝗶𝘁𝗶𝗻𝗴, 𝗯𝘂𝘁 𝗶𝗻 𝘁𝗵𝗲 𝗽𝗿𝗲𝘀𝗲𝗻𝗰𝗲 𝗼𝗳 𝗣𝗨𝗙𝗔, 𝗶𝘁 𝗶𝘀 𝘀𝗲𝗹𝗳-𝗮𝗺𝗽𝗹𝗶𝗳𝘆𝗶𝗻𝗴.
This is because PUFAs create catastrophic lipid peroxidation cascades, a chain reaction that cannot occur among highly stable saturated fats. The lipid peroxidation of PUFAs produces protein damage 23 times faster than simple sugars do.[41]
PUFAs are converted to arachidonic acid by phospholipase A2 and from there they are metabolized to prostaglandins, leukotrienes, and thromboxanes.[42]
Prostaglandins activate the HPA axis (physiological stress cascade).[43] Some researchers speculate that prostaglandins are the reason why unsaturated fats promote tumor formation and saturated fats do not.[44]
✺ 𝗧𝗵𝗲𝘀𝗲 𝗣𝗨𝗙𝗔 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘁𝗲𝘀 𝗹𝗲𝗮𝗱 𝘁𝗼 𝗮 𝗰𝗵𝗿𝗼𝗻𝗶𝗰𝗮𝗹𝗹𝘆 𝗶𝗻𝗳𝗹𝗮𝗺𝗲𝗱 𝘀𝘁𝗮𝘁𝗲, 𝗮𝗻𝗱 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗶𝗻𝗳𝗹𝗮𝗺𝗺𝗮𝘁𝗶𝗼𝗻 𝗶𝘀 𝘀𝘁𝗿𝗼𝗻𝗴𝗹𝘆 𝗮𝘀𝘀𝗼𝗰𝗶𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝗰𝗮𝗻𝗰𝗲𝗿 𝗱𝗲𝘃𝗲𝗹𝗼𝗽𝗺𝗲𝗻𝘁.[45][46][47]
An inflamed and injured cell takes up water (edema) and produces lactic acid, losing its ability to respire (hypoxia). This can only occur in metabolic derangements.
𝗚𝗲𝗿𝗺𝗮𝗻 𝗽𝗵𝘆𝘀𝗶𝗰𝗶𝗮𝗻 𝗥𝘂𝗱𝗼𝗹𝗳 𝗩𝗶𝗿𝗰𝗵𝗼𝘄 𝗻𝗼𝘁𝗶𝗰𝗲𝗱 𝘁𝗵𝗮𝘁 𝘁𝘂𝗺𝗼𝗿𝘀 𝗼𝗳𝘁𝗲𝗻 𝗳𝗼𝗿𝗺𝗲𝗱 𝗮𝘁 𝘀𝗶𝘁𝗲𝘀 𝗼𝗳 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗶𝗻𝗷𝘂𝗿𝘆. So common is it for tumors to grow at sites of injury, that in 1862, Virchow suggested previous injury was a precondition for tumor formation.
Swiss researchers pointed out in 2008 that there is a remarkable similarity between a wound and cancer, dubbing cancer the “overhealing” wound.[48]
The Weston A. Price Foundation has done some great work in “alternative” health, but a major pitfall is their emphasis on fermented cod liver oil, a rancid PUFA.
There is an alarming number of WAPF members who have succumbed to various cancers, and it is speculated that the reason is fermented cod liver oil; however, even regular cod liver oil poses a risk since it is also a highly unstable PUFA.
[49]
✺ 𝗘𝘀𝘁𝗿𝗼𝗴𝗲𝗻 𝗽𝗹𝗮𝘆𝘀 𝗮 𝗺𝗮𝗷𝗼𝗿 𝗿𝗼𝗹𝗲 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿 𝗮𝗻𝗱 𝗼𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝘀𝘁𝗿𝗲𝘀𝘀.[50] 𝗔𝗴𝗶𝗻𝗴 𝗯𝗼𝗱𝗶𝗲𝘀 𝗶𝗻𝗰𝗿𝗲𝗮𝘀𝗲 𝘁𝗵𝗲𝗶𝗿 𝘀𝘁𝗼𝗿𝗲𝘀 𝗼𝗳 𝗣𝗨𝗙𝗔,[51] 𝗮𝗺𝗽𝗹𝗶𝗳𝘆𝗶𝗻𝗴 𝘁𝗵𝗲 𝗶𝗻𝗳𝗹𝗮𝗺𝗺𝗮𝘁𝗶𝗼𝗻 𝗼𝗳 𝗲𝘀𝘁𝗿𝗼𝗴𝗲𝗻.
“𝘐𝘯 𝘵𝘩𝘦 𝘜𝘚 𝘢𝘯𝘥 𝘴𝘦𝘷𝘦𝘳𝘢𝘭 𝘰𝘵𝘩𝘦𝘳 𝘤𝘰𝘶𝘯𝘵𝘳𝘪𝘦𝘴, 𝘣𝘦𝘵𝘸𝘦𝘦𝘯 2002 𝘢𝘯𝘥 2005 𝘵𝘩𝘦𝘳𝘦 𝘸𝘢𝘴 𝘢𝘯 𝘶𝘯𝘱𝘳𝘦𝘤𝘦𝘥𝘦𝘯𝘵𝘦𝘥 𝘥𝘦𝘤𝘭𝘪𝘯𝘦 (7% 𝘪𝘯 𝘵𝘩𝘦 𝘜𝘚) 𝘪𝘯 𝘵𝘩𝘦 𝘪𝘯𝘤𝘪𝘥𝘦𝘯𝘤𝘦 𝘰𝘧 𝘣𝘳𝘦𝘢𝘴𝘵 𝘤𝘢𝘯𝘤𝘦𝘳, 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘮𝘦𝘥𝘪𝘤𝘢𝘭 𝘶𝘴𝘦 𝘰𝘧 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯 𝘥𝘦𝘤𝘳𝘦𝘢𝘴𝘦𝘥 𝘧𝘰𝘭𝘭𝘰𝘸𝘪𝘯𝘨 𝘵𝘩𝘦 𝘞𝘰𝘮𝘦𝘯'𝘴 𝘏𝘦𝘢𝘭𝘵𝘩 𝘐𝘯𝘪𝘵𝘪𝘢𝘵𝘪𝘷𝘦 𝘳𝘦𝘱𝘰𝘳𝘵 𝘴𝘩𝘰𝘸𝘪𝘯𝘨 𝘵𝘩𝘢𝘵 𝙚𝙨𝙩𝙧𝙤𝙜𝙚𝙣 𝙘𝙖𝙪𝙨𝙚𝙙 𝙘𝙖𝙣𝙘𝙚𝙧, 𝙙𝙚𝙢𝙚𝙣𝙩𝙞𝙖, 𝙨𝙩𝙧𝙤𝙠𝙚𝙨 𝙖𝙣𝙙 𝙝𝙚𝙖𝙧𝙩 𝙖𝙩𝙩𝙖𝙘𝙠𝙨. 𝘏𝘰𝘸𝘦𝘷𝘦𝘳, 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤 𝘸𝘢𝘴 𝘳𝘦𝘢𝘴𝘴𝘶𝘳𝘦𝘥 𝘢𝘣𝘰𝘶𝘵 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯'𝘴 𝘴𝘢𝘧𝘦𝘵𝘺, 𝘣𝘳𝘦𝘢𝘴𝘵 𝘤𝘢𝘯𝘤𝘦𝘳 𝘪𝘯𝘤𝘪𝘥𝘦𝘯𝘤𝘦 𝘣𝘦𝘨𝘢𝘯 𝘪𝘯𝘤𝘳𝘦𝘢𝘴𝘪𝘯𝘨 𝘢𝘨𝘢𝘪𝘯 𝘦𝘢𝘤𝘩 𝘺𝘦𝘢𝘳.”
—Ray Peat, PhD
Cancer cannot exist unless there is a presence of polyunsaturated fatty acids (PUFA),[37][38] and carcinogenicity is correlated with the degree of unsaturation of the fatty acid.[39][40]
✺ 𝗪𝗵𝗲𝗻 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀 𝗿𝗲𝘀𝗽𝗼𝗻𝘀𝗲 𝗵𝗮𝗽𝗽𝗲𝗻𝘀 𝗶𝗻 𝘁𝗵𝗲 𝗽𝗿𝗲𝘀𝗲𝗻𝗰𝗲 𝗼𝗳 𝘀𝗮𝘁𝘂𝗿𝗮𝘁𝗲𝗱 𝗳𝗮𝘁𝘁𝘆 𝗮𝗰𝗶𝗱𝘀, 𝘁𝗵𝗲 𝗿𝗲𝘀𝗽𝗼𝗻𝘀𝗲 𝗶𝘀 𝘀𝗲𝗹𝗳-𝗹𝗶𝗺𝗶𝘁𝗶𝗻𝗴, 𝗯𝘂𝘁 𝗶𝗻 𝘁𝗵𝗲 𝗽𝗿𝗲𝘀𝗲𝗻𝗰𝗲 𝗼𝗳 𝗣𝗨𝗙𝗔, 𝗶𝘁 𝗶𝘀 𝘀𝗲𝗹𝗳-𝗮𝗺𝗽𝗹𝗶𝗳𝘆𝗶𝗻𝗴.
This is because PUFAs create catastrophic lipid peroxidation cascades, a chain reaction that cannot occur among highly stable saturated fats. The lipid peroxidation of PUFAs produces protein damage 23 times faster than simple sugars do.[41]
PUFAs are converted to arachidonic acid by phospholipase A2 and from there they are metabolized to prostaglandins, leukotrienes, and thromboxanes.[42]
Prostaglandins activate the HPA axis (physiological stress cascade).[43] Some researchers speculate that prostaglandins are the reason why unsaturated fats promote tumor formation and saturated fats do not.[44]
✺ 𝗧𝗵𝗲𝘀𝗲 𝗣𝗨𝗙𝗔 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘁𝗲𝘀 𝗹𝗲𝗮𝗱 𝘁𝗼 𝗮 𝗰𝗵𝗿𝗼𝗻𝗶𝗰𝗮𝗹𝗹𝘆 𝗶𝗻𝗳𝗹𝗮𝗺𝗲𝗱 𝘀𝘁𝗮𝘁𝗲, 𝗮𝗻𝗱 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗶𝗻𝗳𝗹𝗮𝗺𝗺𝗮𝘁𝗶𝗼𝗻 𝗶𝘀 𝘀𝘁𝗿𝗼𝗻𝗴𝗹𝘆 𝗮𝘀𝘀𝗼𝗰𝗶𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝗰𝗮𝗻𝗰𝗲𝗿 𝗱𝗲𝘃𝗲𝗹𝗼𝗽𝗺𝗲𝗻𝘁.[45][46][47]
An inflamed and injured cell takes up water (edema) and produces lactic acid, losing its ability to respire (hypoxia). This can only occur in metabolic derangements.
𝗚𝗲𝗿𝗺𝗮𝗻 𝗽𝗵𝘆𝘀𝗶𝗰𝗶𝗮𝗻 𝗥𝘂𝗱𝗼𝗹𝗳 𝗩𝗶𝗿𝗰𝗵𝗼𝘄 𝗻𝗼𝘁𝗶𝗰𝗲𝗱 𝘁𝗵𝗮𝘁 𝘁𝘂𝗺𝗼𝗿𝘀 𝗼𝗳𝘁𝗲𝗻 𝗳𝗼𝗿𝗺𝗲𝗱 𝗮𝘁 𝘀𝗶𝘁𝗲𝘀 𝗼𝗳 𝗰𝗵𝗿𝗼𝗻𝗶𝗰 𝗶𝗻𝗷𝘂𝗿𝘆. So common is it for tumors to grow at sites of injury, that in 1862, Virchow suggested previous injury was a precondition for tumor formation.
Swiss researchers pointed out in 2008 that there is a remarkable similarity between a wound and cancer, dubbing cancer the “overhealing” wound.[48]
The Weston A. Price Foundation has done some great work in “alternative” health, but a major pitfall is their emphasis on fermented cod liver oil, a rancid PUFA.
There is an alarming number of WAPF members who have succumbed to various cancers, and it is speculated that the reason is fermented cod liver oil; however, even regular cod liver oil poses a risk since it is also a highly unstable PUFA.
[49]
✺ 𝗘𝘀𝘁𝗿𝗼𝗴𝗲𝗻 𝗽𝗹𝗮𝘆𝘀 𝗮 𝗺𝗮𝗷𝗼𝗿 𝗿𝗼𝗹𝗲 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿 𝗮𝗻𝗱 𝗼𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝘀𝘁𝗿𝗲𝘀𝘀.[50] 𝗔𝗴𝗶𝗻𝗴 𝗯𝗼𝗱𝗶𝗲𝘀 𝗶𝗻𝗰𝗿𝗲𝗮𝘀𝗲 𝘁𝗵𝗲𝗶𝗿 𝘀𝘁𝗼𝗿𝗲𝘀 𝗼𝗳 𝗣𝗨𝗙𝗔,[51] 𝗮𝗺𝗽𝗹𝗶𝗳𝘆𝗶𝗻𝗴 𝘁𝗵𝗲 𝗶𝗻𝗳𝗹𝗮𝗺𝗺𝗮𝘁𝗶𝗼𝗻 𝗼𝗳 𝗲𝘀𝘁𝗿𝗼𝗴𝗲𝗻.
“𝘐𝘯 𝘵𝘩𝘦 𝘜𝘚 𝘢𝘯𝘥 𝘴𝘦𝘷𝘦𝘳𝘢𝘭 𝘰𝘵𝘩𝘦𝘳 𝘤𝘰𝘶𝘯𝘵𝘳𝘪𝘦𝘴, 𝘣𝘦𝘵𝘸𝘦𝘦𝘯 2002 𝘢𝘯𝘥 2005 𝘵𝘩𝘦𝘳𝘦 𝘸𝘢𝘴 𝘢𝘯 𝘶𝘯𝘱𝘳𝘦𝘤𝘦𝘥𝘦𝘯𝘵𝘦𝘥 𝘥𝘦𝘤𝘭𝘪𝘯𝘦 (7% 𝘪𝘯 𝘵𝘩𝘦 𝘜𝘚) 𝘪𝘯 𝘵𝘩𝘦 𝘪𝘯𝘤𝘪𝘥𝘦𝘯𝘤𝘦 𝘰𝘧 𝘣𝘳𝘦𝘢𝘴𝘵 𝘤𝘢𝘯𝘤𝘦𝘳, 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘮𝘦𝘥𝘪𝘤𝘢𝘭 𝘶𝘴𝘦 𝘰𝘧 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯 𝘥𝘦𝘤𝘳𝘦𝘢𝘴𝘦𝘥 𝘧𝘰𝘭𝘭𝘰𝘸𝘪𝘯𝘨 𝘵𝘩𝘦 𝘞𝘰𝘮𝘦𝘯'𝘴 𝘏𝘦𝘢𝘭𝘵𝘩 𝘐𝘯𝘪𝘵𝘪𝘢𝘵𝘪𝘷𝘦 𝘳𝘦𝘱𝘰𝘳𝘵 𝘴𝘩𝘰𝘸𝘪𝘯𝘨 𝘵𝘩𝘢𝘵 𝙚𝙨𝙩𝙧𝙤𝙜𝙚𝙣 𝙘𝙖𝙪𝙨𝙚𝙙 𝙘𝙖𝙣𝙘𝙚𝙧, 𝙙𝙚𝙢𝙚𝙣𝙩𝙞𝙖, 𝙨𝙩𝙧𝙤𝙠𝙚𝙨 𝙖𝙣𝙙 𝙝𝙚𝙖𝙧𝙩 𝙖𝙩𝙩𝙖𝙘𝙠𝙨. 𝘏𝘰𝘸𝘦𝘷𝘦𝘳, 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘱𝘶𝘣𝘭𝘪𝘤 𝘸𝘢𝘴 𝘳𝘦𝘢𝘴𝘴𝘶𝘳𝘦𝘥 𝘢𝘣𝘰𝘶𝘵 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯'𝘴 𝘴𝘢𝘧𝘦𝘵𝘺, 𝘣𝘳𝘦𝘢𝘴𝘵 𝘤𝘢𝘯𝘤𝘦𝘳 𝘪𝘯𝘤𝘪𝘥𝘦𝘯𝘤𝘦 𝘣𝘦𝘨𝘢𝘯 𝘪𝘯𝘤𝘳𝘦𝘢𝘴𝘪𝘯𝘨 𝘢𝘨𝘢𝘪𝘯 𝘦𝘢𝘤𝘩 𝘺𝘦𝘢𝘳.”
—Ray Peat, PhD
𝗘𝗳𝗳𝗲𝗰𝘁𝘀 𝗼𝗯𝘀𝗲𝗿𝘃𝗲𝗱 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿
Otto Warburg was a WWII-era German physiologist, medical doctor, and Nobel laureate. He is the father of cancer research, and why we call the aerobic glycolysis seen in cancer the “𝗪𝗮𝗿𝗯𝘂𝗿𝗴 𝗲𝗳𝗳𝗲𝗰𝘁."
In 1931, he was awarded the Nobel Prize for his "discovery of the nature and mode of action of the respiratory enzyme". Perhaps most importantly, Warburg discovered that 𝘁𝘂𝗺𝗼𝗿𝘀 𝗽𝗿𝗼𝗱𝘂𝗰𝗲 𝗹𝗮𝗿𝗴𝗲 𝗾𝘂𝗮𝗻𝘁𝗶𝘁𝗶𝗲𝘀 𝗼𝗳 𝗹𝗮𝗰𝘁𝗶𝗰 𝗮𝗰𝗶𝗱.
Warburg described cancer as having a respiratory defect that made it lack the “𝗣𝗮𝘀𝘁𝗲𝘂𝗿 𝗲𝗳𝗳𝗲𝗰𝘁” (the observation that oxygen causes yeast to stop fermenting).
Remember “lactic acid fermentation” and “cancer metabolism”?
✺ 𝗜𝗻 𝟭𝟵𝟳𝟬, 𝗗𝗿. 𝗪𝗮𝗿𝗯𝘂𝗿𝗴 𝗮𝗻𝗱 𝗵𝗶𝘀 𝗰𝗼𝗹𝗹𝗲𝗮𝗴𝘂𝗲𝘀 𝗱𝗲𝗺𝗼𝗻𝘀𝘁𝗿𝗮𝘁𝗲𝗱 𝘁𝗵𝗲𝘆 𝗰𝗼𝘂𝗹𝗱 𝗶𝗻𝗱𝘂𝗰𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝗻 𝗻𝗼𝗿𝗺𝗮𝗹 𝗰𝗲𝗹𝗹𝘀 𝘀𝗽𝗲𝗰𝗶𝗳𝗶𝗰𝗮𝗹𝗹𝘆 𝗯𝘆 𝗱𝗲𝗽𝗿𝗶𝘃𝗶𝗻𝗴 𝘁𝗵𝗲𝗺 𝗼𝗳 𝘁𝗵𝗶𝗮𝗺𝗶𝗻𝗲.[52] Thiamine is the primary B vitamin involved in burning glucose for energy.
𝗪𝗵𝘆 𝗶𝘀 𝗮 𝗰𝗲𝗹𝗹’𝘀 𝗶𝗻𝗮𝗯𝗶𝗹𝗶𝘁𝘆 𝘁𝗼 𝗼𝘅𝗶𝗱𝗶𝘇𝗲 𝗴𝗹𝘂𝗰𝗼𝘀𝗲 𝗮 𝗽𝗿𝗼𝗯𝗹𝗲𝗺?
The “𝗥𝗮𝗻𝗱𝗹𝗲 𝗲𝗳𝗳𝗲𝗰𝘁” is the competition between fats and carbohydrates to be used for fuel. Fats burn in the flame of carbohydrates, but excessive fatty acid oxidation (FAO) can shift the Randle cycle too much in favor of FAO, inhibiting glucose oxidation.[53] This failure to use glucose is a failure in oxidative metabolism, and a failure in oxidative metabolism underpins every chronic illness, especially cancer.
Since 1909, there has been an over 1000-fold increase in seed oil (PUFA) consumption,[54] and this creates a multiplier effect on the damage done to the metabolism.[55][56][57] The initial fuel of FAO prefers PUFA as substrate[58], so, as Georgi Dinkov explains, “𝘗𝘜𝘍𝘈 𝘴𝘦𝘦𝘮 𝘵𝘰 𝘩𝘢𝘷𝘦 𝘢 𝘶𝘯𝘪𝘲𝘶𝘦 𝘳𝘰𝘭𝘦 𝘢𝘴 𝘯𝘰𝘵 𝘰𝘯𝘭𝘺 𝘢 𝘶𝘯𝘪𝘷𝘦𝘳𝘴𝘢𝘭𝘭𝘺-𝘤𝘰𝘯𝘴𝘶𝘮𝘦𝘥 𝘮𝘦𝘵𝘢𝘣𝘰𝘭𝘪𝘤 𝘪𝘯𝘩𝘪𝘣𝘪𝘵𝘰𝘳, 𝘣𝘶𝘵 𝘢𝘭𝘴𝘰 𝘢𝘴 𝘵𝘩𝘦 𝘱𝘳𝘦𝘧𝘦𝘳𝘳𝘦𝘥 𝘧𝘶𝘦𝘭 𝘰𝘧 𝘤𝘢𝘯𝘤𝘦𝘳.”
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗱𝗼𝗲𝘀 𝗻𝗼𝘁 𝗵𝗮𝘃𝗲 𝗮 𝘃𝗼𝗿𝗮𝗰𝗶𝗼𝘂𝘀 𝗮𝗽𝗽𝗲𝘁𝗶𝘁𝗲 𝗳𝗼𝗿 𝘀𝘂𝗴𝗮𝗿, 𝗯𝘂𝘁 𝗿𝗮𝘁𝗵𝗲𝗿 𝗳𝗮𝘁𝘁𝘆 𝗮𝗰𝗶𝗱𝘀 𝗮𝗻𝗱 𝘁𝗵𝗲 𝗮𝗺𝗶𝗻𝗼 𝗮𝗰𝗶𝗱 𝗴𝗹𝘂𝘁𝗮𝗺𝗶𝗻𝗲.
A study showed that glioblastoma is primarily a mitochondrial metabolic disease driven by fermentation, and that restricting glutamine was very effective.[59]
The “cancer metabolism” is an incredibly inefficient one, wasting glucose, so naturally, many come to the conclusion that dietary glucose restriction is the answer. This is misguided; cancer cells love to use fat for survival.[60] In fact, excessive lipolysis in the absence of adequate carbs is what turns on the “Warburg effect,” leading to issues oxidizing glucose (The Randle effect), which then leads to lactic acid and the stress cascade.[61] 𝗧𝗵𝗲 𝗮𝗻𝘀𝘄𝗲𝗿 𝗶𝘀 𝗻𝗼𝘁 𝗴𝗹𝘂𝗰𝗼𝘀𝗲 𝗿𝗲𝘀𝘁𝗿𝗶𝗰𝘁𝗶𝗼𝗻 𝗯𝘂𝘁 𝗿𝗮𝘁𝗵𝗲𝗿 𝗿𝗲𝗽𝗮𝗶𝗿𝗶𝗻𝗴 𝘁𝗵𝗲 𝗯𝗼𝗱𝘆’𝘀 𝗮𝗯𝗶𝗹𝗶𝘁𝘆 𝘁𝗼 𝘂𝘀𝗲 𝗶𝘁.
Otto Warburg was a WWII-era German physiologist, medical doctor, and Nobel laureate. He is the father of cancer research, and why we call the aerobic glycolysis seen in cancer the “𝗪𝗮𝗿𝗯𝘂𝗿𝗴 𝗲𝗳𝗳𝗲𝗰𝘁."
In 1931, he was awarded the Nobel Prize for his "discovery of the nature and mode of action of the respiratory enzyme". Perhaps most importantly, Warburg discovered that 𝘁𝘂𝗺𝗼𝗿𝘀 𝗽𝗿𝗼𝗱𝘂𝗰𝗲 𝗹𝗮𝗿𝗴𝗲 𝗾𝘂𝗮𝗻𝘁𝗶𝘁𝗶𝗲𝘀 𝗼𝗳 𝗹𝗮𝗰𝘁𝗶𝗰 𝗮𝗰𝗶𝗱.
Warburg described cancer as having a respiratory defect that made it lack the “𝗣𝗮𝘀𝘁𝗲𝘂𝗿 𝗲𝗳𝗳𝗲𝗰𝘁” (the observation that oxygen causes yeast to stop fermenting).
Remember “lactic acid fermentation” and “cancer metabolism”?
✺ 𝗜𝗻 𝟭𝟵𝟳𝟬, 𝗗𝗿. 𝗪𝗮𝗿𝗯𝘂𝗿𝗴 𝗮𝗻𝗱 𝗵𝗶𝘀 𝗰𝗼𝗹𝗹𝗲𝗮𝗴𝘂𝗲𝘀 𝗱𝗲𝗺𝗼𝗻𝘀𝘁𝗿𝗮𝘁𝗲𝗱 𝘁𝗵𝗲𝘆 𝗰𝗼𝘂𝗹𝗱 𝗶𝗻𝗱𝘂𝗰𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗶𝗻 𝗻𝗼𝗿𝗺𝗮𝗹 𝗰𝗲𝗹𝗹𝘀 𝘀𝗽𝗲𝗰𝗶𝗳𝗶𝗰𝗮𝗹𝗹𝘆 𝗯𝘆 𝗱𝗲𝗽𝗿𝗶𝘃𝗶𝗻𝗴 𝘁𝗵𝗲𝗺 𝗼𝗳 𝘁𝗵𝗶𝗮𝗺𝗶𝗻𝗲.[52] Thiamine is the primary B vitamin involved in burning glucose for energy.
𝗪𝗵𝘆 𝗶𝘀 𝗮 𝗰𝗲𝗹𝗹’𝘀 𝗶𝗻𝗮𝗯𝗶𝗹𝗶𝘁𝘆 𝘁𝗼 𝗼𝘅𝗶𝗱𝗶𝘇𝗲 𝗴𝗹𝘂𝗰𝗼𝘀𝗲 𝗮 𝗽𝗿𝗼𝗯𝗹𝗲𝗺?
The “𝗥𝗮𝗻𝗱𝗹𝗲 𝗲𝗳𝗳𝗲𝗰𝘁” is the competition between fats and carbohydrates to be used for fuel. Fats burn in the flame of carbohydrates, but excessive fatty acid oxidation (FAO) can shift the Randle cycle too much in favor of FAO, inhibiting glucose oxidation.[53] This failure to use glucose is a failure in oxidative metabolism, and a failure in oxidative metabolism underpins every chronic illness, especially cancer.
Since 1909, there has been an over 1000-fold increase in seed oil (PUFA) consumption,[54] and this creates a multiplier effect on the damage done to the metabolism.[55][56][57] The initial fuel of FAO prefers PUFA as substrate[58], so, as Georgi Dinkov explains, “𝘗𝘜𝘍𝘈 𝘴𝘦𝘦𝘮 𝘵𝘰 𝘩𝘢𝘷𝘦 𝘢 𝘶𝘯𝘪𝘲𝘶𝘦 𝘳𝘰𝘭𝘦 𝘢𝘴 𝘯𝘰𝘵 𝘰𝘯𝘭𝘺 𝘢 𝘶𝘯𝘪𝘷𝘦𝘳𝘴𝘢𝘭𝘭𝘺-𝘤𝘰𝘯𝘴𝘶𝘮𝘦𝘥 𝘮𝘦𝘵𝘢𝘣𝘰𝘭𝘪𝘤 𝘪𝘯𝘩𝘪𝘣𝘪𝘵𝘰𝘳, 𝘣𝘶𝘵 𝘢𝘭𝘴𝘰 𝘢𝘴 𝘵𝘩𝘦 𝘱𝘳𝘦𝘧𝘦𝘳𝘳𝘦𝘥 𝘧𝘶𝘦𝘭 𝘰𝘧 𝘤𝘢𝘯𝘤𝘦𝘳.”
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗱𝗼𝗲𝘀 𝗻𝗼𝘁 𝗵𝗮𝘃𝗲 𝗮 𝘃𝗼𝗿𝗮𝗰𝗶𝗼𝘂𝘀 𝗮𝗽𝗽𝗲𝘁𝗶𝘁𝗲 𝗳𝗼𝗿 𝘀𝘂𝗴𝗮𝗿, 𝗯𝘂𝘁 𝗿𝗮𝘁𝗵𝗲𝗿 𝗳𝗮𝘁𝘁𝘆 𝗮𝗰𝗶𝗱𝘀 𝗮𝗻𝗱 𝘁𝗵𝗲 𝗮𝗺𝗶𝗻𝗼 𝗮𝗰𝗶𝗱 𝗴𝗹𝘂𝘁𝗮𝗺𝗶𝗻𝗲.
A study showed that glioblastoma is primarily a mitochondrial metabolic disease driven by fermentation, and that restricting glutamine was very effective.[59]
The “cancer metabolism” is an incredibly inefficient one, wasting glucose, so naturally, many come to the conclusion that dietary glucose restriction is the answer. This is misguided; cancer cells love to use fat for survival.[60] In fact, excessive lipolysis in the absence of adequate carbs is what turns on the “Warburg effect,” leading to issues oxidizing glucose (The Randle effect), which then leads to lactic acid and the stress cascade.[61] 𝗧𝗵𝗲 𝗮𝗻𝘀𝘄𝗲𝗿 𝗶𝘀 𝗻𝗼𝘁 𝗴𝗹𝘂𝗰𝗼𝘀𝗲 𝗿𝗲𝘀𝘁𝗿𝗶𝗰𝘁𝗶𝗼𝗻 𝗯𝘂𝘁 𝗿𝗮𝘁𝗵𝗲𝗿 𝗿𝗲𝗽𝗮𝗶𝗿𝗶𝗻𝗴 𝘁𝗵𝗲 𝗯𝗼𝗱𝘆’𝘀 𝗮𝗯𝗶𝗹𝗶𝘁𝘆 𝘁𝗼 𝘂𝘀𝗲 𝗶𝘁.

𝗛𝗲𝗿𝗲’𝘀 𝗵𝗼𝘄 𝗶𝗻𝗱𝗲𝗽𝗲𝗻𝗱𝗲𝗻𝘁 𝗿𝗲𝘀𝗲𝗮𝗿𝗰𝗵𝗲𝗿 𝗚𝗲𝗼𝗿𝗴𝗶 𝗗𝗶𝗻𝗸𝗼𝘃 𝗲𝘅𝗽𝗹𝗮𝗶𝗻𝘀 𝘁𝗵𝗲 𝗽𝗿𝗼𝗰𝗲𝘀𝘀:
- Chronic stress leads to excessive fatty acid oxidation (FAO).
- Excessive FAO leads to poor glucose oxidation.[62]
Excessive FAO means less CO2 because fats produce less CO2 per unit compared to glucose.
Less CO2 means hypoxia (due to the Haldane-Bohr effect) and more lactic acid (since CO2 and lactic acid are inversely correlated). Lactic acid can potently stimulate tumor growth.[63]
A reduced state in the cell leads to reverse electron transfer (RET) in the electron transport chain (ETC) and eventually the cell begins to dismantle its ETC components.[64]
- RET and excessive FAO means more reactive oxygen species (ROS),[65][66] exacerbating the reductive state of the cell.
- This metabolic derangement becomes self-perpetuating.
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗶𝘀𝗻’𝘁 𝘀𝗼𝗺𝗲 𝗿𝗮𝗻𝗱𝗼𝗺, 𝗴𝗲𝗻𝗲𝘁𝗶𝗰𝗮𝗹𝗹𝘆 𝗽𝗿𝗲𝗱𝗲𝘁𝗲𝗿𝗺𝗶𝗻𝗲𝗱 𝗺𝘂𝘁𝗮𝘁𝗶𝗼𝗻—𝗶𝘁’𝘀 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀𝗲𝗱 𝗰𝗲𝗹𝗹 𝗮𝗻𝗱 𝗮 𝗽𝗿𝗼𝗱𝘂𝗰𝘁 𝗼𝗳 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀𝗲𝗱 𝗲𝗻𝘃𝗶𝗿𝗼𝗻𝗺𝗲𝗻𝘁.
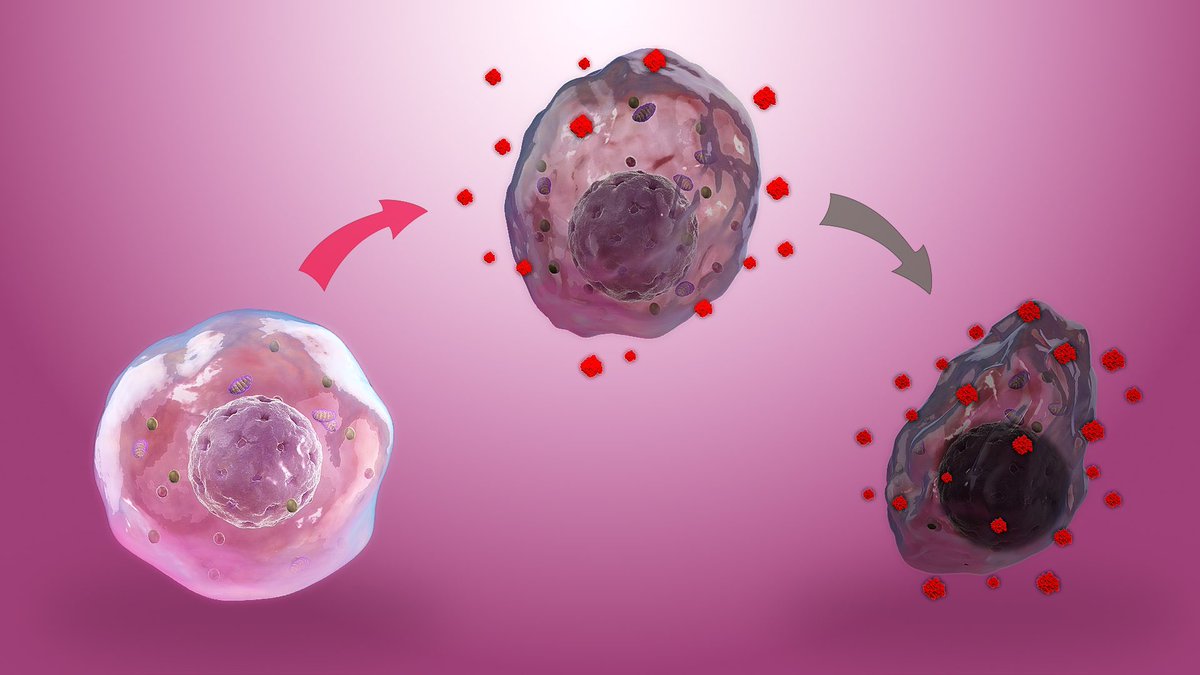
Peat spoke of the cancer cell as defective and weak, with a short lifespan. He explained that every time the cancer cell dies, it is replaced by a similarly defective cell. No matter how you attempt to kill the cancer cell, that injured area is likely going to keep conjuring new, defective replacements. Furthermore, the injury caused by killing the cancer stimulates faster replacement in most cases than just leaving it alone.
✺ 𝗧𝗵𝗲 𝗴𝗼𝗮𝗹 𝗶𝘀 𝘁𝗼 𝗰𝗼𝗿𝗿𝗲𝗰𝘁 𝘁𝗵𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺 𝗼𝗳 𝗯𝗼𝘁𝗵 𝘁𝗵𝗲 𝘁𝘂𝗺𝗼𝗿 𝗮𝗻𝗱 𝘁𝗵𝗲 𝗵𝗼𝘀𝘁.
“𝘖𝘯𝘤𝘰𝘭𝘰𝘨𝘪𝘤𝘢𝘭 𝘱𝘢𝘵𝘩𝘰𝘭𝘰𝘨𝘪𝘴𝘵𝘴, 𝘭𝘰𝘰𝘬𝘪𝘯𝘨 𝘢𝘵 𝘴𝘭𝘪𝘤𝘦𝘴 𝘰𝘧 𝘢 𝘵𝘶𝘮𝘰𝘳, 𝘣𝘦𝘭𝘪𝘦𝘷𝘦 𝘵𝘩𝘦𝘺 𝘤𝘢𝘯 𝘨𝘶𝘦𝘴𝘴 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘤𝘦𝘭𝘭𝘴 𝘩𝘢𝘷𝘦 𝘢𝘯 𝘦𝘷𝘪𝘭 𝘪𝘯𝘵𝘦𝘯𝘵𝘪𝘰𝘯. 𝘏𝘰𝘸𝘦𝘷𝘦𝘳, 𝘣𝘪𝘰𝘭𝘰𝘨𝘪𝘴𝘵𝘴 𝘴𝘵𝘶𝘥𝘺𝘪𝘯𝘨 𝘭𝘪𝘷𝘪𝘯𝘨 𝘤𝘦𝘭𝘭𝘴 𝘧𝘪𝘯𝘥 𝘵𝘩𝘢𝘵 𝙘𝙚𝙡𝙡𝙨 𝙘𝙖𝙣 𝙙𝙤 𝙤𝙣𝙡𝙮 𝙬𝙝𝙖𝙩 𝙩𝙝𝙚𝙮 𝙖𝙧𝙚 𝙖𝙡𝙡𝙤𝙬𝙚𝙙 𝙩𝙤 𝙙𝙤 𝙗𝙮 𝙩𝙝𝙚𝙞𝙧 𝙚𝙣𝙫𝙞𝙧𝙤𝙣𝙢𝙚𝙣𝙩.”
—Ray Peat, PhD
- Chronic stress leads to excessive fatty acid oxidation (FAO).
- Excessive FAO leads to poor glucose oxidation.[62]
Excessive FAO means less CO2 because fats produce less CO2 per unit compared to glucose.
Less CO2 means hypoxia (due to the Haldane-Bohr effect) and more lactic acid (since CO2 and lactic acid are inversely correlated). Lactic acid can potently stimulate tumor growth.[63]
A reduced state in the cell leads to reverse electron transfer (RET) in the electron transport chain (ETC) and eventually the cell begins to dismantle its ETC components.[64]
- RET and excessive FAO means more reactive oxygen species (ROS),[65][66] exacerbating the reductive state of the cell.
- This metabolic derangement becomes self-perpetuating.
✺ 𝗖𝗮𝗻𝗰𝗲𝗿 𝗶𝘀𝗻’𝘁 𝘀𝗼𝗺𝗲 𝗿𝗮𝗻𝗱𝗼𝗺, 𝗴𝗲𝗻𝗲𝘁𝗶𝗰𝗮𝗹𝗹𝘆 𝗽𝗿𝗲𝗱𝗲𝘁𝗲𝗿𝗺𝗶𝗻𝗲𝗱 𝗺𝘂𝘁𝗮𝘁𝗶𝗼𝗻—𝗶𝘁’𝘀 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀𝗲𝗱 𝗰𝗲𝗹𝗹 𝗮𝗻𝗱 𝗮 𝗽𝗿𝗼𝗱𝘂𝗰𝘁 𝗼𝗳 𝗮 𝘀𝘁𝗿𝗲𝘀𝘀𝗲𝗱 𝗲𝗻𝘃𝗶𝗿𝗼𝗻𝗺𝗲𝗻𝘁.
Peat spoke of the cancer cell as defective and weak, with a short lifespan. He explained that every time the cancer cell dies, it is replaced by a similarly defective cell. No matter how you attempt to kill the cancer cell, that injured area is likely going to keep conjuring new, defective replacements. Furthermore, the injury caused by killing the cancer stimulates faster replacement in most cases than just leaving it alone.
✺ 𝗧𝗵𝗲 𝗴𝗼𝗮𝗹 𝗶𝘀 𝘁𝗼 𝗰𝗼𝗿𝗿𝗲𝗰𝘁 𝘁𝗵𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺 𝗼𝗳 𝗯𝗼𝘁𝗵 𝘁𝗵𝗲 𝘁𝘂𝗺𝗼𝗿 𝗮𝗻𝗱 𝘁𝗵𝗲 𝗵𝗼𝘀𝘁.
“𝘖𝘯𝘤𝘰𝘭𝘰𝘨𝘪𝘤𝘢𝘭 𝘱𝘢𝘵𝘩𝘰𝘭𝘰𝘨𝘪𝘴𝘵𝘴, 𝘭𝘰𝘰𝘬𝘪𝘯𝘨 𝘢𝘵 𝘴𝘭𝘪𝘤𝘦𝘴 𝘰𝘧 𝘢 𝘵𝘶𝘮𝘰𝘳, 𝘣𝘦𝘭𝘪𝘦𝘷𝘦 𝘵𝘩𝘦𝘺 𝘤𝘢𝘯 𝘨𝘶𝘦𝘴𝘴 𝘸𝘩𝘦𝘯 𝘵𝘩𝘦 𝘤𝘦𝘭𝘭𝘴 𝘩𝘢𝘷𝘦 𝘢𝘯 𝘦𝘷𝘪𝘭 𝘪𝘯𝘵𝘦𝘯𝘵𝘪𝘰𝘯. 𝘏𝘰𝘸𝘦𝘷𝘦𝘳, 𝘣𝘪𝘰𝘭𝘰𝘨𝘪𝘴𝘵𝘴 𝘴𝘵𝘶𝘥𝘺𝘪𝘯𝘨 𝘭𝘪𝘷𝘪𝘯𝘨 𝘤𝘦𝘭𝘭𝘴 𝘧𝘪𝘯𝘥 𝘵𝘩𝘢𝘵 𝙘𝙚𝙡𝙡𝙨 𝙘𝙖𝙣 𝙙𝙤 𝙤𝙣𝙡𝙮 𝙬𝙝𝙖𝙩 𝙩𝙝𝙚𝙮 𝙖𝙧𝙚 𝙖𝙡𝙡𝙤𝙬𝙚𝙙 𝙩𝙤 𝙙𝙤 𝙗𝙮 𝙩𝙝𝙚𝙞𝙧 𝙚𝙣𝙫𝙞𝙧𝙤𝙣𝙢𝙚𝙣𝙩.”
—Ray Peat, PhD

𝗪𝗵𝗼 𝗲𝗹𝘀𝗲 𝘀𝗮𝘄 𝗰𝗮𝗻𝗰𝗲𝗿 𝗮𝘀 𝗮 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝗰 𝗱𝗲𝗿𝗮𝗻𝗴𝗲𝗺𝗲𝗻𝘁?
• Albert Szent-Györgyi, Hungarian biochemist and Nobel laureate.
• William F. Koch, medical doctor and pharmaceutical entrepreneur.
• Gilbert Ling, a Chinese-born American cell physiologist, biochemist and scientific investigator. Without Ling’s theory of cellular water structure, the MRI wouldn’t exist.
• Max Gerson, a German-born American physician who developed the Gerson Therapy, a dietary-based treatment that he used to cure cancer and other chronic, degenerative diseases.
• Thomas Seyfried, an American professor of biology, genetics, and biochemistry with over 150 peer-reviewed publications.
• Albert Szent-Györgyi, Hungarian biochemist and Nobel laureate.
• William F. Koch, medical doctor and pharmaceutical entrepreneur.
• Gilbert Ling, a Chinese-born American cell physiologist, biochemist and scientific investigator. Without Ling’s theory of cellular water structure, the MRI wouldn’t exist.
• Max Gerson, a German-born American physician who developed the Gerson Therapy, a dietary-based treatment that he used to cure cancer and other chronic, degenerative diseases.
• Thomas Seyfried, an American professor of biology, genetics, and biochemistry with over 150 peer-reviewed publications.
𝗗𝗿. 𝗕𝘂𝘁𝗲𝘆𝗸𝗼, 𝗖𝗢𝟮, 𝗮𝗻𝗱 𝘁𝗵𝗲 “𝗕𝗼𝗵𝗿 𝗲𝗳𝗳𝗲𝗰𝘁”
“𝘍𝘰𝘳 𝘰𝘷𝘦𝘳 30 𝘺𝘦𝘢𝘳𝘴–𝘧𝘳𝘰𝘮 𝘖𝘤𝘵𝘰𝘣𝘦𝘳 1952 𝘵𝘰 𝘚𝘦𝘱𝘵𝘦𝘮𝘣𝘦𝘳 1985–𝘵𝘩𝘦 𝘮𝘦𝘥𝘪𝘤𝘢𝘭 𝘦𝘴𝘵𝘢𝘣𝘭𝘪𝘴𝘩𝘮𝘦𝘯𝘵 𝘩𝘶𝘴𝘩𝘦𝘥 𝘶𝘱 𝘮𝘺 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘺. 𝘐𝘵 𝘥𝘪𝘥 𝘦𝘷𝘦𝘳𝘺𝘵𝘩𝘪𝘯𝘨 𝘵𝘰 𝘵𝘳𝘢𝘮𝘱𝘭𝘦 𝘰𝘯 𝘢𝘯𝘥 𝘥𝘦𝘴𝘵𝘳𝘰𝘺 𝘵𝘩𝘦 𝘴𝘵𝘳𝘰𝘯𝘨𝘦𝘴𝘵 𝘸𝘦𝘢𝘱𝘰𝘯 𝘪𝘯 𝘵𝘩𝘦 𝘧𝘪𝘨𝘩𝘵 𝘢𝘨𝘢𝘪𝘯𝘴𝘵 𝘮𝘢𝘯𝘺 𝘮𝘰𝘥𝘦𝘳𝘯 𝘥𝘪𝘴𝘦𝘢𝘴𝘦𝘴. 𝙄 𝙬𝙖𝙨 𝙘𝙖𝙡𝙡𝙚𝙙 𝙖 𝙘𝙝𝙖𝙧𝙡𝙖𝙩𝙖𝙣, 𝙖 𝙨𝙘𝙝𝙞𝙯𝙤𝙥𝙝𝙧𝙚𝙣𝙞𝙘 𝙖𝙣𝙙 𝙖 𝙧𝙖𝙫𝙞𝙣𝙜 𝙣𝙪𝙩𝙩𝙚𝙧, 𝙖𝙢𝙤𝙣𝙜 𝙤𝙩𝙝𝙚𝙧 𝙣𝙖𝙢𝙚𝙨. 𝙏𝙝𝙚𝙮 𝙩𝙧𝙞𝙚𝙙 𝙩𝙤 𝙥𝙤𝙞𝙨𝙤𝙣 𝙢𝙚 𝙩𝙝𝙧𝙚𝙚 𝙩𝙞𝙢𝙚𝙨, 𝙖𝙣𝙙 𝙤𝙧𝙜𝙖𝙣𝙞𝙯𝙚𝙙 𝙩𝙬𝙤 𝙘𝙖𝙧 𝙘𝙧𝙖𝙨𝙝𝙚𝙨. 𝙏𝙝𝙚𝙧𝙚 𝙬𝙚𝙧𝙚 𝙨𝙚𝙫𝙚𝙧𝙖𝙡 𝙖𝙩𝙩𝙚𝙢𝙥𝙩𝙨 𝙩𝙤 𝙥𝙪𝙩 𝙢𝙚 𝙞𝙣 𝙖 𝙥𝙨𝙮𝙘𝙝𝙞𝙖𝙩𝙧𝙞𝙘 𝙝𝙤𝙨𝙥𝙞𝙩𝙖𝙡. 𝘛𝘩𝘦𝘺 𝘱𝘩𝘺𝘴𝘪𝘤𝘢𝘭𝘭𝘺 𝘥𝘦𝘴𝘵𝘳𝘰𝘺𝘦𝘥 𝘮𝘺 𝘭𝘢𝘣𝘰𝘳𝘢𝘵𝘰𝘳𝘺, 𝘸𝘩𝘪𝘤𝘩 𝘸𝘢𝘴 𝘶𝘯𝘪𝘲𝘶𝘦 𝘵𝘩𝘳𝘰𝘶𝘨𝘩𝘰𝘶𝘵 𝘵𝘩𝘦 𝘸𝘰𝘳𝘭𝘥. 𝘈𝘯𝘥 𝘢𝘭𝘭 𝘰𝘧 𝘵𝘩𝘪𝘴 𝘣𝘦𝘤𝘢𝘶𝘴𝘦 𝘐 𝘩𝘢𝘥 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘦𝘥 𝘢 𝘭𝘦𝘷𝘦𝘳 𝘵𝘩𝘢𝘵 𝘱𝘢𝘵𝘪𝘦𝘯𝘵𝘴 𝘤𝘰𝘶𝘭𝘥 𝘱𝘶𝘭𝘭 𝘵𝘰 𝘣𝘦 𝘧𝘳𝘦𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦𝘪𝘳 𝘱𝘪𝘭𝘦𝘴 𝘰𝘧 𝘱𝘪𝘭𝘭𝘴 𝘢𝘯𝘥 𝘤𝘰𝘮𝘱𝘭𝘪𝘤𝘢𝘵𝘦𝘥 𝘴𝘶𝘳𝘨𝘪𝘤𝘢𝘭 𝘱𝘳𝘰𝘤𝘦𝘥𝘶𝘳𝘦𝘴 𝘵𝘩𝘢𝘵 𝘸𝘦𝘳𝘦 𝘧𝘢𝘳 𝘧𝘳𝘰𝘮 𝘴𝘢𝘧𝘦.”
—Konstantin Buteyko, MD, PhD
What happened to Buteyko, while extreme, is not unique. This total shutdown of effective alternative cancer treatments also happened to:
- Wilhelm Reich
- Max Gerson
- Tullio Simoncini
- William F. Koch
Buteyko was diagnosed with malignant hypertension. At age 29, he had a systolic blood pressure of 212 and was experiencing debilitating symptoms. But under great pressure, diamonds are formed—Buteyko found that by decreasing his breathing, his symptoms would disappear. His greatest work would stem from this simple observation.
𝗪𝗵𝗮𝘁 𝗶𝘀 𝗰𝗮𝗿𝗯𝗼𝗻 𝗱𝗶𝗼𝘅𝗶𝗱𝗲’𝘀 𝗿𝗼𝗹𝗲 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿?
The Bohr effect is when carbon dioxide displaces oxygen from hemoglobin, oxygenating the tissue. This understanding of CO2 is downplayed in modern medicine because it seems counterintuitive, but it’s the reason why acetazolamide (a drug given to mountain climbers for mountain sickness) works.
Cancer cells can be characterized by a deficiency of CO2. The tumor-associated enzyme carbonic anhydrase degrades carbon dioxide, and this enzyme has been shown to be over-expressed in many cancer types.[67] This enzyme is induced by hypoxia and implicated in cancer progression.[68]
✺ 𝗧𝗵𝗶𝗮𝗺𝗶𝗻𝗲 𝗶𝘀 𝗮 𝗰𝗮𝗿𝗯𝗼𝗻𝗶𝗰 𝗮𝗻𝗵𝘆𝗱𝗿𝗮𝘀𝗲 𝗶𝗻𝗵𝗶𝗯𝗶𝘁𝗼𝗿 𝘄𝗶𝘁𝗵 𝘀𝗶𝗺𝗶𝗹𝗮𝗿 𝗽𝗼𝘁𝗲𝗻𝗰𝘆 𝘁𝗼 𝗮𝗰𝗲𝘁𝗮𝘇𝗼𝗹𝗮𝗺𝗶𝗱𝗲.[69]
“𝘋𝘳𝘶𝘨𝘴 𝘴𝘪𝘮𝘪𝘭𝘢𝘳 𝘵𝘰 𝘢𝘤𝘦𝘵𝘢𝘻𝘰𝘭𝘢𝘮𝘪𝘥𝘦, 𝘴𝘶𝘭𝘧𝘰𝘯𝘢𝘮𝘪𝘥𝘦𝘴 𝘵𝘩𝘢𝘵 𝘪𝘯𝘩𝘪𝘣𝘪𝘵 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦, 𝘩𝘢𝘷𝘦 𝘳𝘦𝘤𝘦𝘯𝘵𝘭𝘺 𝘣𝘦𝘦𝘯 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘦𝘥 𝘵𝘰 𝘴𝘵𝘰𝘱 𝘵𝘩𝘦 𝘨𝘳𝘰𝘸𝘵𝘩 𝘰𝘧 𝘢 𝘸𝘪𝘥𝘦 𝘷𝘢𝘳𝘪𝘦𝘵𝘺 𝘰𝘧 𝘵𝘶𝘮𝘰𝘳𝘴.”[70][71][72]
—Ray Peat, PhD
“𝘚𝘪𝘯𝘤𝘦 𝘩𝘪𝘴𝘵𝘢𝘮𝘪𝘯𝘦, 𝘴𝘦𝘳𝘰𝘵𝘰𝘯𝘪𝘯,[73] 𝘢𝘯𝘥 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯[74][75] 𝘢𝘳𝘦 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦 𝘢𝘤𝘵𝘪𝘷𝘢𝘵𝘰𝘳𝘴, 𝘵𝘩𝘦𝘪𝘳 𝘢𝘯𝘵𝘢𝘨𝘰𝘯𝘪𝘴𝘵𝘴 𝘸𝘰𝘶𝘭𝘥 𝘩𝘦𝘭𝘱 𝘵𝘰 𝘢𝘤𝘪𝘥𝘪𝘧𝘺 𝘵𝘩𝘦 𝘩𝘺𝘱𝘰𝘹𝘪𝘤 𝘤𝘦𝘭𝘭𝘴. 𝘛𝘦𝘴𝘵𝘰𝘴𝘵𝘦𝘳𝘰𝘯𝘦[76] 𝘢𝘯𝘥 𝘱𝘳𝘰𝘨𝘦𝘴𝘵𝘦𝘳𝘰𝘯𝘦 𝘢𝘳𝘦 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯 𝘢𝘯𝘵𝘢𝘨𝘰𝘯𝘪𝘴𝘵𝘴 𝘵𝘩𝘢𝘵 𝘪𝘯𝘩𝘪𝘣𝘪𝘵 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦.”
—Ray Peat, PhD
✺ 𝗣𝗲𝗮𝘁 𝗲𝗺𝗽𝗵𝗮𝘀𝗶𝘇𝗲𝗱 𝘁𝗵𝗮𝘁 𝗲𝘃𝗲𝗿𝘆𝘁𝗵𝗶𝗻𝗴 𝗶𝗻 𝘁𝗵𝗲 𝗯𝗼𝗱𝘆 𝗯𝗲𝗵𝗮𝘃𝗲𝘀 𝗱𝗶𝗳𝗳𝗲𝗿𝗲𝗻𝘁𝗹𝘆 𝘄𝗵𝗲𝗻 𝗶𝘁’𝘀 𝘄𝗲𝗹𝗹-𝘀𝗮𝘁𝘂𝗿𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝗰𝗮𝗿𝗯𝗼𝗻 𝗱𝗶𝗼𝘅𝗶𝗱𝗲.
“𝘍𝘰𝘳 𝘰𝘷𝘦𝘳 30 𝘺𝘦𝘢𝘳𝘴–𝘧𝘳𝘰𝘮 𝘖𝘤𝘵𝘰𝘣𝘦𝘳 1952 𝘵𝘰 𝘚𝘦𝘱𝘵𝘦𝘮𝘣𝘦𝘳 1985–𝘵𝘩𝘦 𝘮𝘦𝘥𝘪𝘤𝘢𝘭 𝘦𝘴𝘵𝘢𝘣𝘭𝘪𝘴𝘩𝘮𝘦𝘯𝘵 𝘩𝘶𝘴𝘩𝘦𝘥 𝘶𝘱 𝘮𝘺 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘺. 𝘐𝘵 𝘥𝘪𝘥 𝘦𝘷𝘦𝘳𝘺𝘵𝘩𝘪𝘯𝘨 𝘵𝘰 𝘵𝘳𝘢𝘮𝘱𝘭𝘦 𝘰𝘯 𝘢𝘯𝘥 𝘥𝘦𝘴𝘵𝘳𝘰𝘺 𝘵𝘩𝘦 𝘴𝘵𝘳𝘰𝘯𝘨𝘦𝘴𝘵 𝘸𝘦𝘢𝘱𝘰𝘯 𝘪𝘯 𝘵𝘩𝘦 𝘧𝘪𝘨𝘩𝘵 𝘢𝘨𝘢𝘪𝘯𝘴𝘵 𝘮𝘢𝘯𝘺 𝘮𝘰𝘥𝘦𝘳𝘯 𝘥𝘪𝘴𝘦𝘢𝘴𝘦𝘴. 𝙄 𝙬𝙖𝙨 𝙘𝙖𝙡𝙡𝙚𝙙 𝙖 𝙘𝙝𝙖𝙧𝙡𝙖𝙩𝙖𝙣, 𝙖 𝙨𝙘𝙝𝙞𝙯𝙤𝙥𝙝𝙧𝙚𝙣𝙞𝙘 𝙖𝙣𝙙 𝙖 𝙧𝙖𝙫𝙞𝙣𝙜 𝙣𝙪𝙩𝙩𝙚𝙧, 𝙖𝙢𝙤𝙣𝙜 𝙤𝙩𝙝𝙚𝙧 𝙣𝙖𝙢𝙚𝙨. 𝙏𝙝𝙚𝙮 𝙩𝙧𝙞𝙚𝙙 𝙩𝙤 𝙥𝙤𝙞𝙨𝙤𝙣 𝙢𝙚 𝙩𝙝𝙧𝙚𝙚 𝙩𝙞𝙢𝙚𝙨, 𝙖𝙣𝙙 𝙤𝙧𝙜𝙖𝙣𝙞𝙯𝙚𝙙 𝙩𝙬𝙤 𝙘𝙖𝙧 𝙘𝙧𝙖𝙨𝙝𝙚𝙨. 𝙏𝙝𝙚𝙧𝙚 𝙬𝙚𝙧𝙚 𝙨𝙚𝙫𝙚𝙧𝙖𝙡 𝙖𝙩𝙩𝙚𝙢𝙥𝙩𝙨 𝙩𝙤 𝙥𝙪𝙩 𝙢𝙚 𝙞𝙣 𝙖 𝙥𝙨𝙮𝙘𝙝𝙞𝙖𝙩𝙧𝙞𝙘 𝙝𝙤𝙨𝙥𝙞𝙩𝙖𝙡. 𝘛𝘩𝘦𝘺 𝘱𝘩𝘺𝘴𝘪𝘤𝘢𝘭𝘭𝘺 𝘥𝘦𝘴𝘵𝘳𝘰𝘺𝘦𝘥 𝘮𝘺 𝘭𝘢𝘣𝘰𝘳𝘢𝘵𝘰𝘳𝘺, 𝘸𝘩𝘪𝘤𝘩 𝘸𝘢𝘴 𝘶𝘯𝘪𝘲𝘶𝘦 𝘵𝘩𝘳𝘰𝘶𝘨𝘩𝘰𝘶𝘵 𝘵𝘩𝘦 𝘸𝘰𝘳𝘭𝘥. 𝘈𝘯𝘥 𝘢𝘭𝘭 𝘰𝘧 𝘵𝘩𝘪𝘴 𝘣𝘦𝘤𝘢𝘶𝘴𝘦 𝘐 𝘩𝘢𝘥 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘦𝘥 𝘢 𝘭𝘦𝘷𝘦𝘳 𝘵𝘩𝘢𝘵 𝘱𝘢𝘵𝘪𝘦𝘯𝘵𝘴 𝘤𝘰𝘶𝘭𝘥 𝘱𝘶𝘭𝘭 𝘵𝘰 𝘣𝘦 𝘧𝘳𝘦𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦𝘪𝘳 𝘱𝘪𝘭𝘦𝘴 𝘰𝘧 𝘱𝘪𝘭𝘭𝘴 𝘢𝘯𝘥 𝘤𝘰𝘮𝘱𝘭𝘪𝘤𝘢𝘵𝘦𝘥 𝘴𝘶𝘳𝘨𝘪𝘤𝘢𝘭 𝘱𝘳𝘰𝘤𝘦𝘥𝘶𝘳𝘦𝘴 𝘵𝘩𝘢𝘵 𝘸𝘦𝘳𝘦 𝘧𝘢𝘳 𝘧𝘳𝘰𝘮 𝘴𝘢𝘧𝘦.”
—Konstantin Buteyko, MD, PhD
What happened to Buteyko, while extreme, is not unique. This total shutdown of effective alternative cancer treatments also happened to:
- Wilhelm Reich
- Max Gerson
- Tullio Simoncini
- William F. Koch
Buteyko was diagnosed with malignant hypertension. At age 29, he had a systolic blood pressure of 212 and was experiencing debilitating symptoms. But under great pressure, diamonds are formed—Buteyko found that by decreasing his breathing, his symptoms would disappear. His greatest work would stem from this simple observation.
𝗪𝗵𝗮𝘁 𝗶𝘀 𝗰𝗮𝗿𝗯𝗼𝗻 𝗱𝗶𝗼𝘅𝗶𝗱𝗲’𝘀 𝗿𝗼𝗹𝗲 𝗶𝗻 𝗰𝗮𝗻𝗰𝗲𝗿?
The Bohr effect is when carbon dioxide displaces oxygen from hemoglobin, oxygenating the tissue. This understanding of CO2 is downplayed in modern medicine because it seems counterintuitive, but it’s the reason why acetazolamide (a drug given to mountain climbers for mountain sickness) works.
Cancer cells can be characterized by a deficiency of CO2. The tumor-associated enzyme carbonic anhydrase degrades carbon dioxide, and this enzyme has been shown to be over-expressed in many cancer types.[67] This enzyme is induced by hypoxia and implicated in cancer progression.[68]
✺ 𝗧𝗵𝗶𝗮𝗺𝗶𝗻𝗲 𝗶𝘀 𝗮 𝗰𝗮𝗿𝗯𝗼𝗻𝗶𝗰 𝗮𝗻𝗵𝘆𝗱𝗿𝗮𝘀𝗲 𝗶𝗻𝗵𝗶𝗯𝗶𝘁𝗼𝗿 𝘄𝗶𝘁𝗵 𝘀𝗶𝗺𝗶𝗹𝗮𝗿 𝗽𝗼𝘁𝗲𝗻𝗰𝘆 𝘁𝗼 𝗮𝗰𝗲𝘁𝗮𝘇𝗼𝗹𝗮𝗺𝗶𝗱𝗲.[69]
“𝘋𝘳𝘶𝘨𝘴 𝘴𝘪𝘮𝘪𝘭𝘢𝘳 𝘵𝘰 𝘢𝘤𝘦𝘵𝘢𝘻𝘰𝘭𝘢𝘮𝘪𝘥𝘦, 𝘴𝘶𝘭𝘧𝘰𝘯𝘢𝘮𝘪𝘥𝘦𝘴 𝘵𝘩𝘢𝘵 𝘪𝘯𝘩𝘪𝘣𝘪𝘵 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦, 𝘩𝘢𝘷𝘦 𝘳𝘦𝘤𝘦𝘯𝘵𝘭𝘺 𝘣𝘦𝘦𝘯 𝘥𝘪𝘴𝘤𝘰𝘷𝘦𝘳𝘦𝘥 𝘵𝘰 𝘴𝘵𝘰𝘱 𝘵𝘩𝘦 𝘨𝘳𝘰𝘸𝘵𝘩 𝘰𝘧 𝘢 𝘸𝘪𝘥𝘦 𝘷𝘢𝘳𝘪𝘦𝘵𝘺 𝘰𝘧 𝘵𝘶𝘮𝘰𝘳𝘴.”[70][71][72]
—Ray Peat, PhD
“𝘚𝘪𝘯𝘤𝘦 𝘩𝘪𝘴𝘵𝘢𝘮𝘪𝘯𝘦, 𝘴𝘦𝘳𝘰𝘵𝘰𝘯𝘪𝘯,[73] 𝘢𝘯𝘥 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯[74][75] 𝘢𝘳𝘦 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦 𝘢𝘤𝘵𝘪𝘷𝘢𝘵𝘰𝘳𝘴, 𝘵𝘩𝘦𝘪𝘳 𝘢𝘯𝘵𝘢𝘨𝘰𝘯𝘪𝘴𝘵𝘴 𝘸𝘰𝘶𝘭𝘥 𝘩𝘦𝘭𝘱 𝘵𝘰 𝘢𝘤𝘪𝘥𝘪𝘧𝘺 𝘵𝘩𝘦 𝘩𝘺𝘱𝘰𝘹𝘪𝘤 𝘤𝘦𝘭𝘭𝘴. 𝘛𝘦𝘴𝘵𝘰𝘴𝘵𝘦𝘳𝘰𝘯𝘦[76] 𝘢𝘯𝘥 𝘱𝘳𝘰𝘨𝘦𝘴𝘵𝘦𝘳𝘰𝘯𝘦 𝘢𝘳𝘦 𝘦𝘴𝘵𝘳𝘰𝘨𝘦𝘯 𝘢𝘯𝘵𝘢𝘨𝘰𝘯𝘪𝘴𝘵𝘴 𝘵𝘩𝘢𝘵 𝘪𝘯𝘩𝘪𝘣𝘪𝘵 𝘤𝘢𝘳𝘣𝘰𝘯𝘪𝘤 𝘢𝘯𝘩𝘺𝘥𝘳𝘢𝘴𝘦.”
—Ray Peat, PhD
✺ 𝗣𝗲𝗮𝘁 𝗲𝗺𝗽𝗵𝗮𝘀𝗶𝘇𝗲𝗱 𝘁𝗵𝗮𝘁 𝗲𝘃𝗲𝗿𝘆𝘁𝗵𝗶𝗻𝗴 𝗶𝗻 𝘁𝗵𝗲 𝗯𝗼𝗱𝘆 𝗯𝗲𝗵𝗮𝘃𝗲𝘀 𝗱𝗶𝗳𝗳𝗲𝗿𝗲𝗻𝘁𝗹𝘆 𝘄𝗵𝗲𝗻 𝗶𝘁’𝘀 𝘄𝗲𝗹𝗹-𝘀𝗮𝘁𝘂𝗿𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝗰𝗮𝗿𝗯𝗼𝗻 𝗱𝗶𝗼𝘅𝗶𝗱𝗲.

𝗢𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺; 𝗮𝗹𝗹 𝗽𝗮𝘁𝗵𝘀 𝗰𝗼𝗻𝘃𝗲𝗿𝗴𝗲
While the following physicians and scientists treated cancers in different ways and had slightly differing views on the specifics, what they all had in common was that their treatments involved restoring metabolic function:
• Max Gerson treated his patients with liver extract, thyroid hormone, coffee enemas, and tetracycline antibiotics, which corrected metabolic dysfunction.
• Tullio Simoncini believed cancer was a fungus caused by Candida albicans (which hypothyroid people are uniquely susceptible to) and treated his patients with baking soda, which corrected metabolic dysfunction.
• William F. Koch treated his patients with ethylene dione, which corrected metabolic dysfunction. The FDA claimed ethylene dione did not exist and used this claim as evidence that he was a fraud, but a century later, a chemist synthesized it, proving Koch wasn’t a fraud after all.
• Georgi Dinkov (@haidut) recently regressed human tumor grafted onto immunocompromised mice with vitamins B1/B3/B7 and aspirin, which corrected the metabolic dysfunction.
While the following physicians and scientists treated cancers in different ways and had slightly differing views on the specifics, what they all had in common was that their treatments involved restoring metabolic function:
• Max Gerson treated his patients with liver extract, thyroid hormone, coffee enemas, and tetracycline antibiotics, which corrected metabolic dysfunction.
• Tullio Simoncini believed cancer was a fungus caused by Candida albicans (which hypothyroid people are uniquely susceptible to) and treated his patients with baking soda, which corrected metabolic dysfunction.
• William F. Koch treated his patients with ethylene dione, which corrected metabolic dysfunction. The FDA claimed ethylene dione did not exist and used this claim as evidence that he was a fraud, but a century later, a chemist synthesized it, proving Koch wasn’t a fraud after all.
• Georgi Dinkov (@haidut) recently regressed human tumor grafted onto immunocompromised mice with vitamins B1/B3/B7 and aspirin, which corrected the metabolic dysfunction.

𝗪𝗵𝗮𝘁 𝗰𝗮𝗻 𝗯𝗲 𝗱𝗼𝗻𝗲 𝗮𝗯𝗼𝘂𝘁 𝗰𝗮𝗻𝗰𝗲𝗿?
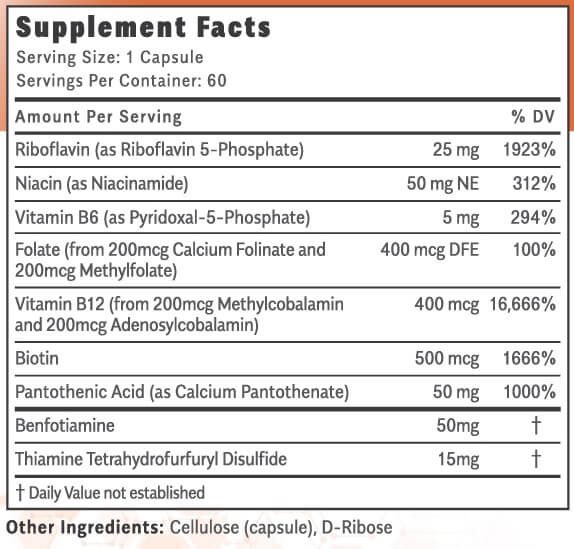
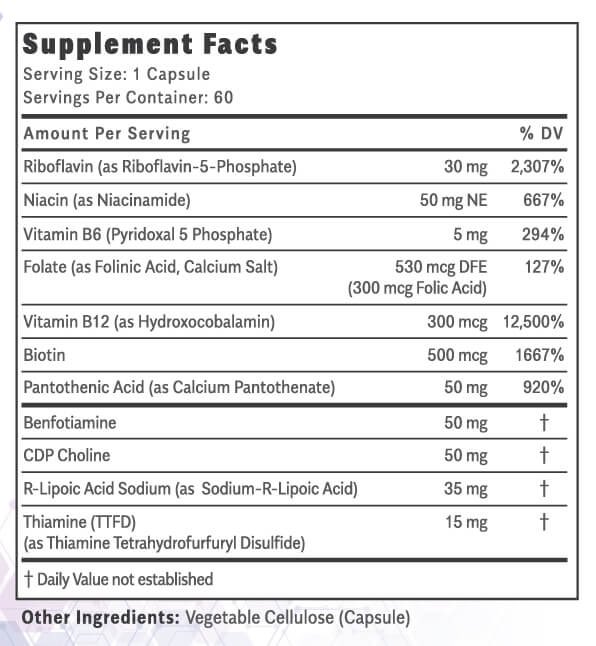
1. 𝗥𝗲𝘀𝘁𝗼𝗿𝗲 𝗼𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺.
• T3
• ATP
• CO2
• Glucose
• Fructose
• Sucrose
• B1
• B2
• B3
• B5
• B6
• B7
• B9
• B12
• Vitamin A
• Vitamin D3
• Vitamin E
• Vitamin K2
• Vitamin C
• CoQ10
• Calcium
• Magnesium
• Potassium
• Sodium
• Coconut oil
• Gelatin
• GABA
• Red light
• Copper
• Selenium
• Zinc
• Caffeine
• Aspirin
• Cholesterol
• Pregnenolone
• Progesterone
• Tetracyclines
• Methylene blue
• Quinine
• Cyproheptadine
2. 𝗠𝗶𝗻𝗶𝗺𝗶𝘇𝗲/𝗼𝗽𝗽𝗼𝘀𝗲 𝘁𝗵𝗲 𝗯𝗶𝗼𝗺𝗮𝗿𝗸𝗲𝗿𝘀 𝗮𝘀𝘀𝗼𝗰𝗶𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝘁𝗵𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺.
• TNF-α
• HIF-α
• IL-4
• IL-6
• IL-8
• NF-κB
• HMGB1
• Endotoxin
• Prostaglandins
• Leukotrienes
• Thromboxanes
• Serotonin
• Lactic acid
• Estrogen
• Histamine
• Nitric oxide
• Ammonia
• Cortisol
• Adrenaline
• Prolactin
Of course, correcting a major metabolic dysfunction can be easier said than done, and everyone’s journey to health is unique. But by staying curious, having hope, and understanding your body, much progress can be made in the right direction.
1. 𝗥𝗲𝘀𝘁𝗼𝗿𝗲 𝗼𝘅𝗶𝗱𝗮𝘁𝗶𝘃𝗲 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺.
• T3
• ATP
• CO2
• Glucose
• Fructose
• Sucrose
• B1
• B2
• B3
• B5
• B6
• B7
• B9
• B12
• Vitamin A
• Vitamin D3
• Vitamin E
• Vitamin K2
• Vitamin C
• CoQ10
• Calcium
• Magnesium
• Potassium
• Sodium
• Coconut oil
• Gelatin
• GABA
• Red light
• Copper
• Selenium
• Zinc
• Caffeine
• Aspirin
• Cholesterol
• Pregnenolone
• Progesterone
• Tetracyclines
• Methylene blue
• Quinine
• Cyproheptadine
2. 𝗠𝗶𝗻𝗶𝗺𝗶𝘇𝗲/𝗼𝗽𝗽𝗼𝘀𝗲 𝘁𝗵𝗲 𝗯𝗶𝗼𝗺𝗮𝗿𝗸𝗲𝗿𝘀 𝗮𝘀𝘀𝗼𝗰𝗶𝗮𝘁𝗲𝗱 𝘄𝗶𝘁𝗵 𝘁𝗵𝗲 𝗰𝗮𝗻𝗰𝗲𝗿 𝗺𝗲𝘁𝗮𝗯𝗼𝗹𝗶𝘀𝗺.
• TNF-α
• HIF-α
• IL-4
• IL-6
• IL-8
• NF-κB
• HMGB1
• Endotoxin
• Prostaglandins
• Leukotrienes
• Thromboxanes
• Serotonin
• Lactic acid
• Estrogen
• Histamine
• Nitric oxide
• Ammonia
• Cortisol
• Adrenaline
• Prolactin
Of course, correcting a major metabolic dysfunction can be easier said than done, and everyone’s journey to health is unique. But by staying curious, having hope, and understanding your body, much progress can be made in the right direction.
𝗖𝗼𝗻𝗰𝗹𝘂𝘀𝗶𝗼𝗻
“𝘞𝘩𝘦𝘯 𝘯𝘦𝘸 𝘬𝘯𝘰𝘸𝘭𝘦𝘥𝘨𝘦 𝘦𝘮𝘦𝘳𝘨𝘦𝘴, 𝘯𝘦𝘸 𝘴𝘤𝘪𝘦𝘯𝘵𝘪𝘧𝘪𝘤 𝘪𝘯𝘴𝘪𝘨𝘩𝘵𝘴, 𝘵𝘩𝘦𝘺 𝘤𝘢𝘯 𝘯𝘦𝘷𝘦𝘳 𝘦𝘷𝘦𝘳 𝘣𝘦 ‘𝘱𝘦𝘦𝘳-𝘳𝘦𝘷𝘪𝘦𝘸𝘦𝘥’. 𝘚𝘰 𝘸𝘦’𝘳𝘦 𝘣𝘭𝘰𝘤𝘬𝘪𝘯𝘨 𝘢𝘭𝘭 𝘯𝘦𝘸 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘴 𝘪𝘯 𝘴𝘤𝘪𝘦𝘯𝘤𝘦 𝘵𝘩𝘢𝘵 𝘢𝘳𝘦 𝘣𝘪𝘨 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘴. 𝘐𝘧 𝘺𝘰𝘶 𝘭𝘰𝘰𝘬 𝘢𝘵 𝘵𝘩𝘦 𝘣𝘳𝘦𝘢𝘬𝘵𝘩𝘳𝘰𝘶𝘨𝘩𝘴 𝘪𝘯 𝘴𝘤𝘪𝘦𝘯𝘤𝘦, 𝘢𝘭𝘮𝘰𝘴𝘵 𝘢𝘭𝘸𝘢𝘺𝘴, 𝘵𝘩𝘦𝘺 𝘥𝘰𝘯’𝘵 𝘤𝘰𝘮𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘤𝘦𝘯𝘵𝘦𝘳 𝘰𝘧 𝘵𝘩𝘢𝘵 𝘱𝘳𝘰𝘧𝘦𝘴𝘴𝘪𝘰𝘯, 𝘵𝘩𝘦𝘺 𝘤𝘰𝘮𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘧𝘳𝘪𝘯𝘨𝘦. 𝘛𝘩𝘦 𝘧𝘪𝘯𝘦𝘴𝘵 𝘤𝘢𝘯𝘥𝘭𝘦𝘮𝘢𝘬𝘦𝘳𝘴 𝘪𝘯 𝘵𝘩𝘦 𝘸𝘰𝘳𝘭𝘥 𝘤𝘰𝘶𝘭𝘥𝘯’𝘵 𝘦𝘷𝘦𝘯 𝘵𝘩𝘪𝘯𝘬 𝘰𝘧 𝘦𝘭𝘦𝘤𝘵𝘳𝘪𝘤 𝘭𝘪𝘨𝘩𝘵𝘴.”
—Allan Savory, Ecologist
I didn’t write this thread because I know everything about cancer; I wrote this thread because the current allopathic model for understanding cancer is flawed since it fails to consider it as primarily a metabolic disorder.
The medical industry is largely ignoring the metabolic origin of cancer. Instead, it is pursuing the more profitable route of producing endless expensive, patented drugs for hyper-specific conditions that fail to treat the vast majority of patients.
𝗪𝗲 𝗰𝗮𝗻’𝘁 𝗺𝗮𝗸𝗲 𝗺𝗲𝗮𝗻𝗶𝗻𝗴𝗳𝘂𝗹 𝗽𝗿𝗼𝗴𝗿𝗲𝘀𝘀 𝗶𝗻 𝘁𝗵𝗲 “𝗪𝗮𝗿 𝗼𝗻 𝗖𝗮𝗻𝗰𝗲𝗿” 𝘂𝗻𝘁𝗶𝗹 𝘄𝗲 𝗮𝗯𝗮𝗻𝗱𝗼𝗻 𝘁𝗵𝗲 𝘄𝗮𝗿, 𝗿𝗲𝗰𝗼𝗴𝗻𝗶𝘇𝗲 𝘁𝗵𝗮𝘁 𝗼𝘂𝗿 𝗼𝘄𝗻 𝗯𝗼𝗱𝘆 𝗶𝘀 𝗻𝗼𝘁 𝗼𝘂𝗿 𝗲𝗻𝗲𝗺𝘆, 𝗮𝗻𝗱 𝗴𝗶𝘃𝗲 𝗶𝘁 𝘁𝗵𝗲 𝘀𝘂𝗽𝗽𝗼𝗿𝘁 𝘁𝗵𝗮𝘁 𝗶𝘁 𝗻𝗲𝗲𝗱𝘀.
This is by no means a definitive thread on cancer. Still, I hope it was useful and provided some resources to take control of your own health and make more informed decisions for yourself and your loved ones.
I am not a doctor and nothing in this thread is medical advice, it is purely informational.
“𝘍𝘰𝘳 𝘦𝘷𝘦𝘳𝘺 𝘵𝘩𝘪𝘯𝘨 𝘵𝘩𝘢𝘵 𝘭𝘪𝘷𝘦𝘴 𝘪𝘴 𝘩𝘰𝘭𝘺, 𝘭𝘪𝘧𝘦 𝘥𝘦𝘭𝘪𝘨𝘩𝘵𝘴 𝘪𝘯 𝘭𝘪𝘧𝘦.”
—William Blake
“𝘞𝘩𝘦𝘯 𝘯𝘦𝘸 𝘬𝘯𝘰𝘸𝘭𝘦𝘥𝘨𝘦 𝘦𝘮𝘦𝘳𝘨𝘦𝘴, 𝘯𝘦𝘸 𝘴𝘤𝘪𝘦𝘯𝘵𝘪𝘧𝘪𝘤 𝘪𝘯𝘴𝘪𝘨𝘩𝘵𝘴, 𝘵𝘩𝘦𝘺 𝘤𝘢𝘯 𝘯𝘦𝘷𝘦𝘳 𝘦𝘷𝘦𝘳 𝘣𝘦 ‘𝘱𝘦𝘦𝘳-𝘳𝘦𝘷𝘪𝘦𝘸𝘦𝘥’. 𝘚𝘰 𝘸𝘦’𝘳𝘦 𝘣𝘭𝘰𝘤𝘬𝘪𝘯𝘨 𝘢𝘭𝘭 𝘯𝘦𝘸 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘴 𝘪𝘯 𝘴𝘤𝘪𝘦𝘯𝘤𝘦 𝘵𝘩𝘢𝘵 𝘢𝘳𝘦 𝘣𝘪𝘨 𝘢𝘥𝘷𝘢𝘯𝘤𝘦𝘴. 𝘐𝘧 𝘺𝘰𝘶 𝘭𝘰𝘰𝘬 𝘢𝘵 𝘵𝘩𝘦 𝘣𝘳𝘦𝘢𝘬𝘵𝘩𝘳𝘰𝘶𝘨𝘩𝘴 𝘪𝘯 𝘴𝘤𝘪𝘦𝘯𝘤𝘦, 𝘢𝘭𝘮𝘰𝘴𝘵 𝘢𝘭𝘸𝘢𝘺𝘴, 𝘵𝘩𝘦𝘺 𝘥𝘰𝘯’𝘵 𝘤𝘰𝘮𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘤𝘦𝘯𝘵𝘦𝘳 𝘰𝘧 𝘵𝘩𝘢𝘵 𝘱𝘳𝘰𝘧𝘦𝘴𝘴𝘪𝘰𝘯, 𝘵𝘩𝘦𝘺 𝘤𝘰𝘮𝘦 𝘧𝘳𝘰𝘮 𝘵𝘩𝘦 𝘧𝘳𝘪𝘯𝘨𝘦. 𝘛𝘩𝘦 𝘧𝘪𝘯𝘦𝘴𝘵 𝘤𝘢𝘯𝘥𝘭𝘦𝘮𝘢𝘬𝘦𝘳𝘴 𝘪𝘯 𝘵𝘩𝘦 𝘸𝘰𝘳𝘭𝘥 𝘤𝘰𝘶𝘭𝘥𝘯’𝘵 𝘦𝘷𝘦𝘯 𝘵𝘩𝘪𝘯𝘬 𝘰𝘧 𝘦𝘭𝘦𝘤𝘵𝘳𝘪𝘤 𝘭𝘪𝘨𝘩𝘵𝘴.”
—Allan Savory, Ecologist
I didn’t write this thread because I know everything about cancer; I wrote this thread because the current allopathic model for understanding cancer is flawed since it fails to consider it as primarily a metabolic disorder.
The medical industry is largely ignoring the metabolic origin of cancer. Instead, it is pursuing the more profitable route of producing endless expensive, patented drugs for hyper-specific conditions that fail to treat the vast majority of patients.
𝗪𝗲 𝗰𝗮𝗻’𝘁 𝗺𝗮𝗸𝗲 𝗺𝗲𝗮𝗻𝗶𝗻𝗴𝗳𝘂𝗹 𝗽𝗿𝗼𝗴𝗿𝗲𝘀𝘀 𝗶𝗻 𝘁𝗵𝗲 “𝗪𝗮𝗿 𝗼𝗻 𝗖𝗮𝗻𝗰𝗲𝗿” 𝘂𝗻𝘁𝗶𝗹 𝘄𝗲 𝗮𝗯𝗮𝗻𝗱𝗼𝗻 𝘁𝗵𝗲 𝘄𝗮𝗿, 𝗿𝗲𝗰𝗼𝗴𝗻𝗶𝘇𝗲 𝘁𝗵𝗮𝘁 𝗼𝘂𝗿 𝗼𝘄𝗻 𝗯𝗼𝗱𝘆 𝗶𝘀 𝗻𝗼𝘁 𝗼𝘂𝗿 𝗲𝗻𝗲𝗺𝘆, 𝗮𝗻𝗱 𝗴𝗶𝘃𝗲 𝗶𝘁 𝘁𝗵𝗲 𝘀𝘂𝗽𝗽𝗼𝗿𝘁 𝘁𝗵𝗮𝘁 𝗶𝘁 𝗻𝗲𝗲𝗱𝘀.
This is by no means a definitive thread on cancer. Still, I hope it was useful and provided some resources to take control of your own health and make more informed decisions for yourself and your loved ones.
I am not a doctor and nothing in this thread is medical advice, it is purely informational.
“𝘍𝘰𝘳 𝘦𝘷𝘦𝘳𝘺 𝘵𝘩𝘪𝘯𝘨 𝘵𝘩𝘢𝘵 𝘭𝘪𝘷𝘦𝘴 𝘪𝘴 𝘩𝘰𝘭𝘺, 𝘭𝘪𝘧𝘦 𝘥𝘦𝘭𝘪𝘨𝘩𝘵𝘴 𝘪𝘯 𝘭𝘪𝘧𝘦.”
—William Blake
𝗦𝗽𝗲𝗰𝗶𝗮𝗹 𝘁𝗵𝗮𝗻𝗸𝘀 𝘁𝗼
@haidut
@dannyroddy
@BradCohn
@ImPeating314
@EndoMedChem
@Outdoctrination
@nobody97799851
@PeatPill
@bioenergy_space
@GenEnergyNotes
@Menatetronone_4
@faustianpeatler
@J0HNSMITHx
@anabology
@haidut
@dannyroddy
@BradCohn
@ImPeating314
@EndoMedChem
@Outdoctrination
@nobody97799851
@PeatPill
@bioenergy_space
@GenEnergyNotes
@Menatetronone_4
@faustianpeatler
@J0HNSMITHx
@anabology
• • •
Missing some Tweet in this thread? You can try to
force a refresh