Prof Adam Finn on Radio 4’s Today programme (@BBCr4today):
“We’re in a very different place with almost everyone in the population immune to SARS-CoV-2...”
This statement is incredibly poor public health messaging. Here’s a quick thread of reasons why…
🧵
“We’re in a very different place with almost everyone in the population immune to SARS-CoV-2...”
This statement is incredibly poor public health messaging. Here’s a quick thread of reasons why…
🧵
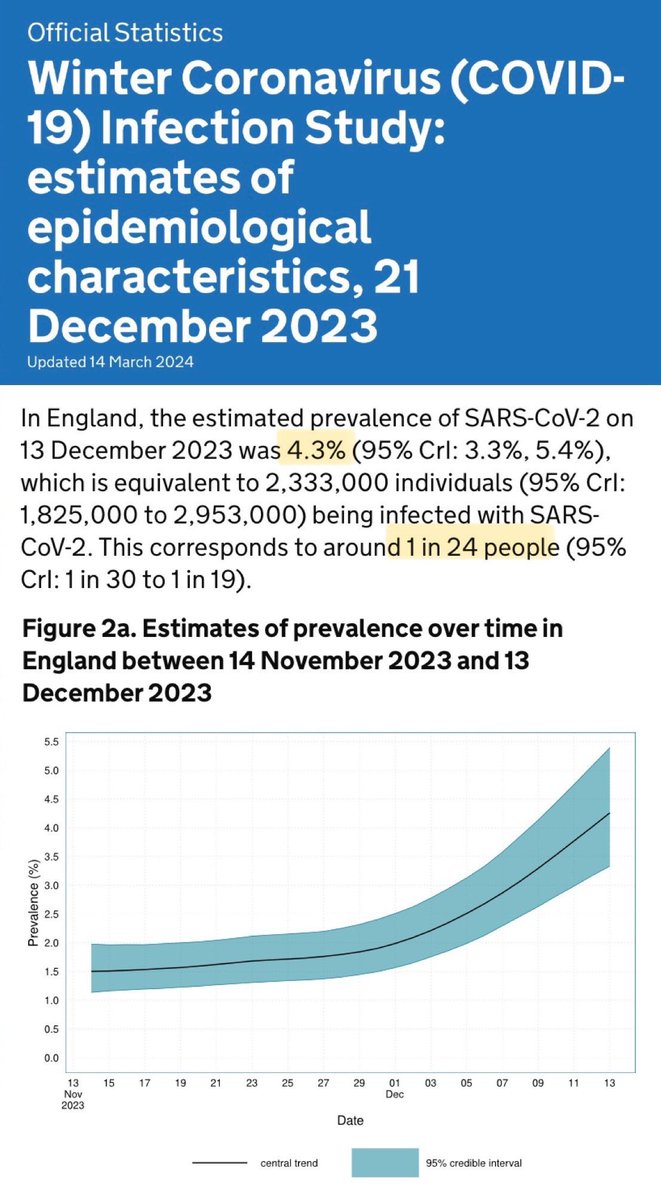
If we’re all so ‘immune’, why is it that, as recently as mid-December 2023, 1 in every 24 people across the whole of England were infected with Covid?
If we’re all so ‘immune’, surely such high waves of Covid shouldn’t be happening repeatedly?
gov.uk/government/sta…

If we’re all so ‘immune’, surely such high waves of Covid shouldn’t be happening repeatedly?
gov.uk/government/sta…
If we’re all so ‘immune’, why do the scientific studies show that people infected with the Omicron variant (& its many sub-variants) have very little natural immunity boost against future Covid infections?
imperial.ac.uk/news/237315/om…
imperial.ac.uk/news/237315/om…

If we’re all so ‘immune’, why does very recent research on the currently circulating JN.1 Covid variant show that protection against reinfection rapidly declines to just 50% after 6-9 months & is down to negligible levels after one year?
(H/t @ejustin46) medrxiv.org/content/10.110…
(H/t @ejustin46) medrxiv.org/content/10.110…

If we’re all so ‘immune’, why have there been nearly 4.5 THOUSAND registered Covid deaths just in the first 17 weeks of 2024?
https://twitter.com/tigresseleanor/status/1788490760846782954

If we’re all so ‘immune’, why is Yale School of Public Health telling us that growing research shows that Covid infections can have a lasting detrimental effect on people’s immune systems, making them more susceptible to other opportunistic infections?
https://twitter.com/_catinthehat/status/1782209760630096168

The really concerning thing is that Prof Adam Finn is a key member of the JCVI, the committee which decides who does and doesn’t get offered a Covid vaccine…

Prof Finn has stated in the past (before the Autumn booster):
“There's no real value in investing a lot of time & effort immunising them again.”
He’s made it clear that the UK’s strategy is a ‘get infected to protect against getting infected’ strategy.
bbc.co.uk/news/health-66…
“There's no real value in investing a lot of time & effort immunising them again.”
He’s made it clear that the UK’s strategy is a ‘get infected to protect against getting infected’ strategy.
bbc.co.uk/news/health-66…

Let me translate:
The stated aim is to get infected over & over & over again… to protect against getting infected over & over & over again!
How does this make any sense at all when there are vaccines available?
The stated aim is to get infected over & over & over again… to protect against getting infected over & over & over again!
How does this make any sense at all when there are vaccines available?
It also seems to be a direct contradiction of what Prof Chris Whitty said recently (in November 2023) at the Covid Inquiry:
“The ONE situation… that you would ever aim to achieve herd immunity is BY VACCINATION. That is the ONLY situation that is a rational policy response.”
“The ONE situation… that you would ever aim to achieve herd immunity is BY VACCINATION. That is the ONLY situation that is a rational policy response.”
Worse still, it turns out that the government would rather throw away the vaccines they’ve ALREADY BOUGHT (with taxpayers money), rather than using them to protect people…
…and so millions of doses have tragically been destroyed.
You can read more about that in this thread ⬇️
…and so millions of doses have tragically been destroyed.
You can read more about that in this thread ⬇️
https://twitter.com/_catinthehat/status/1725575757647200639
For the Spring 2024 booster campaign, the *same* cost-effectiveness methodology was used, with the same fundamental flaws.
Aspects ignored in analysis include:
▪️Long Covid in non-hospitalised patients
▪️Primary care costs
▪️Infection control in hospitals
▪️Workplace absences
Aspects ignored in analysis include:
▪️Long Covid in non-hospitalised patients
▪️Primary care costs
▪️Infection control in hospitals
▪️Workplace absences
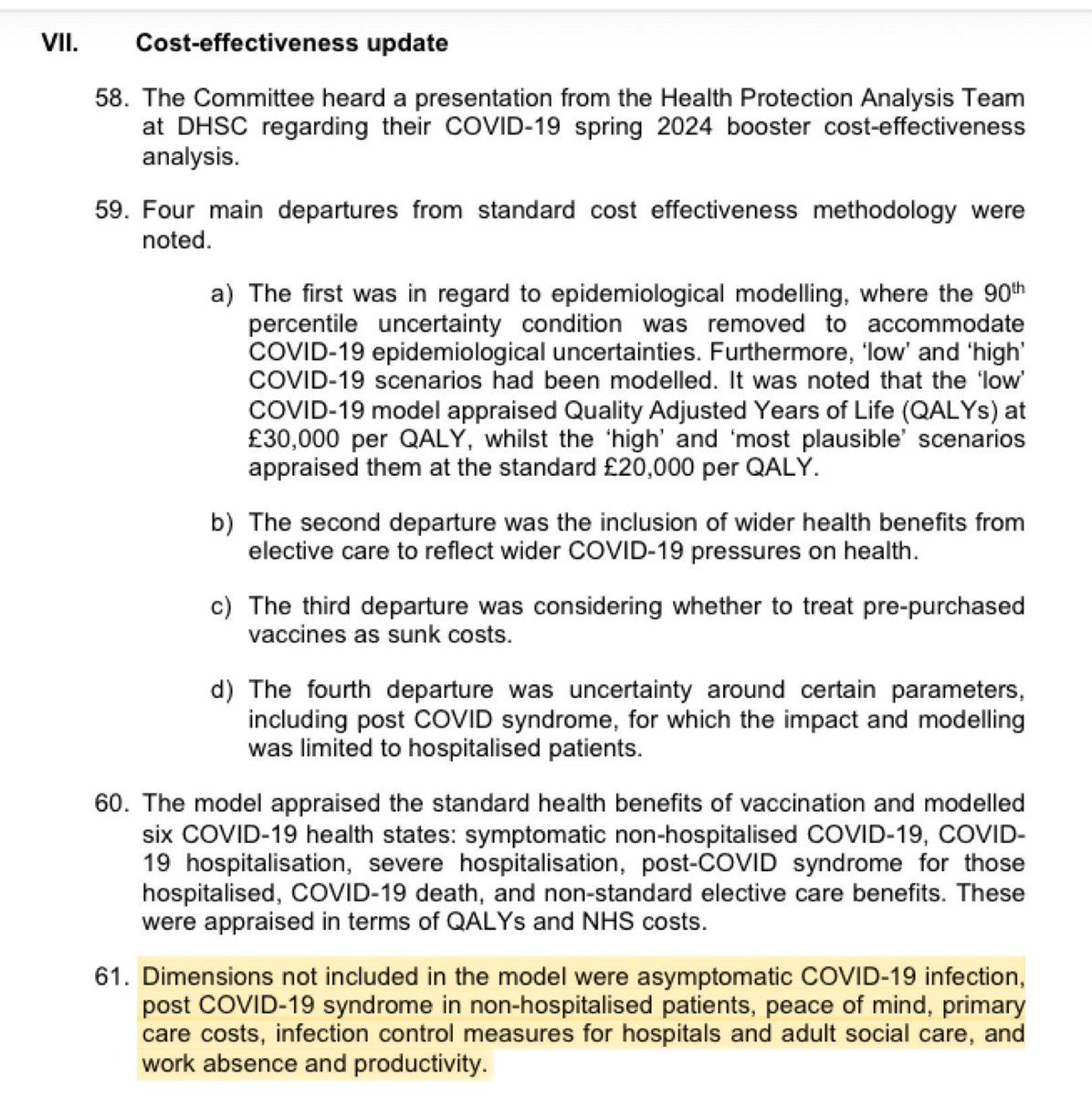
One of the key aspects that has been left out of the cost-effectiveness analysis is the impact of Long Covid in NON-hospitalised patients…
…despite studies which tell us that Long Covid strikes after MILD initial symptoms in ~90% of cases.
fortune.com/2023/01/05/ori…
…despite studies which tell us that Long Covid strikes after MILD initial symptoms in ~90% of cases.
fortune.com/2023/01/05/ori…

We also know that Covid vaccination dramatically lowers the risk of Long Covid.
“A meta-analysis of 24 studies found that people who had received 3 doses of Covid vax were 68.7% less likely to develop Long Covid compared with those who were unvaxxed.”
scientificamerican.com/article/vaccin…
“A meta-analysis of 24 studies found that people who had received 3 doses of Covid vax were 68.7% less likely to develop Long Covid compared with those who were unvaxxed.”
scientificamerican.com/article/vaccin…

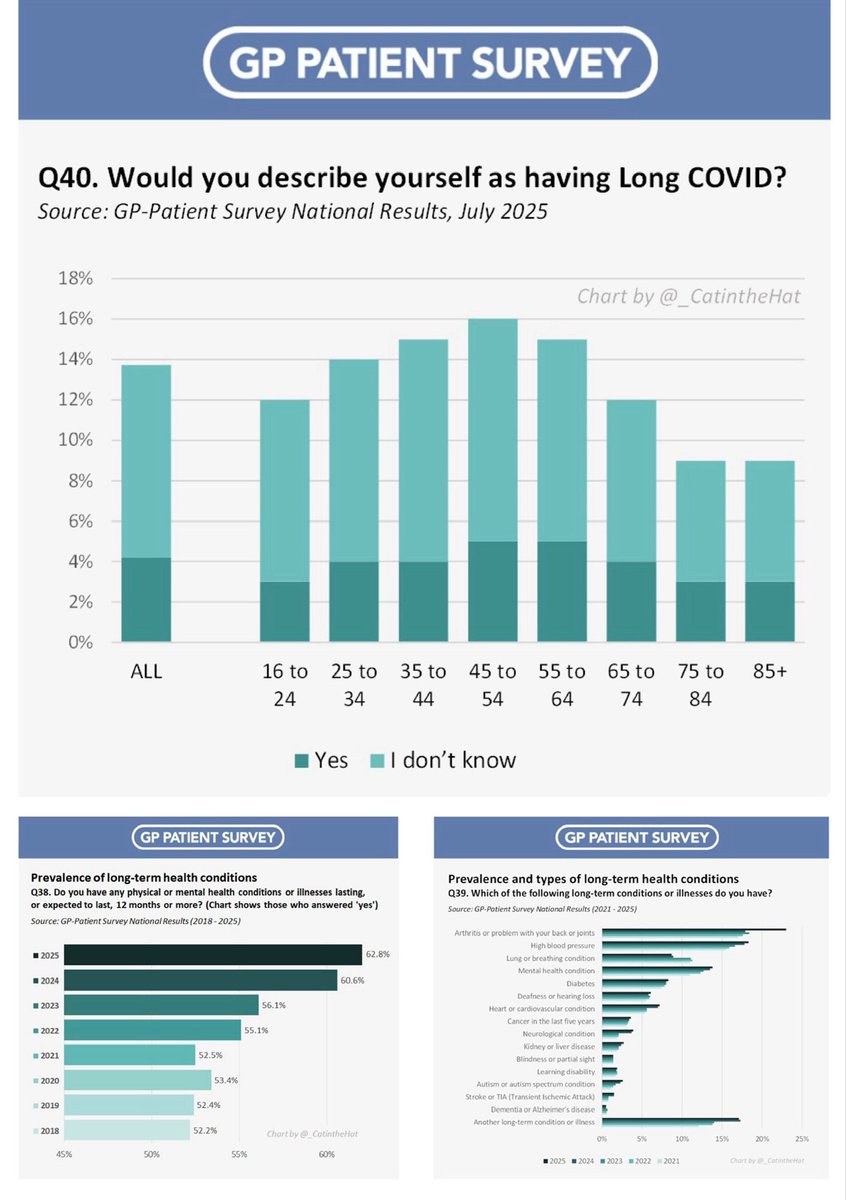
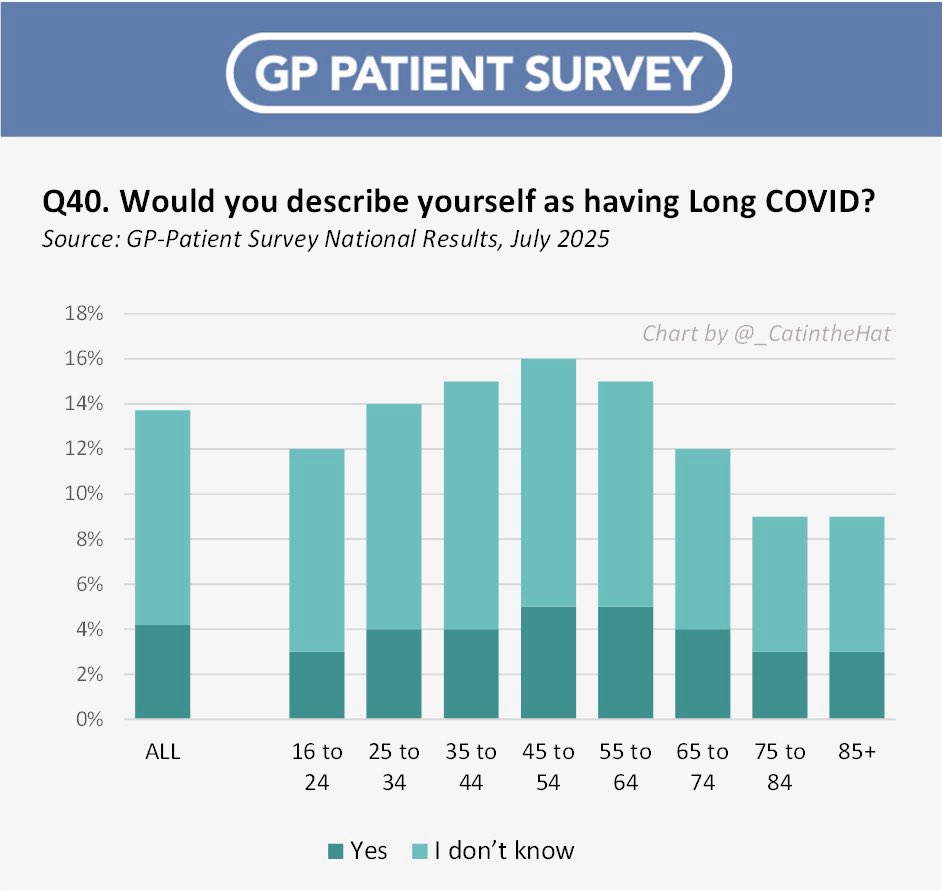
Meanwhile, 2 MILLION people are now suffering from Long Covid across England & Scotland.
That’s a massive 3.3% of the entire population.
Over 380,000 people reported that their daily activities were SEVERELY impacted by their Long Covid illness.
ons.gov.uk/peoplepopulati…
That’s a massive 3.3% of the entire population.
Over 380,000 people reported that their daily activities were SEVERELY impacted by their Long Covid illness.
ons.gov.uk/peoplepopulati…

30% of these people currently affected by Long Covid have been suffering for under a year.
It’s clear that this is NOT just a legacy problem from the early waves of the pandemic.
With each new wave of Covid infections, more & more people are succumbing to Long Covid…
It’s clear that this is NOT just a legacy problem from the early waves of the pandemic.
With each new wave of Covid infections, more & more people are succumbing to Long Covid…

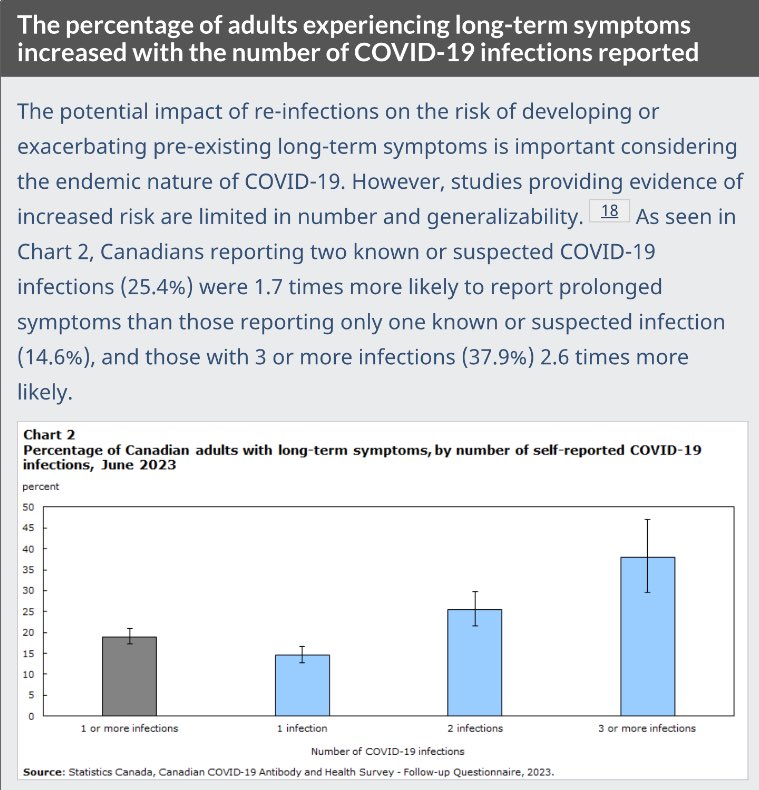
Multiple studies show that the risk of Long Covid increases with each subsequent infection.
This study from @StatCan_eng showed that the risk of developing Long Covid is:
▪️15% after 1 infection
▪️25% after 2 infections
▪️38% after 3+ infections - that’s 1 in 2.6 people!
This study from @StatCan_eng showed that the risk of developing Long Covid is:
▪️15% after 1 infection
▪️25% after 2 infections
▪️38% after 3+ infections - that’s 1 in 2.6 people!
https://twitter.com/chiefscican/status/1733865086748414173
And this study from Prof. Al-Aly (@zalaly) also clearly demonstrated that the risk of developing Long Covid symptoms increases with each successive reinfection.
Just because you’ve had Covid before & were fine, it doesn’t mean you’ll be fine next time…
nature.com/articles/s4159…
Just because you’ve had Covid before & were fine, it doesn’t mean you’ll be fine next time…
nature.com/articles/s4159…

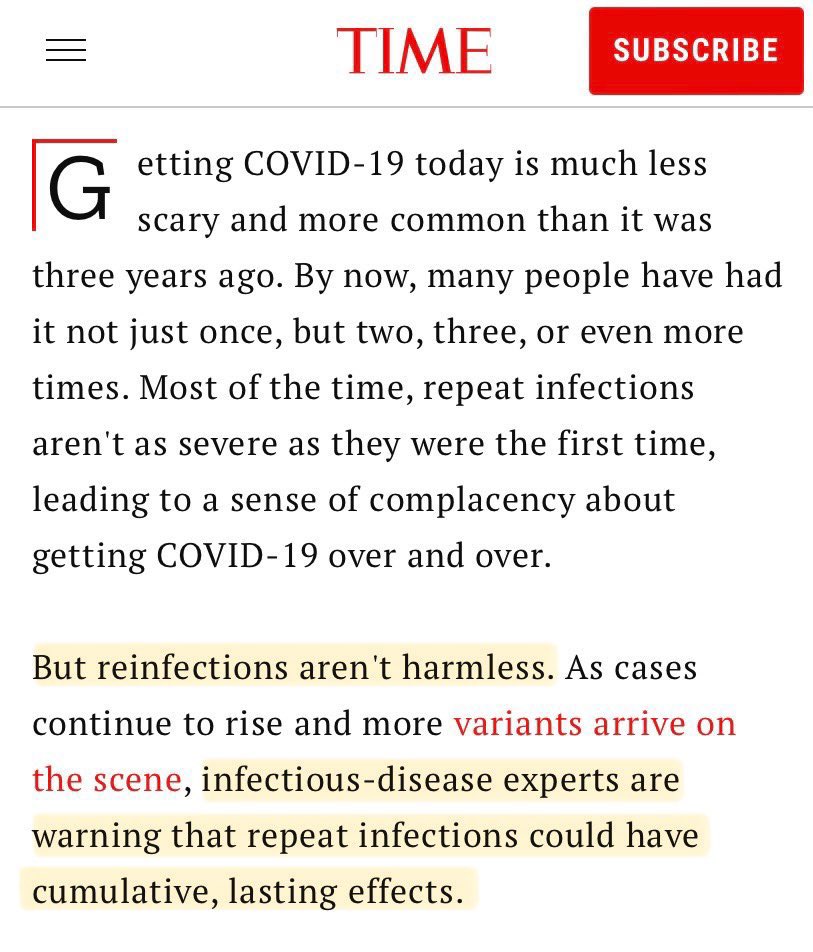
With no mitigations to reduce the spread of Covid, we keep getting infected again & again.
But reinfections are NOT harmless.
Each infection is a game of Covid Roulette as to whether you’ll end up with long-term health repercussions.
time.com/6553340/covid-…
But reinfections are NOT harmless.
Each infection is a game of Covid Roulette as to whether you’ll end up with long-term health repercussions.
time.com/6553340/covid-…
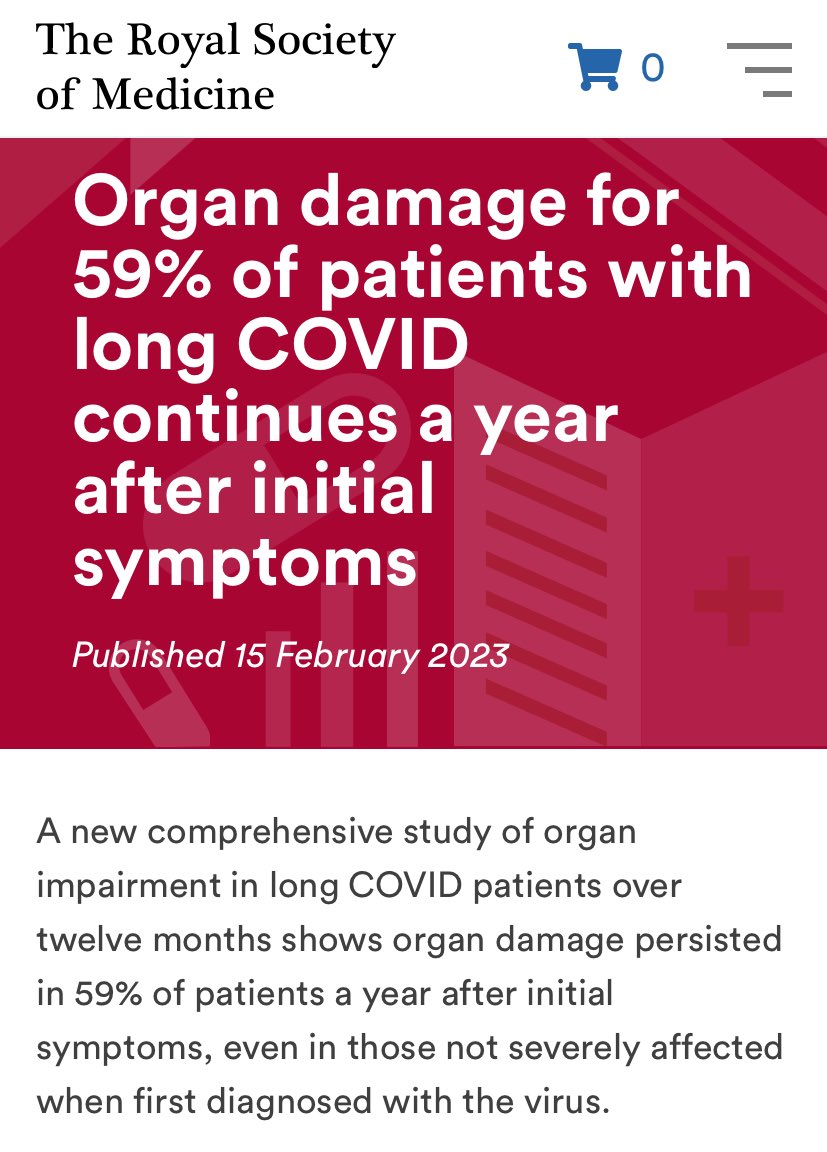
Many people may think they’ve fully recovered from their Covid infection…
…but this is a virus which causes untold damage below the surface…
…and the full impact of the longer term ‘silent’ organ damage may not become apparent for several years.
rsm.ac.uk/media-releases…
…but this is a virus which causes untold damage below the surface…
…and the full impact of the longer term ‘silent’ organ damage may not become apparent for several years.
rsm.ac.uk/media-releases…
A recent study found that people who caught Covid were 5x more likely to die from heart disease in the 18 months after infection.
As of June 2023, there had been nearly 100,000 more deaths than usual attributed to heart problems since the pandemic began.
bhf.org.uk/what-we-do/new…
As of June 2023, there had been nearly 100,000 more deaths than usual attributed to heart problems since the pandemic began.
bhf.org.uk/what-we-do/new…

One of the aspects I’m most concerned about is the long-term damage which Covid can cause to the brain.
We now know that Covid infection can lead to a plethora of new neurological symptoms, including confusion, difficulty concentrating, memory problems, depression & anxiety.
We now know that Covid infection can lead to a plethora of new neurological symptoms, including confusion, difficulty concentrating, memory problems, depression & anxiety.
https://twitter.com/_catinthehat/status/1763878368242524370
All this is leading to a BIG problem…
As Prof Danny Altmann (@Daltmann10) wrote in this paper:
“The oncoming burden of long COVID faced by patients, health-care providers, governments and economies is so large as to be unfathomable…”
nature.com/articles/s4157…
As Prof Danny Altmann (@Daltmann10) wrote in this paper:
“The oncoming burden of long COVID faced by patients, health-care providers, governments and economies is so large as to be unfathomable…”
nature.com/articles/s4157…

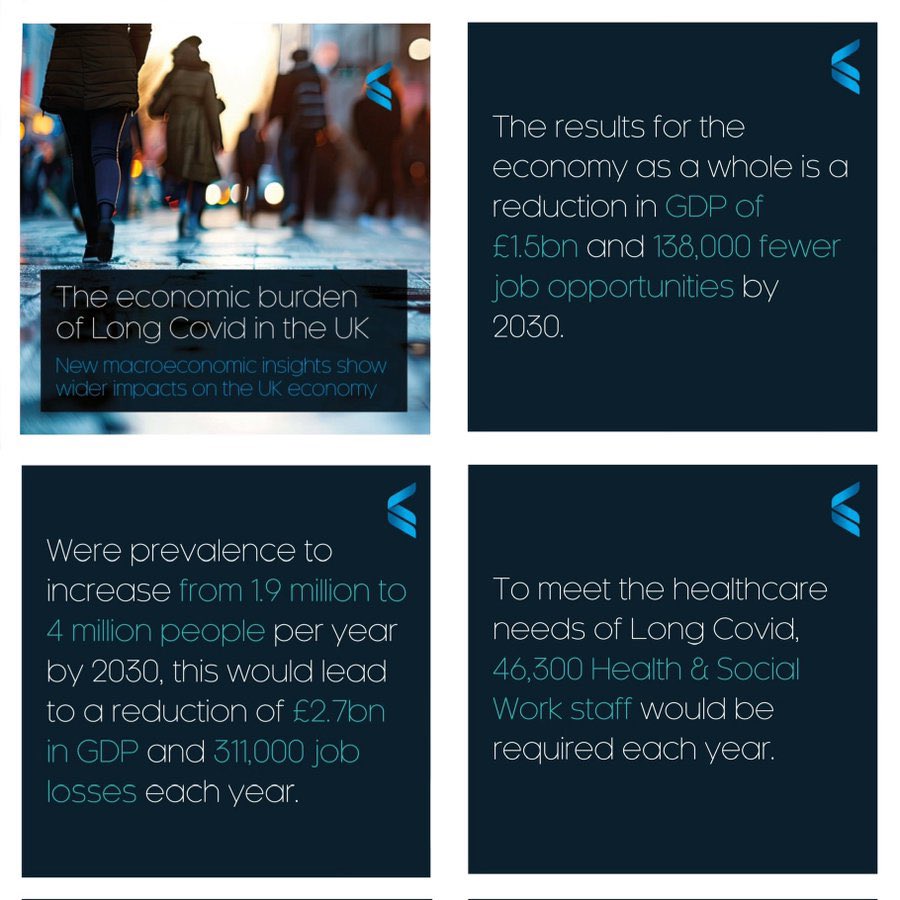
Cambridge Econometrics have done some important analysis into the economic burden of Long Covid in the UK through to 2030…
If prevalence of Long Covid increases to 4 million people by 2030, this would lead to:
▪️a reduction of 2.7 BILLION in GDP
▪️311k job losses PER YEAR.
If prevalence of Long Covid increases to 4 million people by 2030, this would lead to:
▪️a reduction of 2.7 BILLION in GDP
▪️311k job losses PER YEAR.
https://twitter.com/_catinthehat/status/1770429694711656723
To anyone paying attention, none of this should come as a surprise...
When you mass infect a population with a disease which, according to the World Health Organisation, causes long-term chronic illness in around 10% of infections, then this is the inevitable consequence.
When you mass infect a population with a disease which, according to the World Health Organisation, causes long-term chronic illness in around 10% of infections, then this is the inevitable consequence.
https://twitter.com/implausibleblog/status/1651956995010752517
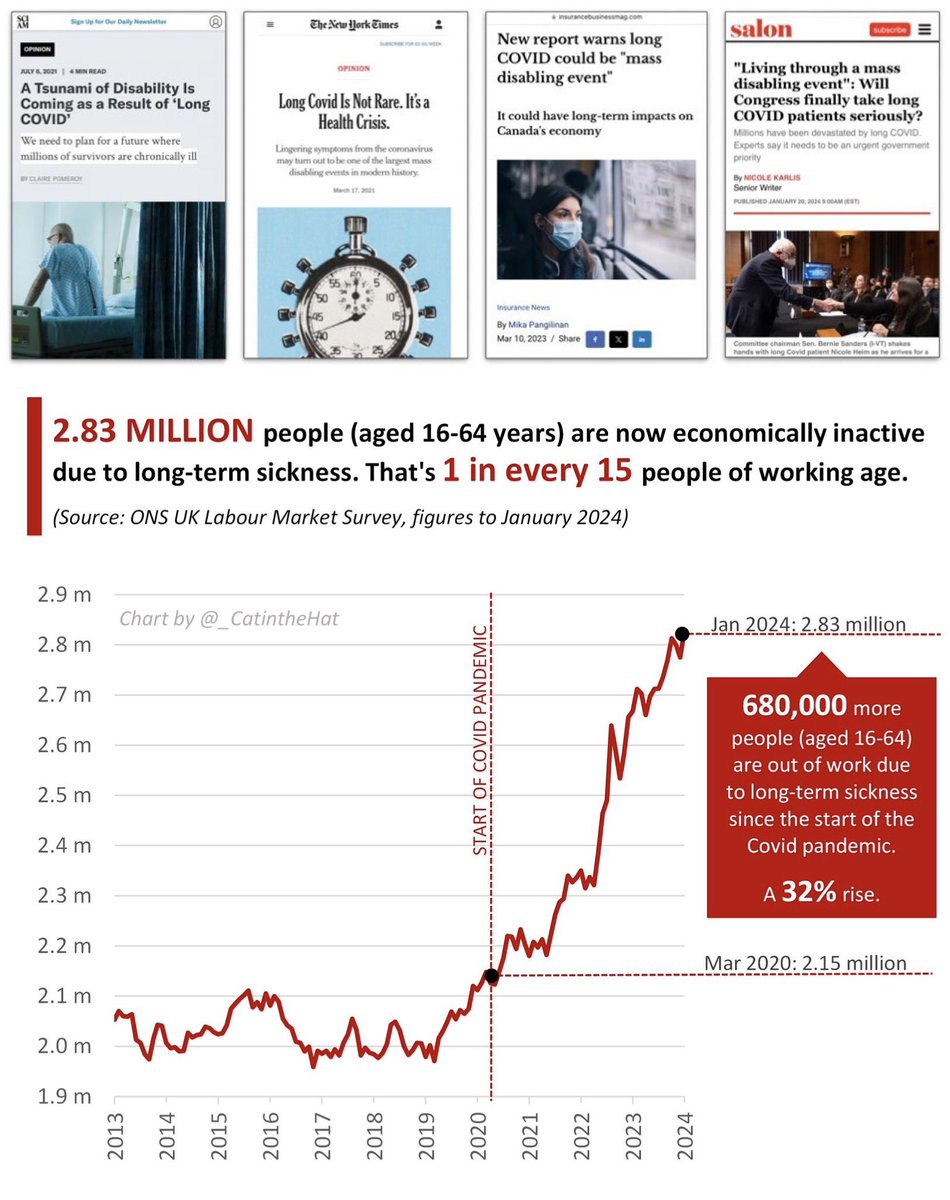
Experts have predicted for several years that Long Covid would lead to a tsunami of disability.
Our government ignored those warnings and now we must all face the consequences...
scientificamerican.com/article/a-tsun…
nytimes.com/2021/03/17/opi…
insurancebusinessmag.com/ca/news/breaki…
salon.com/2024/01/20/liv…
Our government ignored those warnings and now we must all face the consequences...
scientificamerican.com/article/a-tsun…
nytimes.com/2021/03/17/opi…
insurancebusinessmag.com/ca/news/breaki…
salon.com/2024/01/20/liv…
It’s time to stop brushing Covid and Long Covid under the carpet.
It doesn’t have to be this way.
We could be doing SO much more to reduce the spread of infections and halt the gradual decline in the health of our nation & economy.
Here’s my Top 10 Covid mitigation wishlist ⬇️
It doesn’t have to be this way.
We could be doing SO much more to reduce the spread of infections and halt the gradual decline in the health of our nation & economy.
Here’s my Top 10 Covid mitigation wishlist ⬇️
https://twitter.com/_catinthehat/status/1758994858272870822
• • •
Missing some Tweet in this thread? You can try to
force a refresh