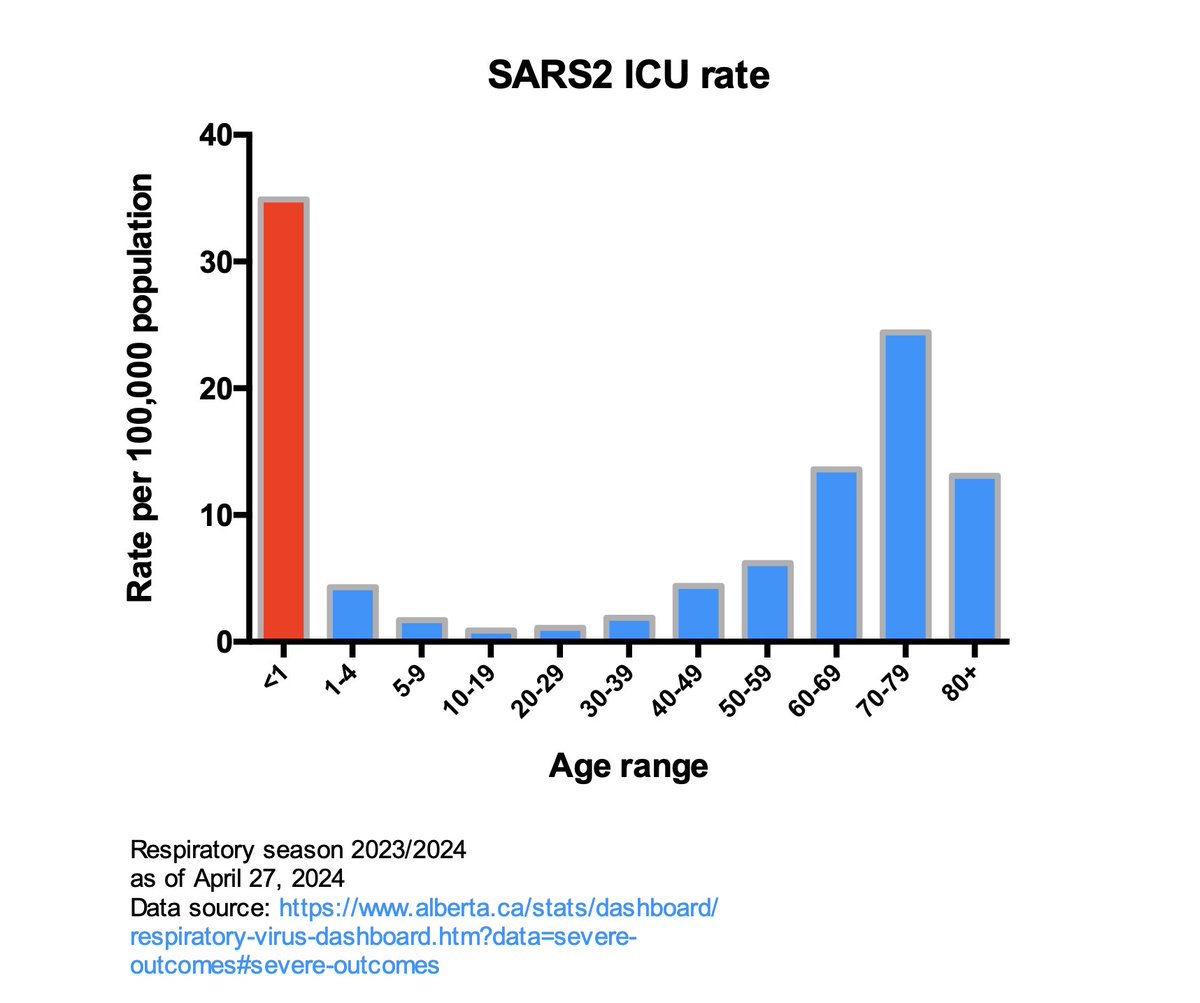
Babies have the highest SARS2 ICU admission rate among all age ranges.
They should be protected from infection by those around them and those around pregnant people & parents.
1/
They should be protected from infection by those around them and those around pregnant people & parents.
1/
Things that'd protect newborns in NICU from infections w/ SARS2, RSV, Influenza
1) Mandatory N95s for staff & visitors (stops short range aerosol transmission)
2) Mandatory testing for RSV/C19/Flu
3) Vaxx requirement C19/Flu & other
4) Medical leadership implementing #1-#3
2/
1) Mandatory N95s for staff & visitors (stops short range aerosol transmission)
2) Mandatory testing for RSV/C19/Flu
3) Vaxx requirement C19/Flu & other
4) Medical leadership implementing #1-#3
2/
Safety of newborns (and their future health) hinges on point #4:
i.e. Medical leadership deciding to prevent irreversible health harms to newborns.
3/
i.e. Medical leadership deciding to prevent irreversible health harms to newborns.
3/
AB, this week. Premies👇
"Although not stated, this is undoubtably the PLC NICU outbreak
So those 2 patients? are premature babies
and I've heard reports that the unit was indeed maskless when the transmission occurred (that's been rectified, for now)"
"Although not stated, this is undoubtably the PLC NICU outbreak
So those 2 patients? are premature babies
and I've heard reports that the unit was indeed maskless when the transmission occurred (that's been rectified, for now)"
https://x.com/jvipondmd/status/1788220184899310053
• • •
Missing some Tweet in this thread? You can try to
force a refresh