Given that the COVID numbers are on the rise, I thought I’d it useful to share some our research team’s work looking at the interplay between CO2, aerosol, SARS-CoV-2, and airborne transmission. 🧵 

SARSCoV2 is spread primarily through the air via aerosol. Meaning, the amount of aerosol a person produces will to some degree correlate with the amount of virus exhaled. Our group has done of studies into how different activities affect aerosol production
tandfonline.com/doi/full/10.10…
tandfonline.com/doi/full/10.10…
The amount of aerosol a person exhales is correlated with how loud they are talking/singing. Perhaps a reason why there have been no super spreader events reported in a library (?)

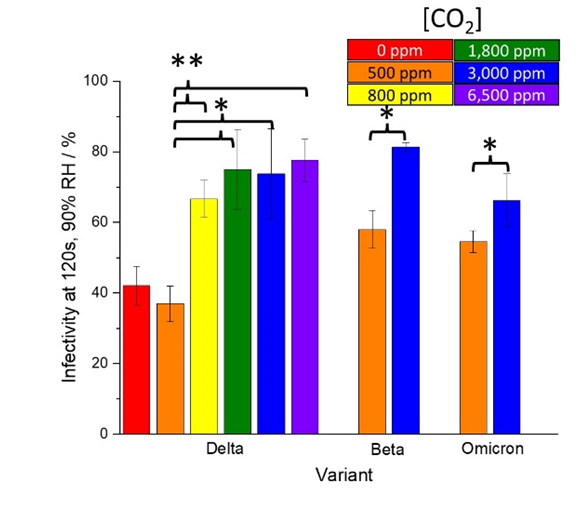
We’ve recently reported that the amount of CO2 in the air will affect how long SARS-CoV-2 remains infectious. Increasing CO2 to as little as 800ppm increases aerostability and transmission risk.
nature.com/articles/s4146…
nature.com/articles/s4146…
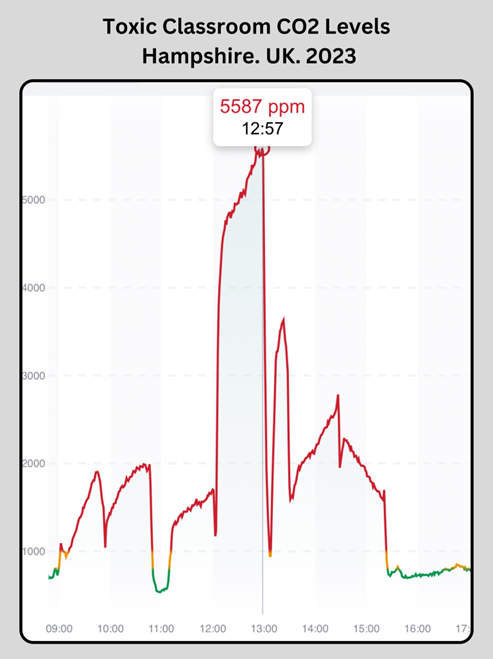
Both CO2 and infectious respiratory aerosol have a similar source, the exhaled breath. As a result, people have used CO2 monitors to measure the amount of CO2 in the air to get a sense of (a) how much exhaled breath is in an area, and (b) roughly how good is the ventilation.
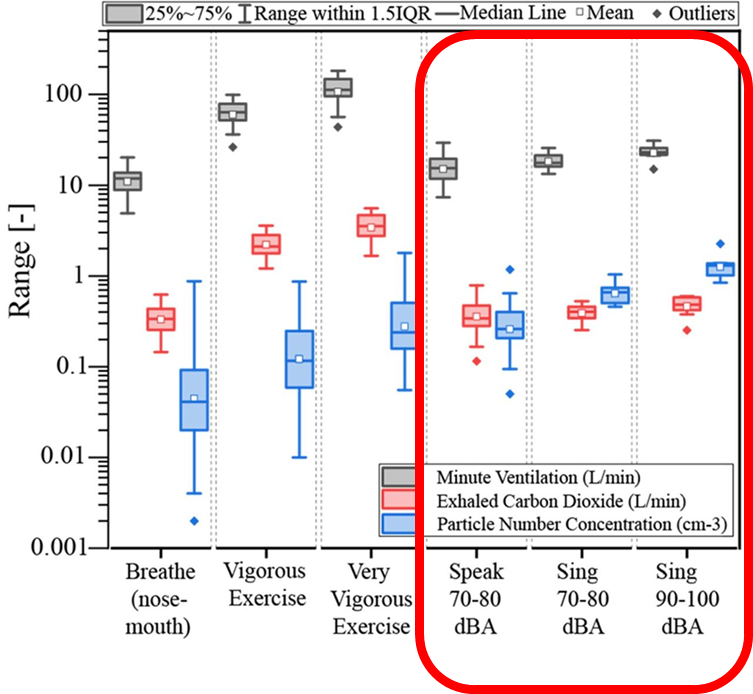
Our group recently reported on the relationship between exhaled aerosol concentration and carbon dioxide across a range of activities.
thorax.bmj.com/content/78/Sup…
thorax.bmj.com/content/78/Sup…
Sometimes the CO2 concentration correlated with the aerosol counts, and sometimes they did not. For example, when a person is silent, the amount of aerosol they produce largely correlates with the CO2 levels exhaled.
Conversely, the volume in which people talks or sings breaks this relationship down. When people are loud, the CO2 level is largely unchanged while the particle counts change dramatically.
So, what does this all mean? Collectively, these studies suggest that there are going to be specific environments where transmission would be much more likely to occur.

For example, in a poorly ventilated space, where the CO2 counts are high, any exhaled virus will remain infectious for much longer. If the people in the space are loud, they will be producing much more aerosol. With this combination, transmission is much more likely.
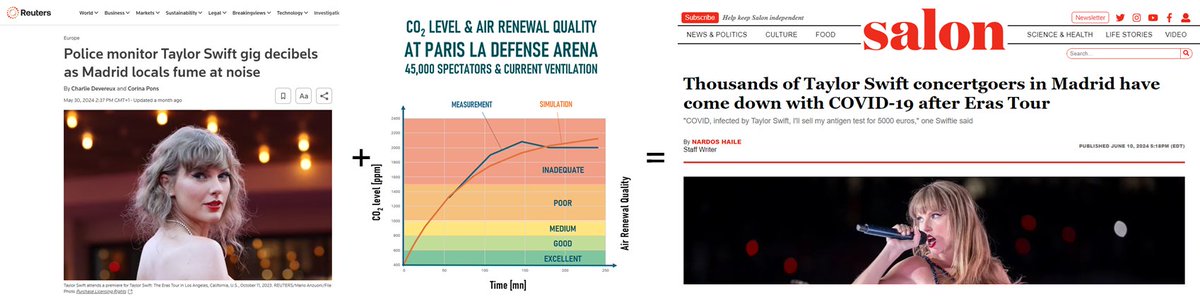
For example, this is not surprising. A stadium filled with people singing is a recipe for trouble.
That said, it’s not all doom and gloom. If you know you are entering an area of higher risk, adjust accordingly. For example, wear a high-quality mask.
That said, it’s not all doom and gloom. If you know you are entering an area of higher risk, adjust accordingly. For example, wear a high-quality mask.
I hope you find this helpful! If you have any questions about any of this, I'd be happy to try to answer them!
@CaliforniaCodes Because CO2 affects both the decay rate and physical removal of the aerosol, the relationship between CO2 and risk is non-linear.
• • •
Missing some Tweet in this thread? You can try to
force a refresh