
OOHHHH WOW! New preprint on the host immune response in Long Covid was just posted (few hours ago), and it's more significant than the 3-gene signature!
They found reactivation of viral herpes (EBV/CMV/HSV2) and CONFIRMED PERSISTENT SARS-CoV-2 INFECTIONS! Here's a summary...
1/![Preprint Title: "MENSA, a Media Enriched with Newly Synthesized Antibodies, to Identify SARS-CoV-2 Persistence and Latent Viral Reactivation in Long-COVID." Abstract: "Here, we use MENSA, Media Enriched with Newly Synthesized Antibodies, secreted exclusively from circulating human plasmablasts, to provide an immune snapshot that defines the underlying viral triggers. [...] Applying the same principles for long-COVID patients, MENSA is positive for SARS2 in 40% of PASC vs none of the COVID recovered (CR) patients without any sequelae demonstrating ongoing SARS2 viral inflamma...](/images/1px.png)
They found reactivation of viral herpes (EBV/CMV/HSV2) and CONFIRMED PERSISTENT SARS-CoV-2 INFECTIONS! Here's a summary...
1/
![Preprint Title: "MENSA, a Media Enriched with Newly Synthesized Antibodies, to Identify SARS-CoV-2 Persistence and Latent Viral Reactivation in Long-COVID." Abstract: "Here, we use MENSA, Media Enriched with Newly Synthesized Antibodies, secreted exclusively from circulating human plasmablasts, to provide an immune snapshot that defines the underlying viral triggers. [...] Applying the same principles for long-COVID patients, MENSA is positive for SARS2 in 40% of PASC vs none of the COVID recovered (CR) patients without any sequelae demonstrating ongoing SARS2 viral inflamma...](https://pbs.twimg.com/media/GR7lGksW8AEcoDF.jpg)
IMO, this is a hugely important study, so I'm going to do my best to explain it in detail, in a way that everybody can understand!
The headline here is that a persistent/reactivated infection of (one or more of) SARS2, EBV, CMV, and/or HSV2 were found in 60% of LC patients!
2/
The headline here is that a persistent/reactivated infection of (one or more of) SARS2, EBV, CMV, and/or HSV2 were found in 60% of LC patients!
2/
Simply put, they looked at the antibodies produced by "Antibody-Secreting Cells" (ASCs), a type of short-lived immune response cells!
The primary types of antibodies stay in the blood. In contrast, ASCs peak *shortly* after infection, then rapidly decline! (see screenshot)
3/
The primary types of antibodies stay in the blood. In contrast, ASCs peak *shortly* after infection, then rapidly decline! (see screenshot)
3/
Because serum (blood) antibodies increase after infection (or vaccination), remaining high for years as a defense against new infection, they're not a good measure of *current* infections!
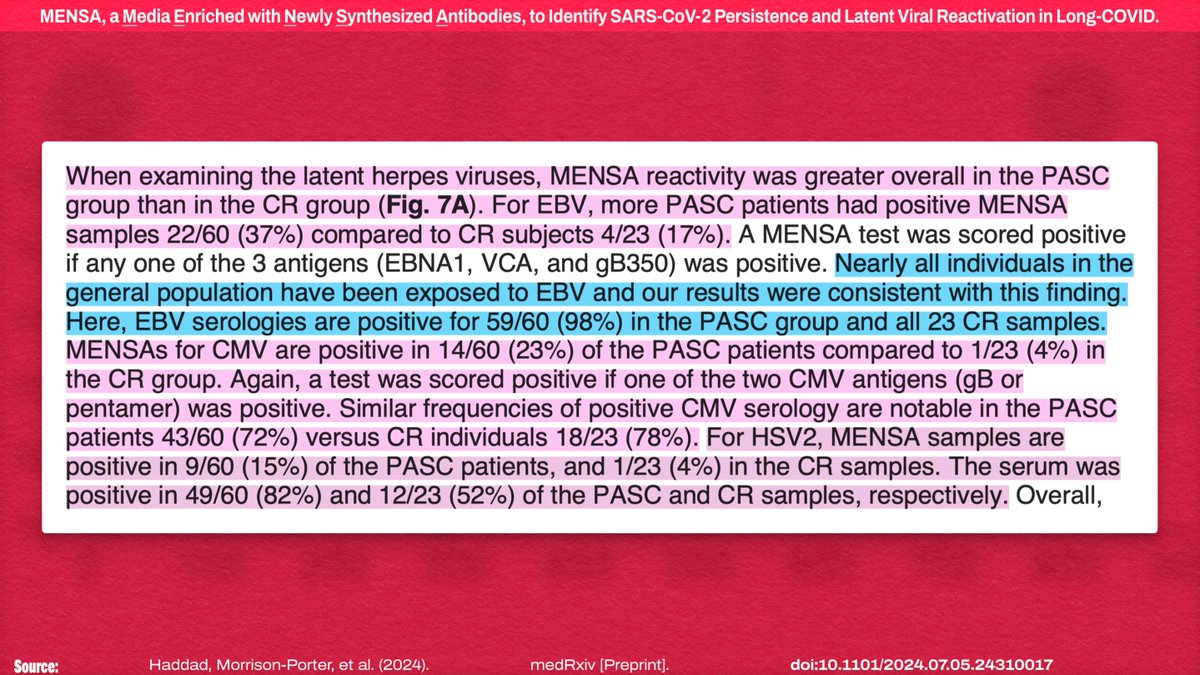
For example, 98% of LC and 100% of controls had serum antibodies for EBV:
4/
For example, 98% of LC and 100% of controls had serum antibodies for EBV:
4/
!["Nearly all individuals in the general population have been exposed to EBV and our results were consistent with this finding. Here, EBV serologies are positive for 59/60 (98%) in the PASC group and all 23 [control] samples."](https://pbs.twimg.com/media/GR7lPztWkAAW0p4.jpg)
This is where the MENSA (Media Enriched with Newly Synthesized Antibodies) matrix created in the current study comes in.
This new tool *specifically* measures the antibodies produced by ASCs (new infections) and memory immune cells (reactivated/persistent infections).
5/20
This new tool *specifically* measures the antibodies produced by ASCs (new infections) and memory immune cells (reactivated/persistent infections).
5/20
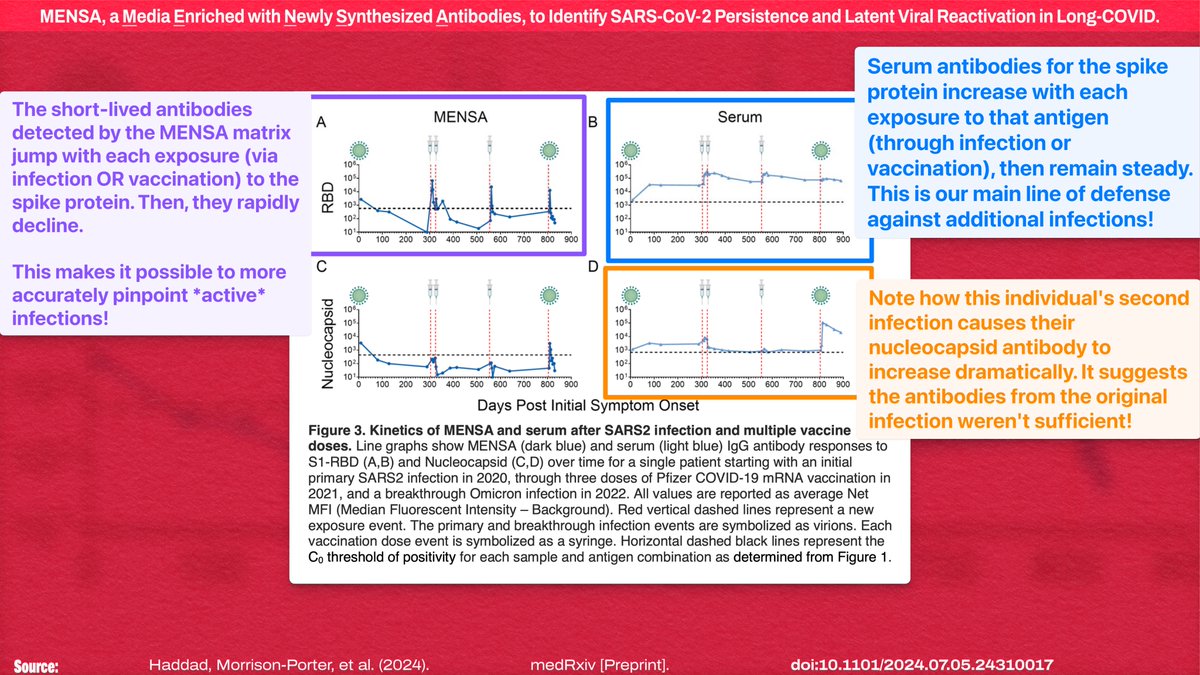
Looking at SARS-CoV-2 antibodies for one individual across multiple infections and vaccinations (comparing serum vs. MENSA antibody levels), the MENSA antibodies decline MUCH more rapidly after each exposure.
Thus, it distinctly detects *active* infection!
6/20
Thus, it distinctly detects *active* infection!
6/20
Just for the uninformed losers who show up to squawk "it's the jab! it's the jab!" every time:
- All of the LC patients had pre-vaccine infections
- 97% of the LC patients had nucleocapsid antibodies in serum. Those are acquired through INFECTION, and aren't in mRNA vaccines
7/
- All of the LC patients had pre-vaccine infections
- 97% of the LC patients had nucleocapsid antibodies in serum. Those are acquired through INFECTION, and aren't in mRNA vaccines
7/
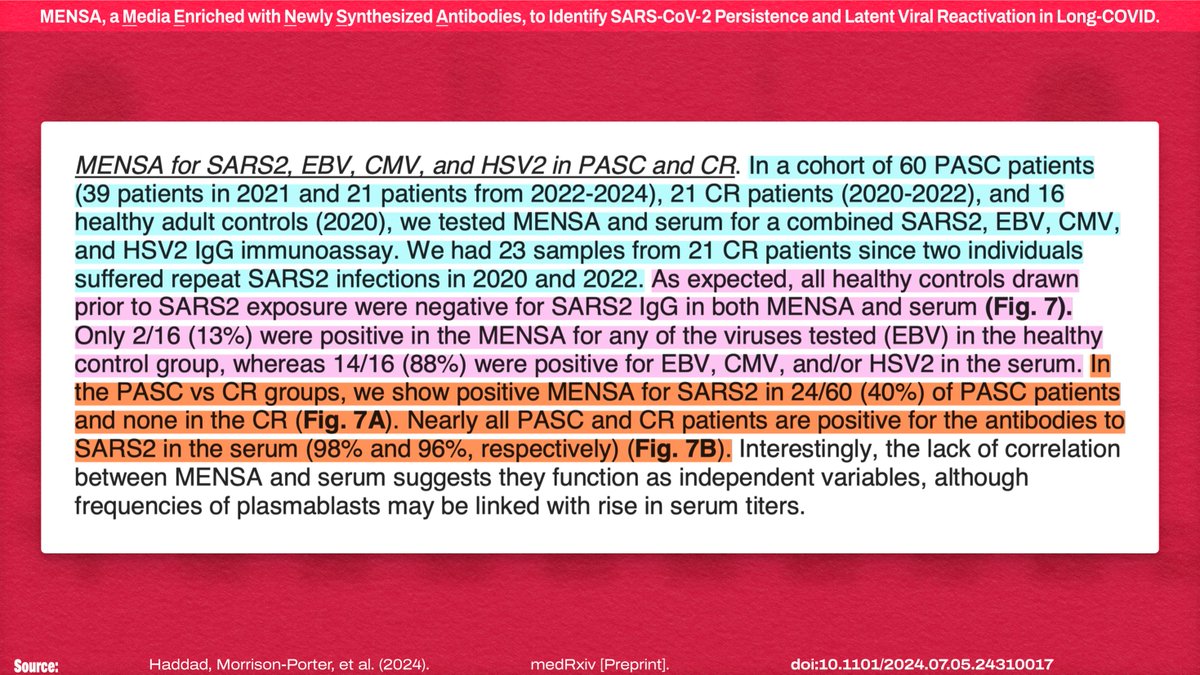
!["For the initial PASC experiment, we tested for only SARS2 antigens in MENSA and serum samples prepared from the subset of 19 CR subjects mentioned above and 39 PASC patients recruited during the first year of the Long-COVID clinic at Emory University December 2020-May 2021. [...] All patients were enrolled from day 60-279 DPSO after their initial acute infection and prior to any COVID-19 vaccination. Of the 39 PASC patients, 56% had initial M/M acute infections and 44% had initial S/C acute infections. Of the 19 CR patients, 95% had M/M acute infections and 5% had S/C acute infections...](https://pbs.twimg.com/media/GR7lZ5UW8AABoDe.jpg)
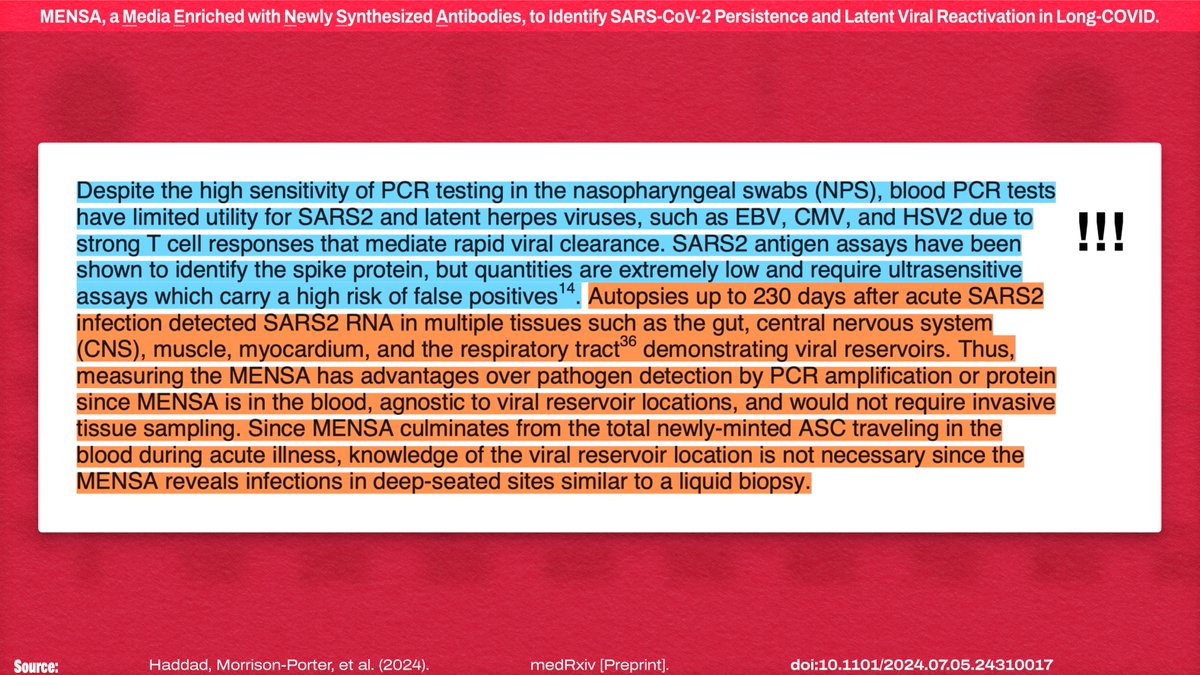
An issue with existing research is that SARS2 (and Herpesviruses) just don't show up in PCR tests of blood. Most of the studies showing viral reservoirs are *autopsy* studies because sampling those tissues is *destructive*
MENSA indirectly samples those same reservoirs!
8/20
MENSA indirectly samples those same reservoirs!
8/20
Antibodies produced by ASCs are only found when there was RECENTLY a replicating pathogen that the immune system needed to attack, so this test can identify the "cause of the present-day illness" and is "an immune snapshot to uncover the sources of the patient's ailment"!
9/20
9/20
!["...lymph nodes to form memory B cells and newly-minted ASC that produce antibodies. Interestingly, the majority of these ASC die, but a few successfully migrate to the bone marrow or tissue sites where they can undergo further maturation to become long-lived plasma cells (LLPC). [...] Memory B cells persist over a lifetime and differentiate into plasmablasts when re-encountering the same antigens?5. During breakthrough or repeat infections, newly-minted ASC mostly originate from memory B cells and circulate transiently in the blood'5. Since MENSA measures antibodies only from these ne...](https://pbs.twimg.com/media/GR7lf7xWQAAmlcC.jpg)
They found reactivated latent infections! Here's the percentage of patients positive for *MENSA antibodies* (CR = Covid Recovered)
- EBV: 37% LC / 17% CR
- CMV: 23% LC / 4% CR
- HSV2: 15% LC / 4% CR
But *serum* levels were high for all, because these viruses are common!
10/20
- EBV: 37% LC / 17% CR
- CMV: 23% LC / 4% CR
- HSV2: 15% LC / 4% CR
But *serum* levels were high for all, because these viruses are common!
10/20
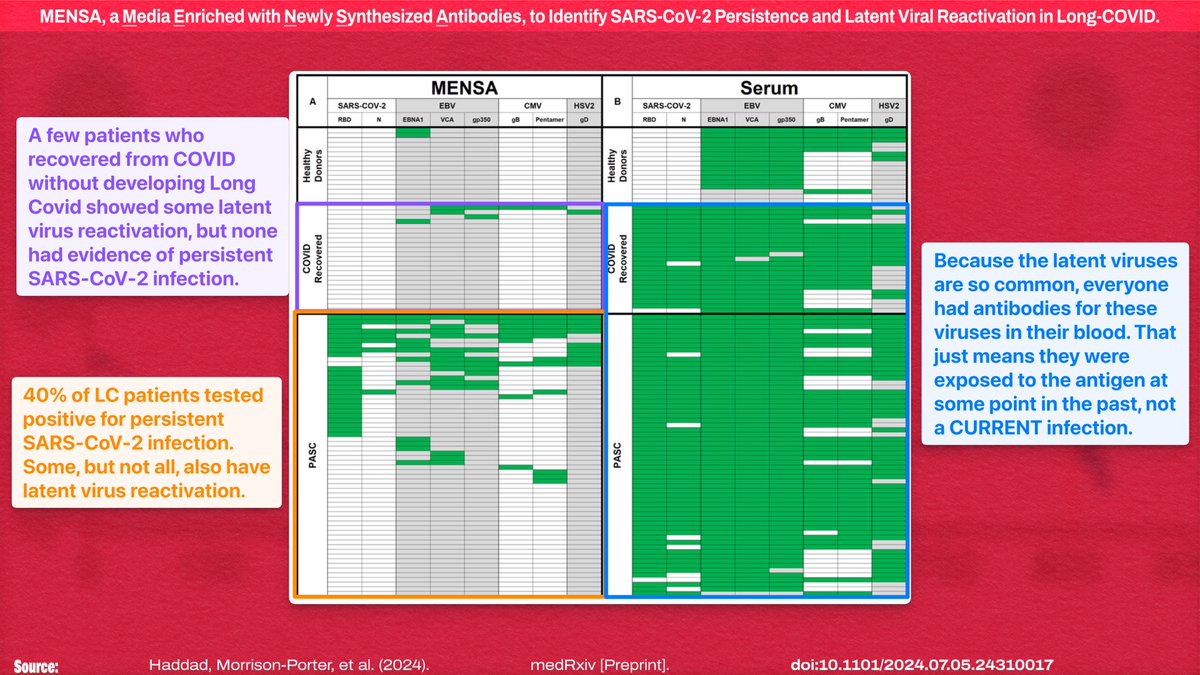
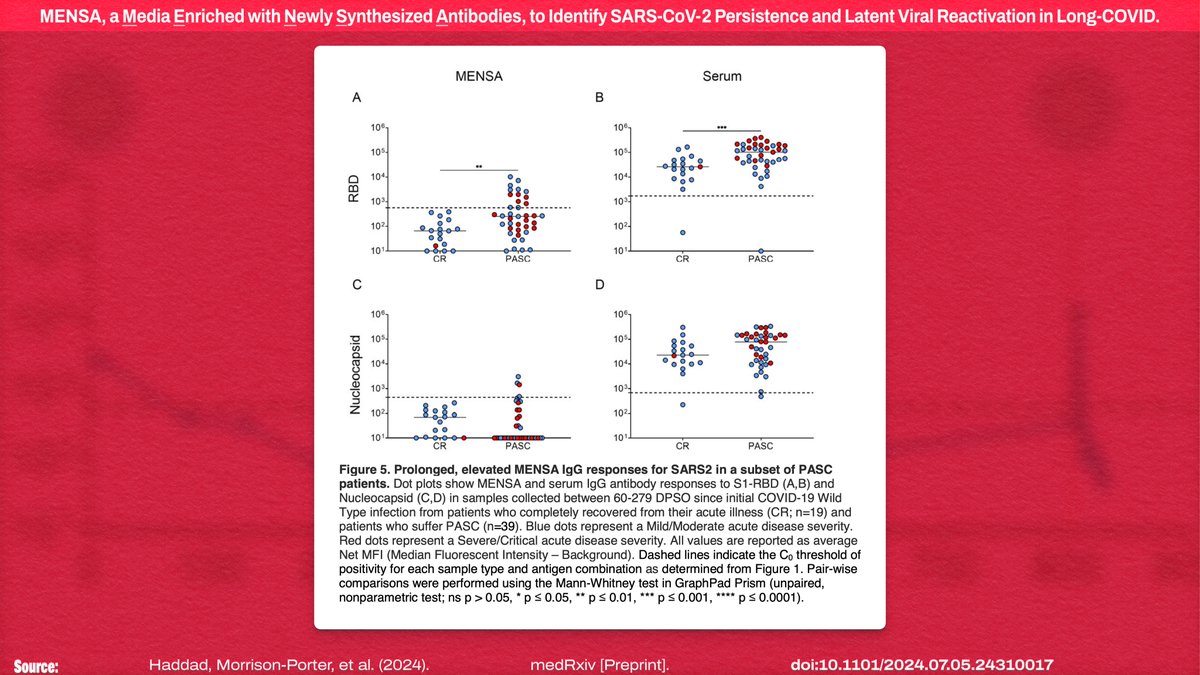
But even more significantly, they found the presence of MENSA antibodies for SARS-CoV-2 (indicating *persistent* infection) in 40% of LC patients and NONE OF THE CONTROL GROUP.
To put it another way, this test has SPECIFCALLY identified persistent SARS-CoV-2 infections!
11/20
To put it another way, this test has SPECIFCALLY identified persistent SARS-CoV-2 infections!
11/20
Overall, the MENSA assays found:
- HALF of the LC patients were positive for at least one of EBV/CMV/HSV2
- 60% of the LC patients were positive for at least one of EBV/CMV/HSV2 *or* SARS2
- Only 17% of the recovered were positive for even one of EBV/CMV/HSV2
12/20
- HALF of the LC patients were positive for at least one of EBV/CMV/HSV2
- 60% of the LC patients were positive for at least one of EBV/CMV/HSV2 *or* SARS2
- Only 17% of the recovered were positive for even one of EBV/CMV/HSV2
12/20
IMO, 40% is the LOWER bound for people with LC having persistent SARS-CoV-2 infection, because their positivity threshold is fairly conservative, statistically speaking: SARS2 positivity is three standard deviations beyond the mean MENSA values for *recovered* patients!
13/20
13/20
The AVERAGE level of antibodies *in the LC group* was BELOW the point they set as the test positivity threshold for the MENSA assay.
If we assume intensity of persistent infection is a spectrum, this is now an optimization problem!
14/20
If we assume intensity of persistent infection is a spectrum, this is now an optimization problem!
14/20
This study pushes us a long way toward understanding the *specific drivers* of Long Covid, given that observable chronic symptoms don't manifest after *every* infection. MENSA allows precise sampling of *currently active* infections, regardless of serum antibody levels!
15/20
15/20
It's also worth noting that they checked for the presence of active responses to autoantigens and came up empty; however, that's not a definitive answer, because their technique had limited power. But, realistically, persistent infection explains most of the symptoms!
16/20
16/20
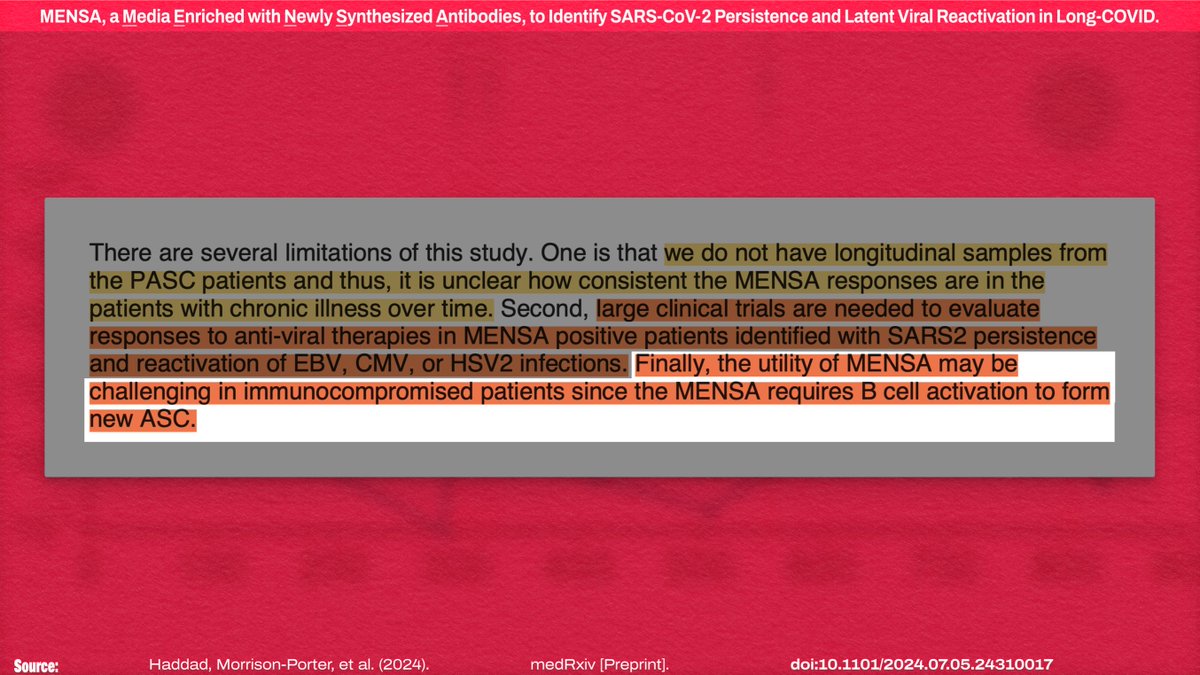
It's unknown how the MENSA assay results will look *over time* in LC patients or how treatment impacts it, so the specifics of how it can be used as a diagnostic tool are up in the air. But that's usually something the lab companies that commercialize the tests figure out!
17/20
17/20
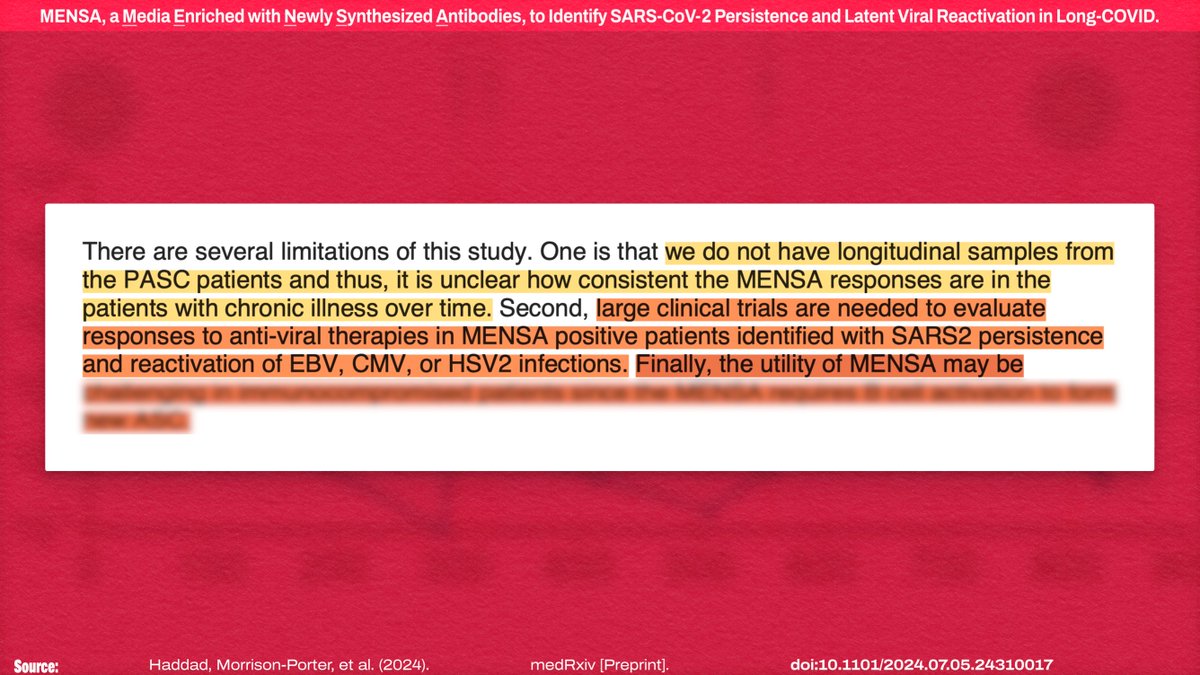
And, of course, that gigantic fucking Catch-22 of the week, the MENSA assay may not be reliable in immunocompromised patients due to lack of B cell activation to form ASCs. SARS-CoV-2 ALSO fucks with B cells, in addition to T cells. Fantastic.
18/20
18/20
https://x.com/NickAnderegg/status/1809763342837256201
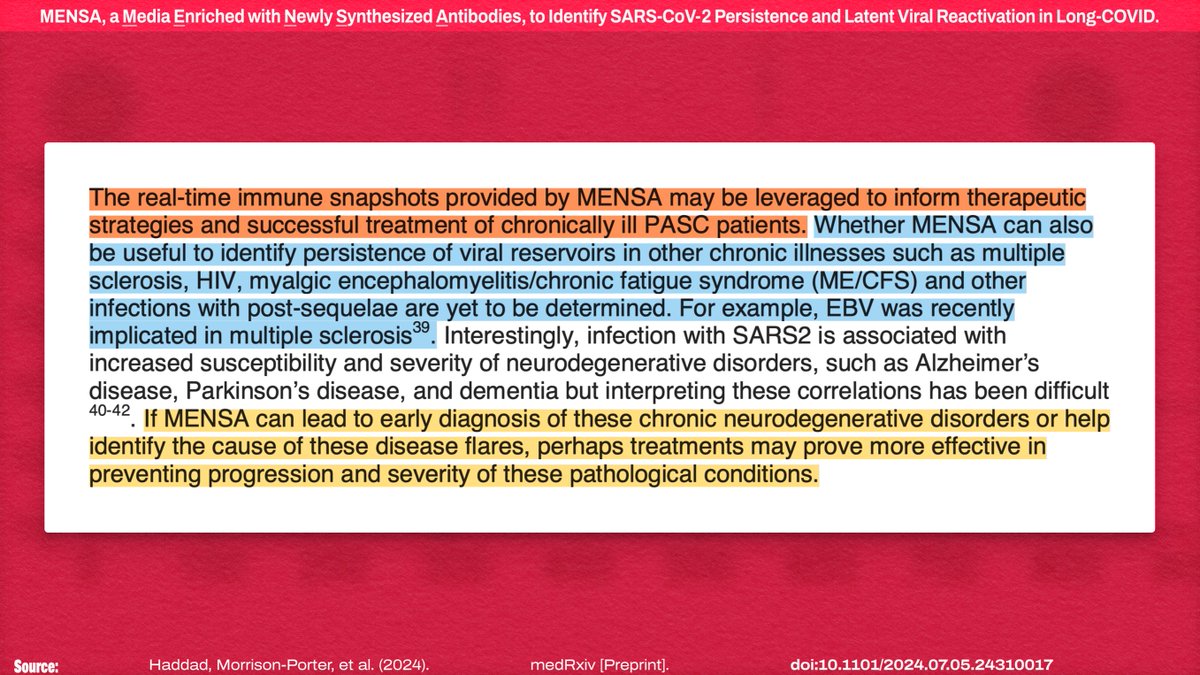
One interesting thing to note is that this method may *potentially* be capable of detecting other chronic (and/or neurodegenerative) conditions from very early in their onset, long before symptoms are present!
19/20
19/20
IMO, this is a STRONG study, and it's a starting point for much more specific diagnostics of chronic conditions resulting from SARS-CoV-2 infection—or any other pathogen!
AND IT CONFIRMS SARS2 VIRAL PERSISTENCE!
Preprint on medRxiv:
20/endmedrxiv.org/content/10.110…
AND IT CONFIRMS SARS2 VIRAL PERSISTENCE!
Preprint on medRxiv:
20/endmedrxiv.org/content/10.110…
This study is really just about the diagnostic tool, and their confirmation of viral persistence were part of proving that the tool works. This will likely end up being part of the measure treatment response, however
21/20
21/20
https://twitter.com/derekmorgan2020/status/1810267805318615375
Also, huge shoutout to the people who routinely quote my threads with translations to other languages! We’ve got an efficient little global public health information network going!
22/20
22/20
IMO they missed a huge opportunity by not including VZV in their panel, because shingles is suuuch a common PASC! If (and only if) LC symptoms turn out to be driven PRIMARILY by latent herpesvirus reactivation (triggered by SARS2 persistence), VZV will prob be another 40%
23/20
23/20
https://twitter.com/justushoneybees/status/1810316847667146764
TBD! This is really just a technical paper introducing a new *test method*, not a full blown virology research/theory paper. Also note that positives in the LC group were
- 40% for SARS2
- 47% for EBV/CMV/HSV2
- *60%* for SARS2 *and/or* EBV/CMV/HSV2
24/20
- 40% for SARS2
- 47% for EBV/CMV/HSV2
- *60%* for SARS2 *and/or* EBV/CMV/HSV2
24/20
https://x.com/Opinions_Survey/status/1810339194020954523
Good question! The *sensitivity* of this provisional test (i.e. not yet commercialized) was set conservatively to ensure the validity of the test results. If SARS2 persistence is ubiquitous, this positivity *threshold* will be artificially high
25/20
25/20
https://x.com/Opinions_Survey/status/1810342345704869958
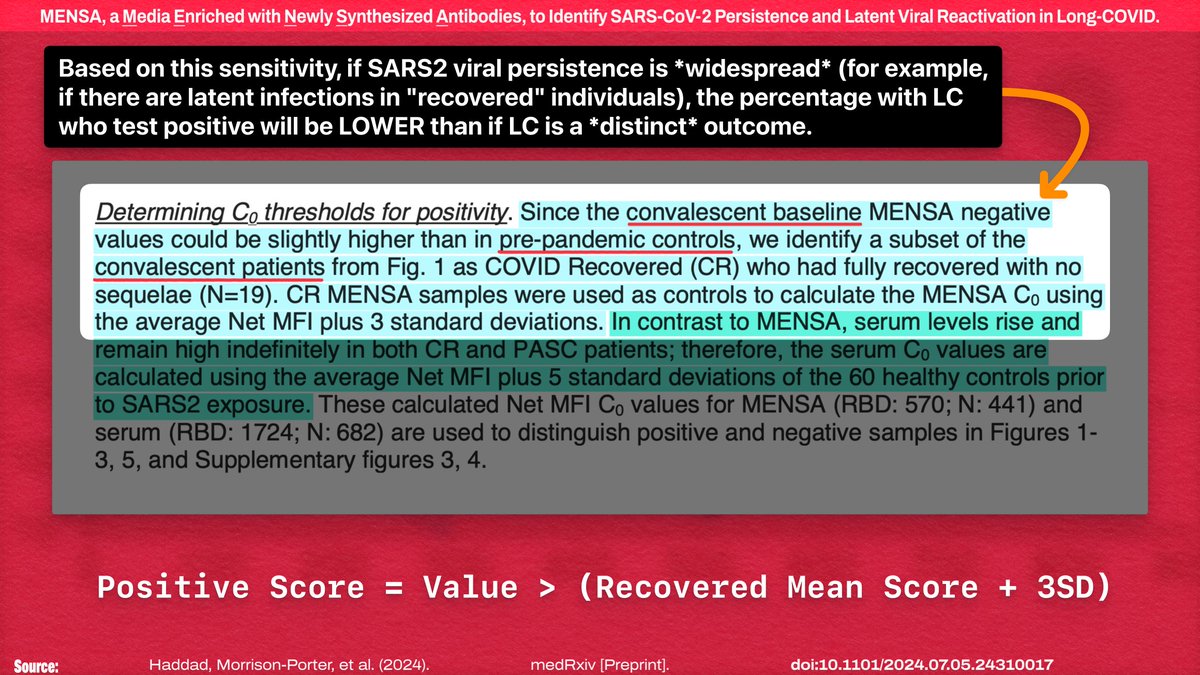
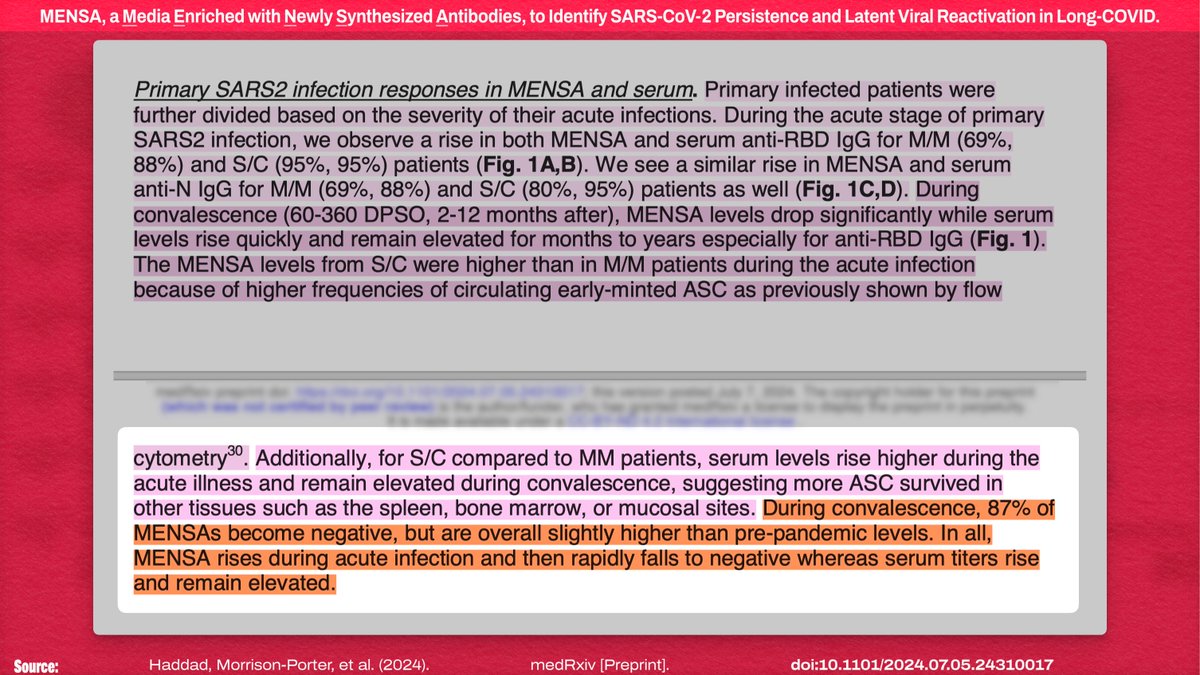
It's also worth noting they confirmed that the convalescent MENSA antibody levels do, in fact, remain HIGHER than the pre-pandemic baseline—and the convalescent MENSA baseline for an individual is also somewhat correlated with acute disease severity!
26/20
26/20
Here's the entire thread on the "Media Enriched with Newly Synthesized Antibodies" preprint available on one page:
And all of the content here is freely licensed for reuse: readwise.io/reader/shared/…
And all of the content here is freely licensed for reuse: readwise.io/reader/shared/…
https://x.com/NickAnderegg/status/1810361088489259381
They were only *validating the ability to DETECT chronic infections,* so we can't infer causality.
HOWEVER!
All of the control group had high SERUM titers for EBV. Thus, in this study, adverse outcomes were *uncorrelated* w/ PRE-COVID EBV exposure!
27/20
HOWEVER!
All of the control group had high SERUM titers for EBV. Thus, in this study, adverse outcomes were *uncorrelated* w/ PRE-COVID EBV exposure!
27/20
https://x.com/NameIsStolen/status/1810411936837939365

• • •
Missing some Tweet in this thread? You can try to
force a refresh


![CONSTITUTION OF THE WHO […] Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition. The health of all peoples is fundamental to the attainment of peace and security and is dependent upon the fullest co-operation of individuals and States. Informed opinion and active co-operation on the part of the public are of the utmost impor...](https://pbs.twimg.com/media/HEYSQdLW0AAomwA.png)


![“8. Performance of Nuclear Power Plants Affected by the Blackout On August 14, 2003, nine U.S. nuclear power plants experienced rapid shutdowns (reactor trips) as a consequence of the power outage. Seven nuclear power plants in Canada operating at high power levels at the time of the event also experienced rapid shutdowns. […]. Many non-nuclear generating plants in both countries also tripped during the event. Numerous other nuclear plants observed disturbances on the electrical grid but continued to generate electrical power without interruption. […] - The severity of the grid transient...](https://pbs.twimg.com/media/G0Q9wDEXkAAknYM.jpg)








