This study is HUGE FOR YOU!
Why? Every hospital, dental, and nursing home corporation around the world use studies designed by the Mark Loeb Group to keep N95s off of your HCW.
As they bend over you in a mask so baggy you can see their toothy smile.
Let me ask you...
/1
Why? Every hospital, dental, and nursing home corporation around the world use studies designed by the Mark Loeb Group to keep N95s off of your HCW.
As they bend over you in a mask so baggy you can see their toothy smile.
Let me ask you...
/1
https://twitter.com/Mark_Ungrin/status/1810789900092154082
Would pulling on an N95 protect you more from airborne anthrax than if you pulled on a medical mask (MM)? From only 3 feet away?
In fact, IT IS AGAINST the proper use of respirators.
OSHA would have you KICKED off the job site.
But when Loeb did it in 2022? The $$$ 🎉🎉🎉
In fact, IT IS AGAINST the proper use of respirators.
OSHA would have you KICKED off the job site.
But when Loeb did it in 2022? The $$$ 🎉🎉🎉
But - once this preprint is published? I do not see how Loeb (2022) is not RETRACTED.🔥🔥🔥
That study compared surgical masks to N95s. It said that surgical (medical) masks are as good as N95s in protection from Covid.
That they are not inferior, aka noninferior, to N95s.
That study compared surgical masks to N95s. It said that surgical (medical) masks are as good as N95s in protection from Covid.
That they are not inferior, aka noninferior, to N95s.
And this stone-cold evisceration of the Loeb group who richly deserve it?
Is a thing of savage beauty.
Starting with - how do you not get infected 3 feet away from some feverish (febrile) C0Vid infected?
(Plus, the 58% asymptomatic transmissions? )

Is a thing of savage beauty.
Starting with - how do you not get infected 3 feet away from some feverish (febrile) C0Vid infected?
(Plus, the 58% asymptomatic transmissions? )


But Loeb's group said, "No way, man. Our people were rolling strapped! From the parking lot to the parking lot." (Universal masking***).
Now, this is where it gets good.
Someone👇 confirmed with a Loeb study member that the N95 group could use medical masks in hallways.
Now, this is where it gets good.
Someone👇 confirmed with a Loeb study member that the N95 group could use medical masks in hallways.


And the people in medical masks could wear N95s anytime they wanted.
Got it? This supposedly very methodological study has people switching anytime they wanted.
Got it? This supposedly very methodological study has people switching anytime they wanted.

And their OWN PLAN said they would have sites with and without universal masking.
Until they changed it after the fact.
AFTER THE FACT! Can we trust them? Surely they have no incentive to lie like rugs, right?
No UNREPORTED conflicts of interests like 7 million dead.
Until they changed it after the fact.
AFTER THE FACT! Can we trust them? Surely they have no incentive to lie like rugs, right?
No UNREPORTED conflicts of interests like 7 million dead.



No conflicts of interest at all, like 16 study members running IPC at their hospital. No pressure from needing to be proved right. No pressure to keep costs low as N95s are spendy!
None like testifying at a trial to deny nurses N95s. With 5 study members.
None like testifying at a trial to deny nurses N95s. With 5 study members.


None like running THE group that the WORLD listened to for a year of death. Or being a member.

No, when the study was abruptly moved from Canada to Egypt, Israel, Pakistan, just as clear evidence was emerging that N95s were better than MM? Nothing suspicious.
And Egypt ending up being the location for finding surgical masks are the same as N95s?
And Egypt ending up being the location for finding surgical masks are the same as N95s?


Nothing against Egypt, it's just where serious issues with women being forced to work, men in N95s, bad ventilation, public transportation in the middle of the first Omicron wave, all caused that effect.
Although...
Although...

The actual data collected was sketch AF. "Perfectly excluded" is not a good phrase to hear about your study.
You been busted, son! Is a rough translation.
You been busted, son! Is a rough translation.

Nothing like a few changes to a study👇. Between 16 IPC directors, you'd think they'd kick all kinds of study a$$, instead of needing midstream changes.
There is more, but I am tired of reading about the Canadian IPC Mafia.
They are very bad people who did a very bad study.
There is more, but I am tired of reading about the Canadian IPC Mafia.
They are very bad people who did a very bad study.

That should be retracted!
They did it! Called for retraction!
/Continued with some thoughts. acpjournals.org/doi/full/10.73…
They did it! Called for retraction!
/Continued with some thoughts. acpjournals.org/doi/full/10.73…

Actual care exposure time to patients in Egypt was about double (very important, not mentioned)?
It has all the outbreaks (mentioned in the study)
It has all the outbreaks (mentioned in the study)


One factor everyone seems to have missed? Maybe I just didn't see it?
Extended use AND re-use of the N95s does not seem to have been factored in.
Fit failure is a huge issue.👇
Loeb does a self-own on this in commenting on his own study.
healthresearch.healthsci.mcmaster.ca/surgical-masks…
Extended use AND re-use of the N95s does not seem to have been factored in.
Fit failure is a huge issue.👇
Loeb does a self-own on this in commenting on his own study.
healthresearch.healthsci.mcmaster.ca/surgical-masks…




Universal masking was not fully explained in the study.
Parking lot to parking lot?
UM in Egypt, Pakistan, Canada - might be all different.
For example, Japan, this hospital had universal masking, but not in break rooms. Led to infections.
ncbi.nlm.nih.gov/pmc/articles/P…
Parking lot to parking lot?
UM in Egypt, Pakistan, Canada - might be all different.
For example, Japan, this hospital had universal masking, but not in break rooms. Led to infections.
ncbi.nlm.nih.gov/pmc/articles/P…

Pakistani where PATIENTS did not adhere to universal masking (UM), despite beng requird to.
Obviously, patients are aerosol src. Also, the antimaskers at the Loeb group included ACH at the various places. THAT IS NOT MEASURED ACH. There is a
researchgate.net/profile/Saerah…
Obviously, patients are aerosol src. Also, the antimaskers at the Loeb group included ACH at the various places. THAT IS NOT MEASURED ACH. There is a
researchgate.net/profile/Saerah…
huge difference - if you ask someone actually experienced with aerosols.
Changing rooms in hospitals - we have no idea of the Egypt set up.
We do know Egyptian HCWs are pretty good at masking up at work. Not in public.
journals.lww.com/joem/fulltext/…
ijic.info/article/view/2…
Changing rooms in hospitals - we have no idea of the Egypt set up.
We do know Egyptian HCWs are pretty good at masking up at work. Not in public.
journals.lww.com/joem/fulltext/…
ijic.info/article/view/2…


Loeb (2022), truly one of the worst studies ever. Giving Walach a run for his money.
My apologies, I forgot to link to the top of the thread for your convenience!
Thank you for getting to here and now knowing how the latest masking RCT is fatally flawed.
The other two main ones are also flawed in the main same way. 3 feet.
Thank you for getting to here and now knowing how the latest masking RCT is fatally flawed.
The other two main ones are also flawed in the main same way. 3 feet.
https://x.com/LazarusLong13/status/1810967035486060866?t=hSDEwzl9qyvZde2pc5pOuw&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh

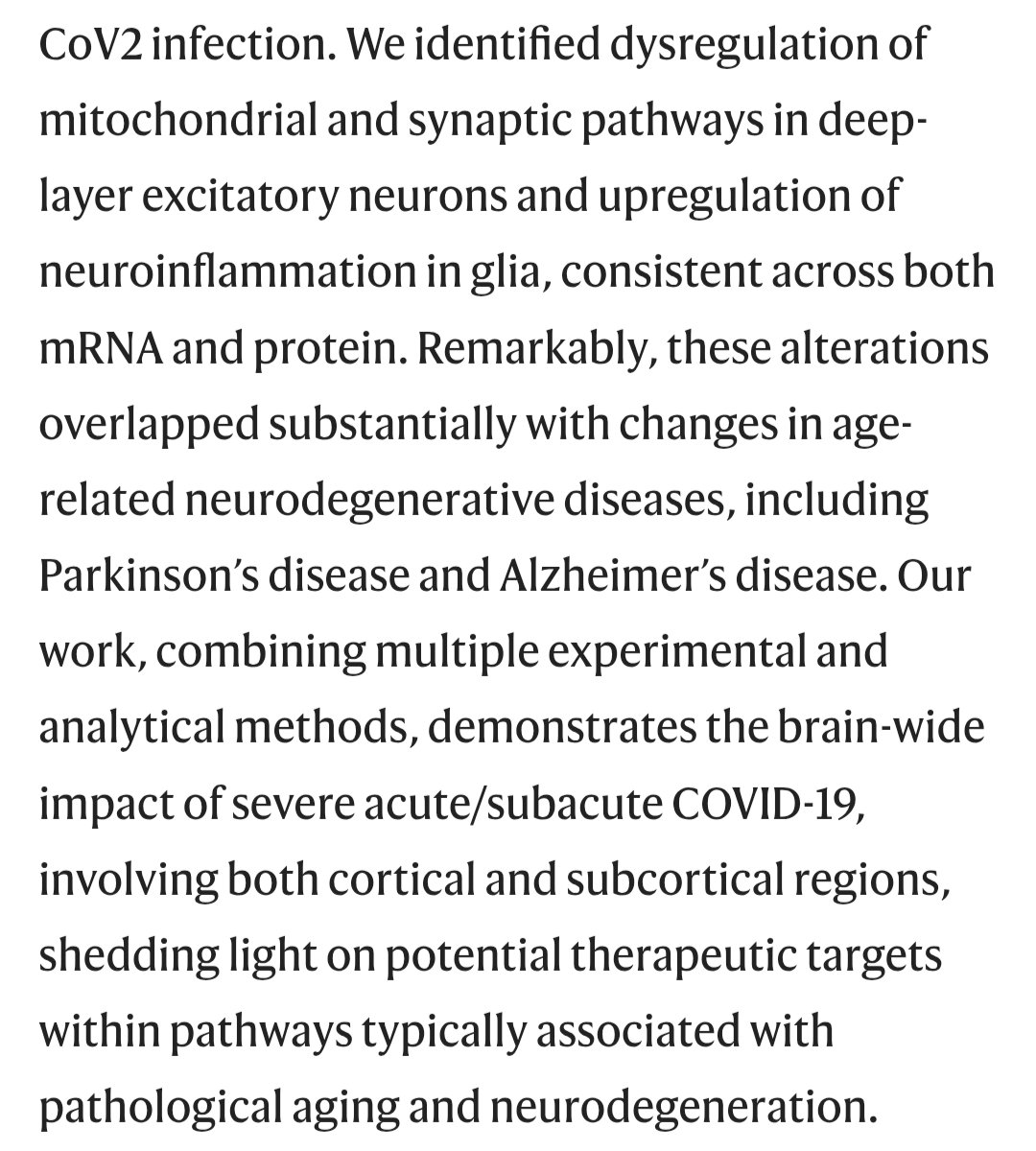
![Opposing effects of SARS-CoV-2/COVID-19 infection and recombinant zoster vaccination on the risk of late-onset Alzheimer disease View ORCID ProfileCarly M. Rose, Shiying Liu, View ORCID ProfileWilliam S. Bush, Jonathan L. Haines, Scott M. Williams, View ORCID ProfileDana C. Crawford N3C Consortium doi: https://doi.org/10.64898/2026.01.21.26344555 This article is a preprint and has not been peer-reviewed [what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.](https://pbs.twimg.com/media/HDht0SUagAAveEw.png)