🧵 The #UKCovidInquiry's first report on 𝗥𝗲𝘀𝗶𝗹𝗶𝗲𝗻𝗰𝗲 𝗮𝗻𝗱 𝗣𝗿𝗲𝗽𝗮𝗿𝗲𝗱𝗻𝗲𝘀𝘀 has been published.
While it addresses many critical areas, it missed significant issues faced by Clinically Vulnerable (CV) families. Here’s what you need to know...
1/ #CVAwareness
While it addresses many critical areas, it missed significant issues faced by Clinically Vulnerable (CV) families. Here’s what you need to know...
1/ #CVAwareness
The report’s focus on general preparedness overlooked the specific needs and challenges of CV people.
Our community faced unique risks and often felt abandoned in the early stages of the pandemic. Our exclusion from *this module* (M1) of the inquiry was a glaring oversight.
2/
Our community faced unique risks and often felt abandoned in the early stages of the pandemic. Our exclusion from *this module* (M1) of the inquiry was a glaring oversight.
2/

Key areas missed include:
💔 The lack of tailored guidance for CV families
😷 Insufficient availability of appropriate PPE for home use
🫂 Inadequate mental health support
CV households had to navigate the crisis alone, compounding their stress and isolation.
3/ #CVAwareness
💔 The lack of tailored guidance for CV families
😷 Insufficient availability of appropriate PPE for home use
🫂 Inadequate mental health support
CV households had to navigate the crisis alone, compounding their stress and isolation.
3/ #CVAwareness
The report also failed to address the systemic issues in healthcare access for CV people.
🏥 Delayed treatments / limited availability of in-person consultations put these vulnerable people at greater risk.
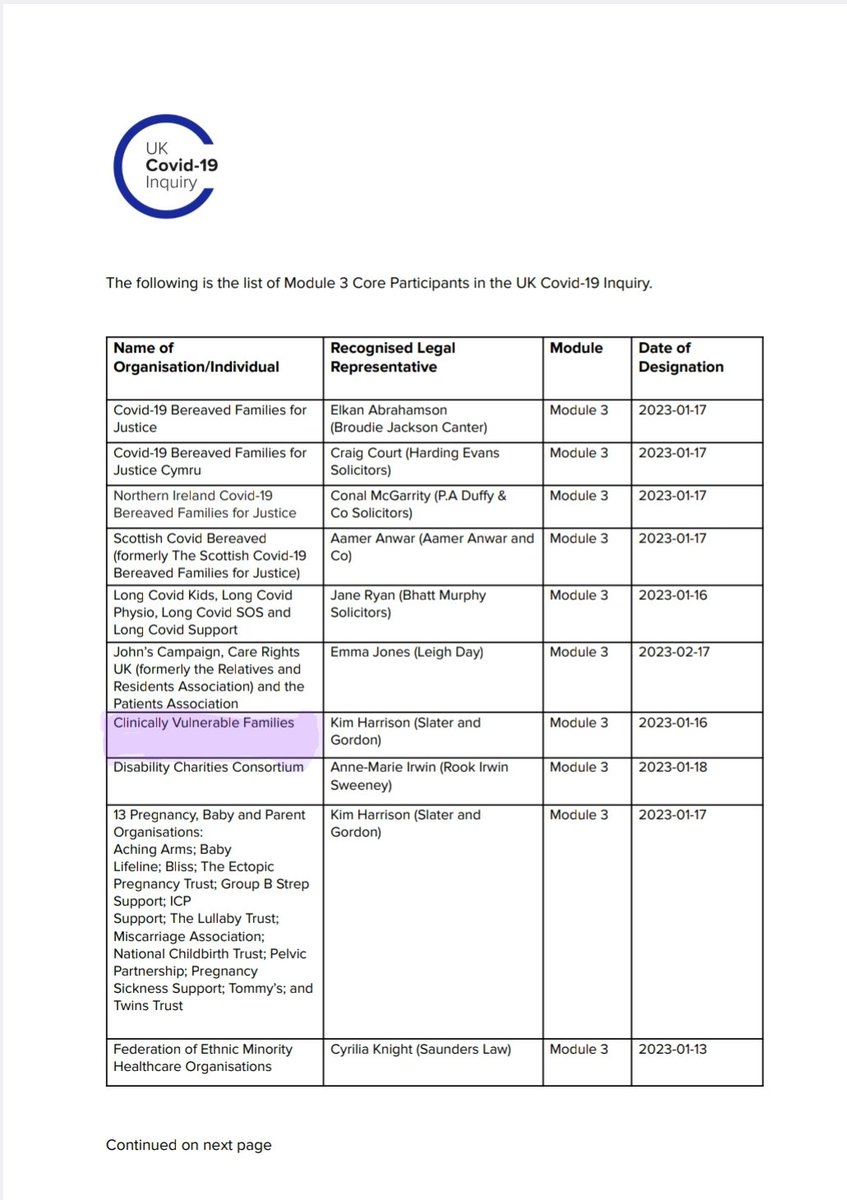
We are in the upcoming Healthcare module (M3).
4/ #CVAwareness
🏥 Delayed treatments / limited availability of in-person consultations put these vulnerable people at greater risk.
We are in the upcoming Healthcare module (M3).
4/ #CVAwareness
👩🏫 Education was another key area. CV children and those in CV households faced challenges without remote learning / safe schools. The lack of appropriate protective policies disrupted their education significantly.
We hope to have the opportunity to assist the Inquiry in M8.
5/
We hope to have the opportunity to assist the Inquiry in M8.
5/
💷 Economic support mechanisms often did not account for the additional costs borne by CV families, such as home delivery charges and increased utility bills due to shielding or informal shielding.
Financial assistance was vital but insufficiently targeted.
6/ #CVAwareness
Financial assistance was vital but insufficiently targeted.
6/ #CVAwareness
For future preparedness, it’s vital that the voices of CV people are heard. Our experiences offer valuable insights into creating a more inclusive and effective response framework.
7/ #CVAwareness
7/ #CVAwareness
![CLINICAL VULNERABILITY IS AN EQUALITY ISSUE We are the highest risk of the worst Covid outcomes. Government policy never considered our new needs. 98% of CV people feel healthcare is unsafe [Mar '24] 98% 82% of CV households lost work / retired early due to high Covid risks [Mar '24] 65% of mask wearers have experienced Mask Abuse [Jan '24] 1 in 5 CV families withdrew children from unsafe schools [Sept '22] Clinically Vulnerable Families](https://pbs.twimg.com/media/GS7qULdWoAEf4uJ.jpg)
The inquiry must broaden its scope to consider the impact on CV communities in upcoming modules. Ignoring their plight risks repeating the same mistakes in future health crises.
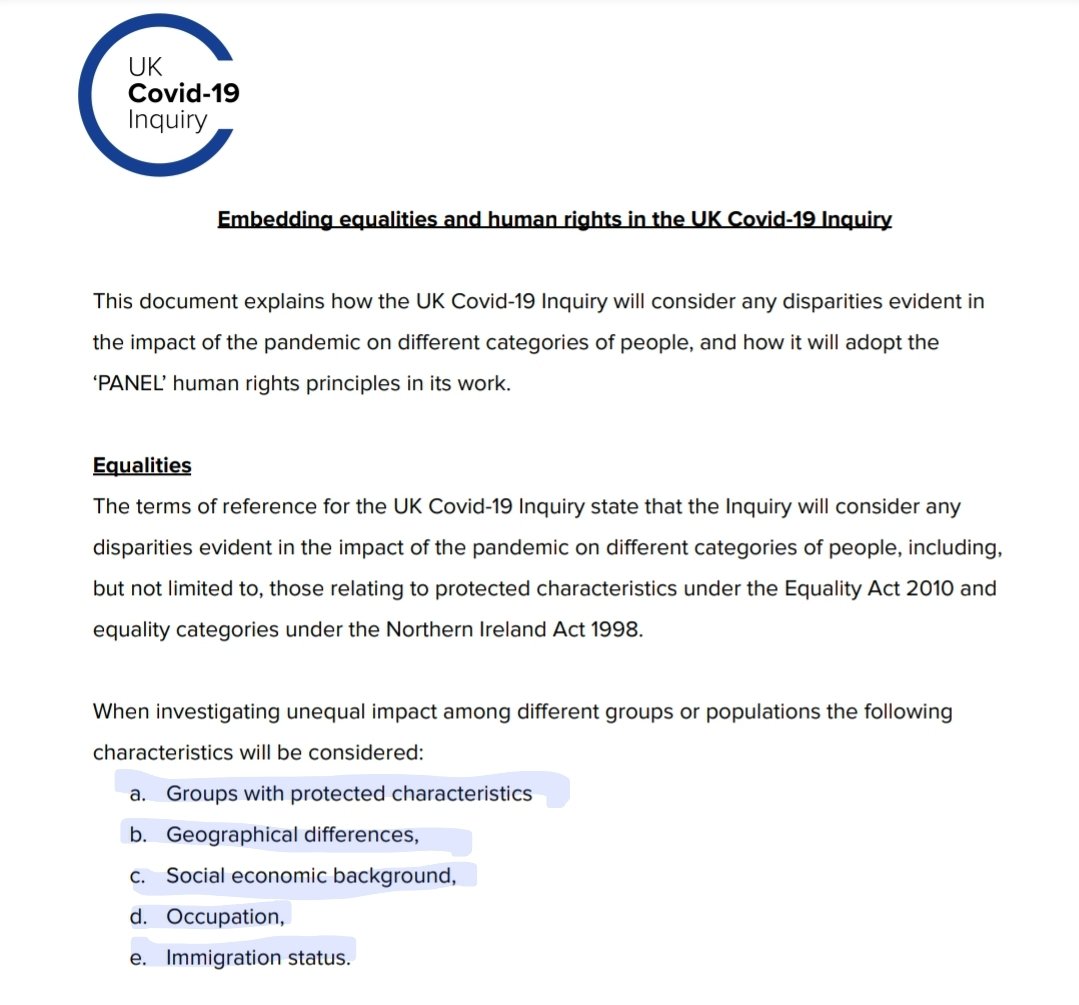
We are still *not* identified in their Equalities and Human Rights statement:
8/ #CVAwareness
We are still *not* identified in their Equalities and Human Rights statement:
8/ #CVAwareness
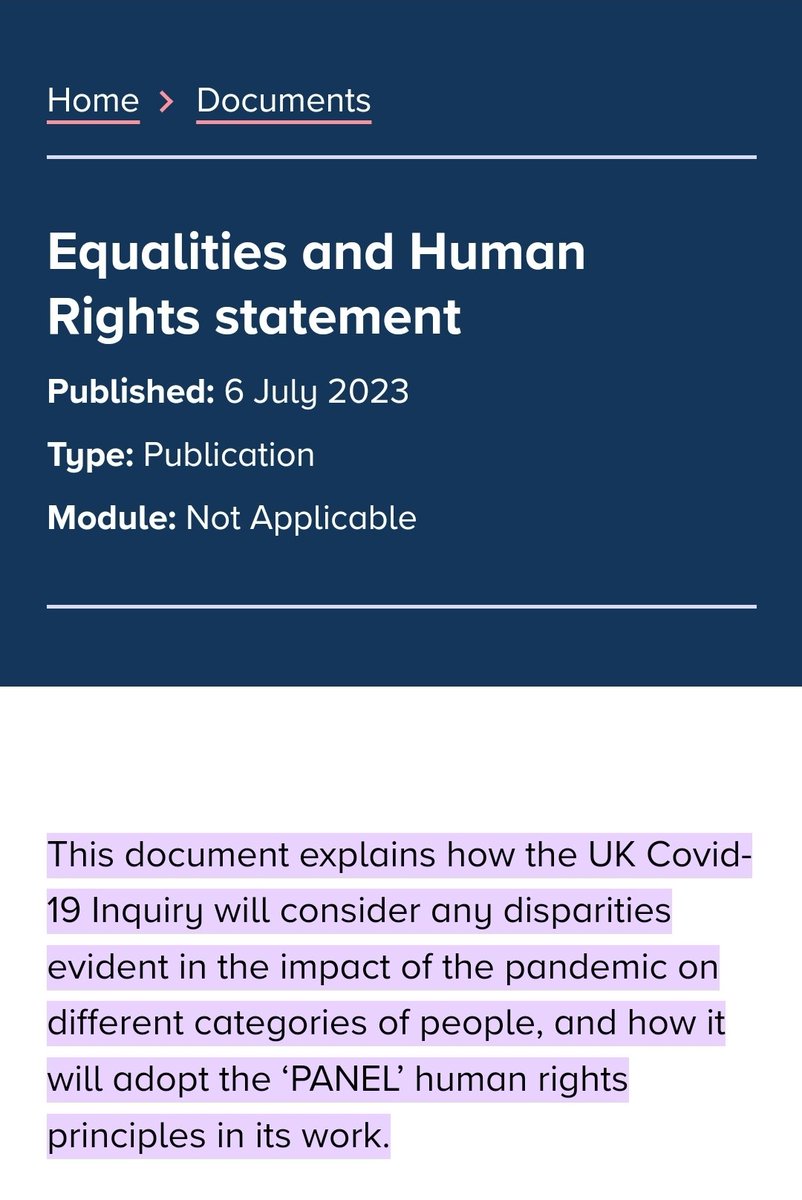
We have raised concerns to the that we are missing from this statement for a considerable length of time now. Perhaps almost 18 months?
Equity can only be achieved if we recognise that people have different needs and circumstances. #CVAwareness !
9/
Equity can only be achieved if we recognise that people have different needs and circumstances. #CVAwareness !
9/
https://x.com/cv_cev/status/1778356063055602081?t=e4MQOn97JF8UFPBtPnfZoA&s=19
For more detailed information on the report, visit the UK COVID-19 Inquiry website.
Share your thoughts with us below.
10/ #CVAwareness
covid19.public-inquiry.uk/reports
Share your thoughts with us below.
10/ #CVAwareness
covid19.public-inquiry.uk/reports
If you are interested in contributing to our work and you come from a Clinically Vulnerable household.
STEP 1: Join us on FB
11/ #CVAwarenessfacebook.com/groups/clinica…
STEP 1: Join us on FB
11/ #CVAwarenessfacebook.com/groups/clinica…
STEP 2: Sign up to our online event to meet our Covid-19 Inquiry legal team on 24th July.
* Apply by Monday 22nd July *
⬇️⬇️⬇️
⬆️⬆️⬆️
STEP 3: Keep fighting for #CVAwareness and #CVRights 💪
12/ clinicallyvulnerable.org
* Apply by Monday 22nd July *
⬇️⬇️⬇️
⬆️⬆️⬆️
STEP 3: Keep fighting for #CVAwareness and #CVRights 💪
12/ clinicallyvulnerable.org

• • •
Missing some Tweet in this thread? You can try to
force a refresh