
Let me start by saying AAAAAAAAAAAAAAAAAAAAAA.
Turns out SARS-CoV-2 RAPIDLY infects the NERVOUS SYSTEM long BEFORE it even enters the bloodstream.
These findings have huge implications! Here's an analysis of the study, written for a general audience. (Sorry in advance!)
1/many![Published July 28, 2024 in IJMS: "SARS-CoV-2 Rapidly Infects Peripheral Sensory and Autonomic Neurons, Contributing to Central Nervous System Neuroinvasion before Viremia" Abstract: "...little attention has been paid to susceptibility of the PNS to infection [by SARS-CoV-2] or to its contribution to CNS invasion. Here we show that sensory and autonomic neurons in the PNS are susceptible to productive infection with SARS-CoV-2 and outline physiological and molecular mechanisms mediating neuroinvasion. Our infection of K18-hACE2 mice, wild-type mice, and golden Syrian hamsters...](/images/1px.png)
Turns out SARS-CoV-2 RAPIDLY infects the NERVOUS SYSTEM long BEFORE it even enters the bloodstream.
These findings have huge implications! Here's an analysis of the study, written for a general audience. (Sorry in advance!)
1/many
![Published July 28, 2024 in IJMS: "SARS-CoV-2 Rapidly Infects Peripheral Sensory and Autonomic Neurons, Contributing to Central Nervous System Neuroinvasion before Viremia" Abstract: "...little attention has been paid to susceptibility of the PNS to infection [by SARS-CoV-2] or to its contribution to CNS invasion. Here we show that sensory and autonomic neurons in the PNS are susceptible to productive infection with SARS-CoV-2 and outline physiological and molecular mechanisms mediating neuroinvasion. Our infection of K18-hACE2 mice, wild-type mice, and golden Syrian hamsters...](https://pbs.twimg.com/media/GTn4kqaWkAASZTk.jpg)
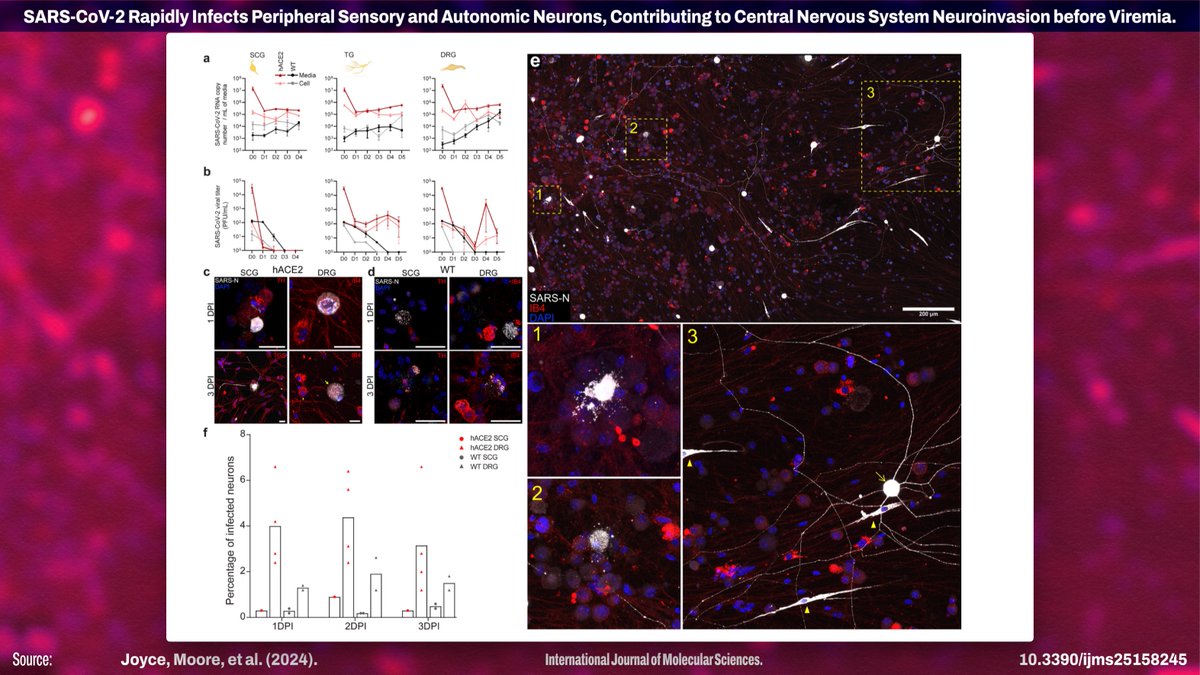
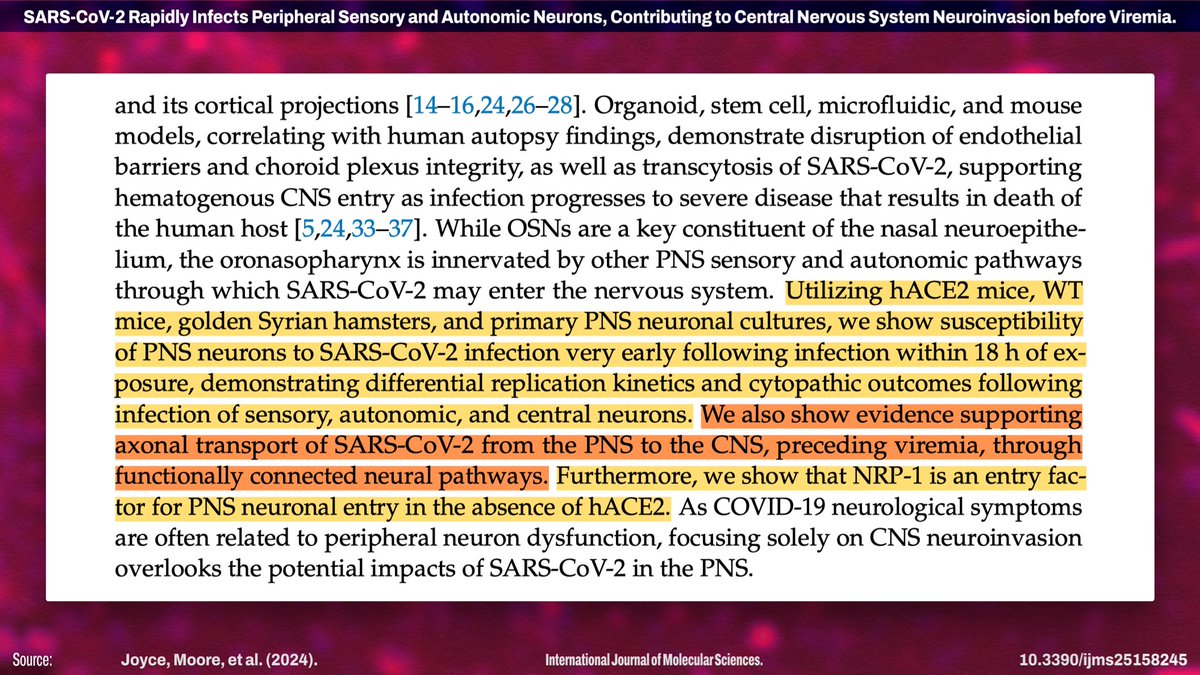
Overall, it's pretty extensive: They examined the productivity of neuronal infection in multiple animal models and multiple neuronal cell cultures, and found productive neuronal infection across the board.
It's also a long one, but we'll pick up the pace as we go!
2/
It's also a long one, but we'll pick up the pace as we go!
2/
So, as you may already know, neurological symptoms are actually VERY common when it comes to COVID, with several different types of neurological issues being notable features of Long COVID. There's seriously so much evidence beyond these 13 citations!
3/
3/
!["Up to 80% of people infected with SARS-CoV-2, the virus responsible for COVID-19, report neurological symptoms. ... including [with] sensory and autonomic systems [1–3]. Both central and peripheral symptoms, such as fatigue, memory issues, “brain fog”, hyper/hypoesthesia, and autonomic dysfunction, can persist as part of postCOVID-19 syndrome (“long COVID”) long after acute infection [4]. Detection of the virus, viral RNA, and antigens in the cerebrospinal fluid and brains of COVID-19 patients indicates SARS-CoV-2 is neuroinvasive, which has also been documented for common cold and ep...](https://pbs.twimg.com/media/GTn4uWGWkAANAnX.jpg)
The ability of SARS-CoV-2 to invade the nervous system is not news on its own! (For example, see )
This study, instead, looks at all the other possible routes of neuroinvasion that have been somewhat neglected UNTIL now!
4/
pandemicpatients.org/home/covid-19-…
This study, instead, looks at all the other possible routes of neuroinvasion that have been somewhat neglected UNTIL now!
4/
pandemicpatients.org/home/covid-19-…
https://x.com/NickAnderegg/status/1767727732274626937
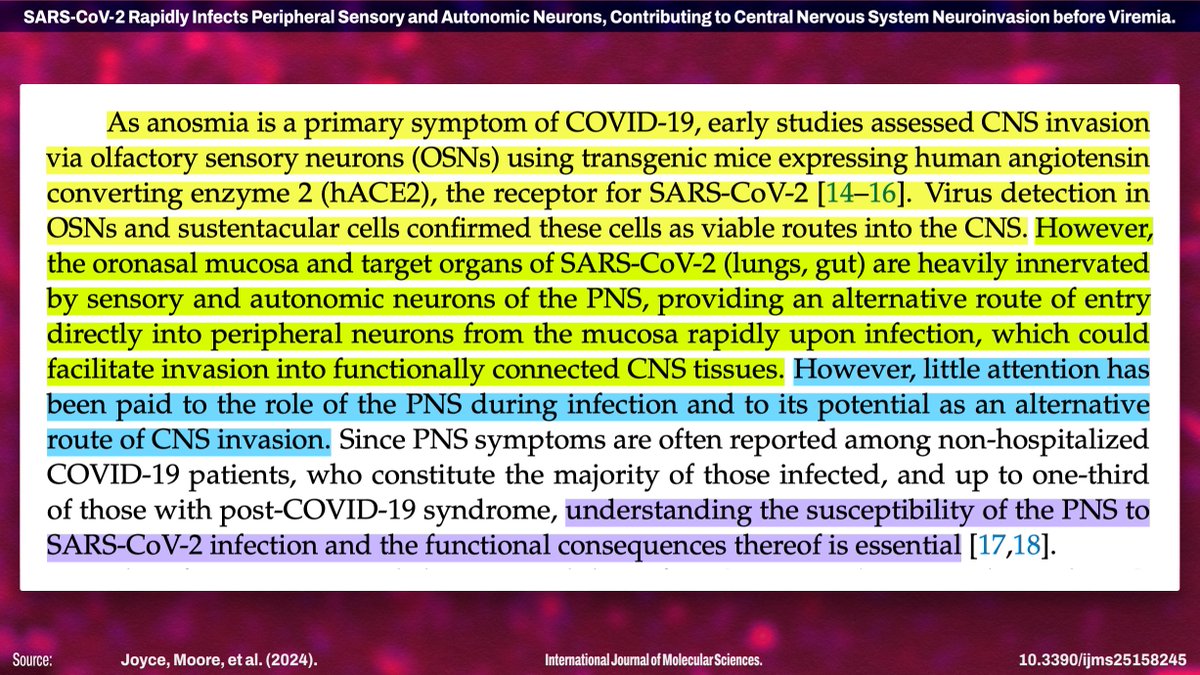
Their goal was to "determine if infection of the PNS [peripheral nervous system] preceded and contributed to CNS [central nervois system] infection," by examining the mucosal tissues with lots of PNS connections.
[Spoiler: Turns out, it super-duper does.]
5/
[Spoiler: Turns out, it super-duper does.]
5/
!["To determine if infection of the PNS preceded and contributed to CNS infection, we assessed early neuroinvasion of CNS tissues functionally connected to peripheral neurons innervating oronasal and gut mucosa (lumbosacral spinal cord and specific brain regions [olfactory bulb, cortex, hippocampus, brainstem, cerebellum]). ... We focused on early neuroinvasion of ancestral SARS-CoV-2, as differences in neurological symptoms between variants are only beginning to be reported. A recent epidemiological study has shown the odds ratio for developing post-COVID-19 syndrome following infectio...](https://pbs.twimg.com/media/GTn4zPBXkAAGgi-.jpg)
In the first reported study, they did a comparison between:
- "wild type" mice (WT)
- human ACE2-expressing mice (hACE2)
which were exposed to the SARS-CoV-2 variant from 2020—specifically, the isolate from one of the first cases detected in the US! (So, first wave.)
6/
- "wild type" mice (WT)
- human ACE2-expressing mice (hACE2)
which were exposed to the SARS-CoV-2 variant from 2020—specifically, the isolate from one of the first cases detected in the US! (So, first wave.)
6/
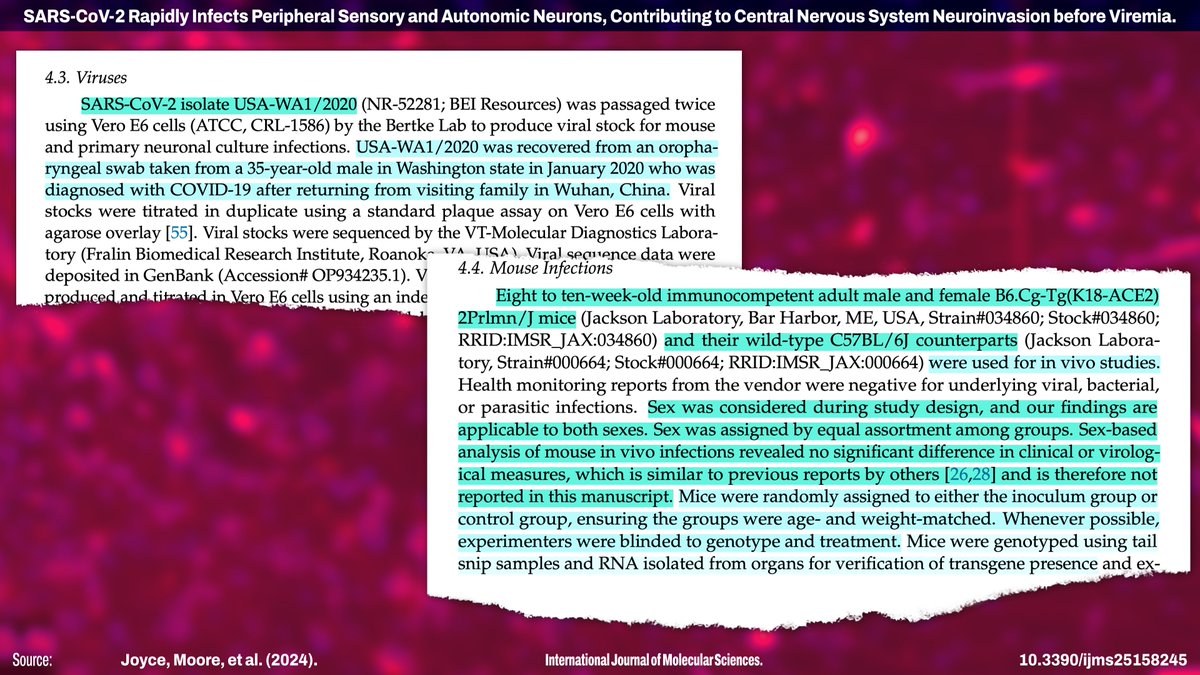
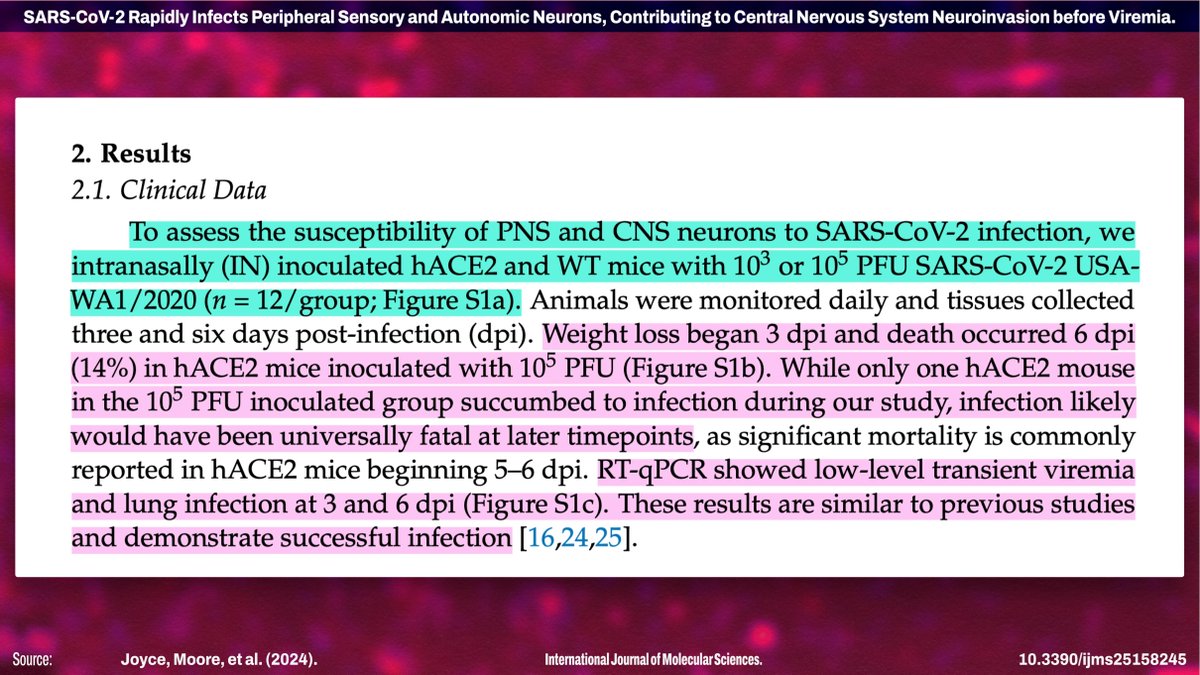
The mice were innoculated with SARS-CoV-2 (by spraying it up their noses), then letting it run its course, with various diagnostic tests along the way.
They confirmed low levels of blood and lung infection at 3 and 6 days post-infection in both groups, as expected!
7/
They confirmed low levels of blood and lung infection at 3 and 6 days post-infection in both groups, as expected!
7/
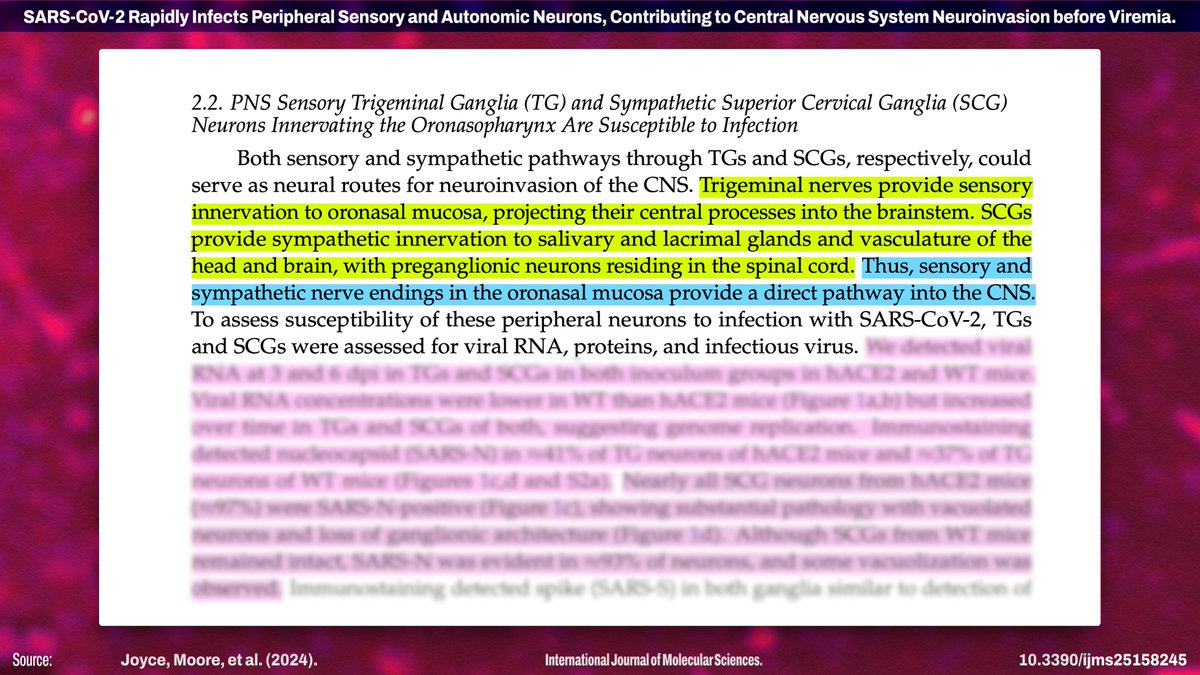
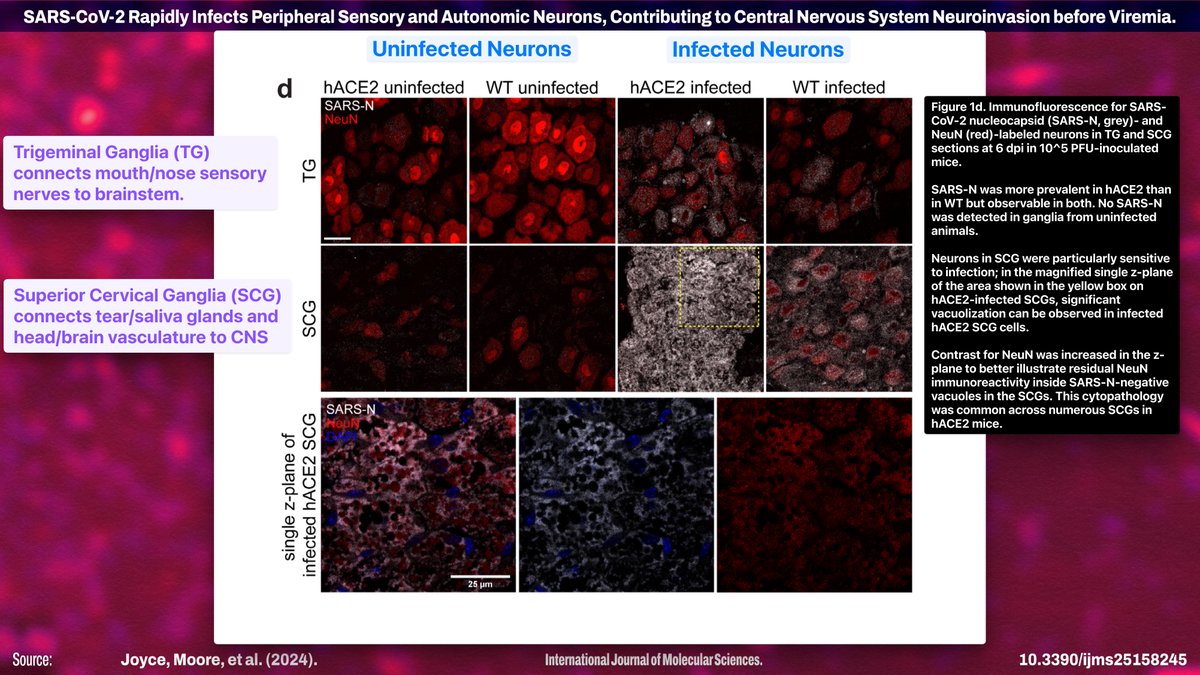
The Trigeminal Ganglia (TG) connects *sensory nerves* from the mouth and nose to the brainstem.
The Superior Cervical Ganglia (SCG) is part of the *sympathetic nervous system*, connecting glands (saliva, tears) and head/brain vasculature to the CNS.
8/
The Superior Cervical Ganglia (SCG) is part of the *sympathetic nervous system*, connecting glands (saliva, tears) and head/brain vasculature to the CNS.
8/
Before we get to the results, I want to pause to note that if you are reading this, what happened to these mice has DEFINITELY NOT happened to you to anywhere near the same extent! If the mice weren't euthanized for dissection, they would have ALL died from the infection.
9/
9/
SARS-CoV-2 was found in both TGs and SCGs, in BOTH groups—hACE2 mice AND WT mice.
In both group, the viral concentration increased over time, suggesting there was active viral genome replication occurring.
But, hACE2 neurons in the SCG, in particular, basically fell apart.
10/
In both group, the viral concentration increased over time, suggesting there was active viral genome replication occurring.
But, hACE2 neurons in the SCG, in particular, basically fell apart.
10/
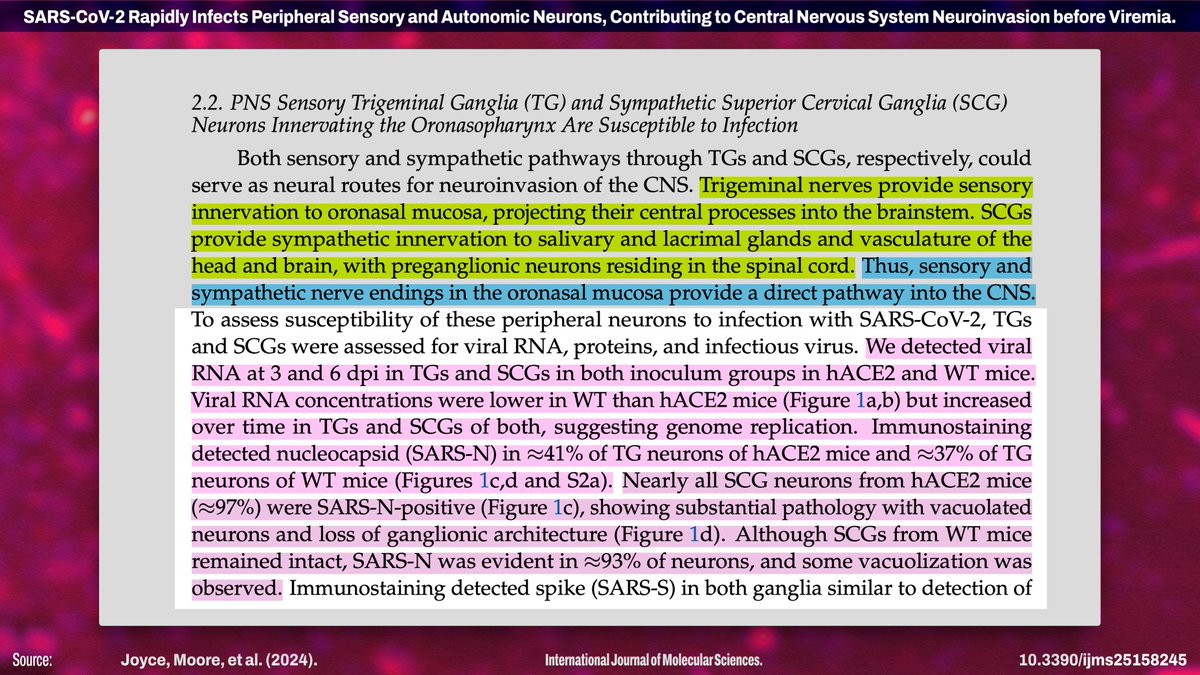
In the hACE2 mice infected with SARS-CoV-2, about 97% of the neurons in the SCG were positive for the nucleocapsid (N) protein, "showing substantial pathology with vacuolated neurons and loss of ganglionic architecture."
So... not great.
11/
So... not great.
11/
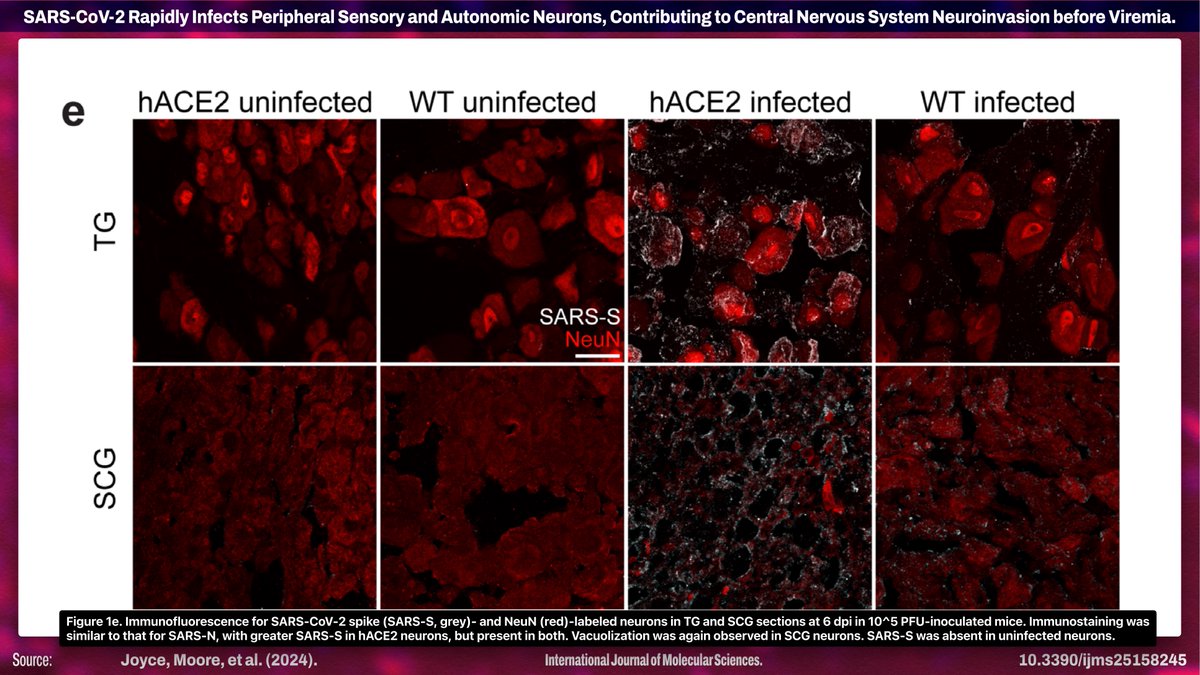
If you're now wondering about the spike protein: They found it in both ganglia, in hACE2 and WT groups!
However, infectious virus "was not detected in SCGs." Why?
"SARS-CoV-2 may have produced such significant cytotoxicity that production of viral progeny was impossible."
12/
However, infectious virus "was not detected in SCGs." Why?
"SARS-CoV-2 may have produced such significant cytotoxicity that production of viral progeny was impossible."
12/
That's a very scientific way of saying "it so thoroughly damaged the cells of the hACE2 Superior Cervical Ganglia that they kinda stopped being cells."
Thus, they conclude "TGs may serve as a route of CNS invasion" AND "neuroinvasion can occur independently of hACE2."
13/
Thus, they conclude "TGs may serve as a route of CNS invasion" AND "neuroinvasion can occur independently of hACE2."
13/
Now that we've have the conceptual groundwork for what they're doing, we can go a bit quicker! I'm also going to stop writing out terms from the excerpts that are identified by acronyms, for brevity.
Next up, nerves for sensory information from limbs and internal organs!
14/
Next up, nerves for sensory information from limbs and internal organs!
14/
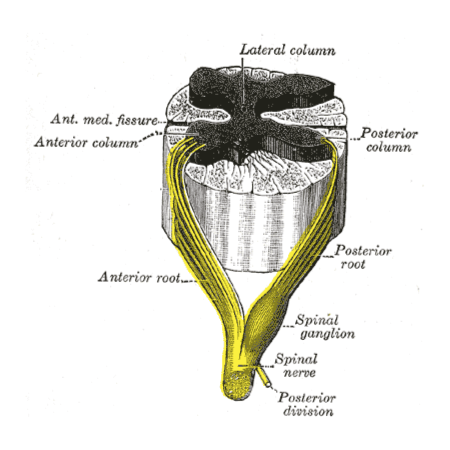
The LS-DRG is a PNS nerve cluster that "conveys sensory information (pain, pressure, position) from the periphery [limbs] and internal organs" to the LS-SC. The LS-SC is the part of the spinal cord where the peripheral nerve bundle connects to the CNS.
15/
15/
Viral RNA was found in both LS-DRG and spinal cord, for both the hACE2 and WT mice.
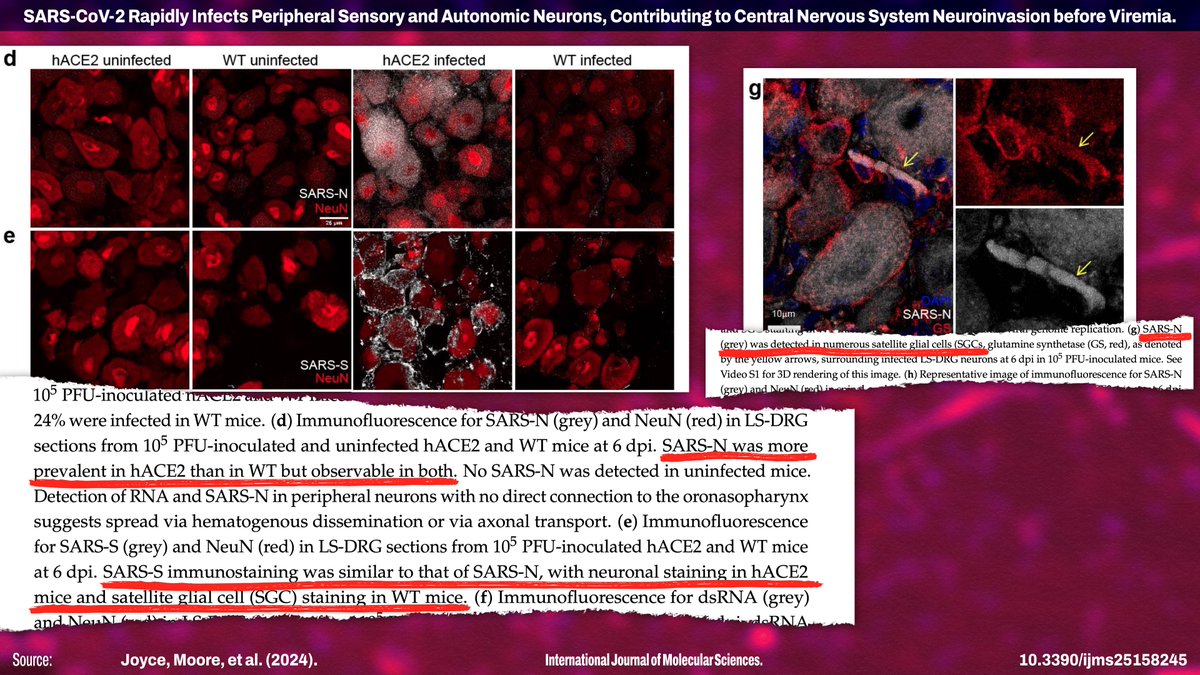
The nucleocapsid protein was found in about 42% of LS-DRG neurons of hACE2 mice (24% for WT mice), and results for the spike protein were similar.
Satellite glial cells were also infected.
16/
The nucleocapsid protein was found in about 42% of LS-DRG neurons of hACE2 mice (24% for WT mice), and results for the spike protein were similar.
Satellite glial cells were also infected.
16/
Furthermore, they stained the spinal cord nerve cells and found a diffuse signal (not pictured).
"These data further demonstrate that PNS sensory neurons, as well as functionally connected neurons in the spinal cord, are susceptible to infection with SARS-CoV-2."
17/
"These data further demonstrate that PNS sensory neurons, as well as functionally connected neurons in the spinal cord, are susceptible to infection with SARS-CoV-2."
17/
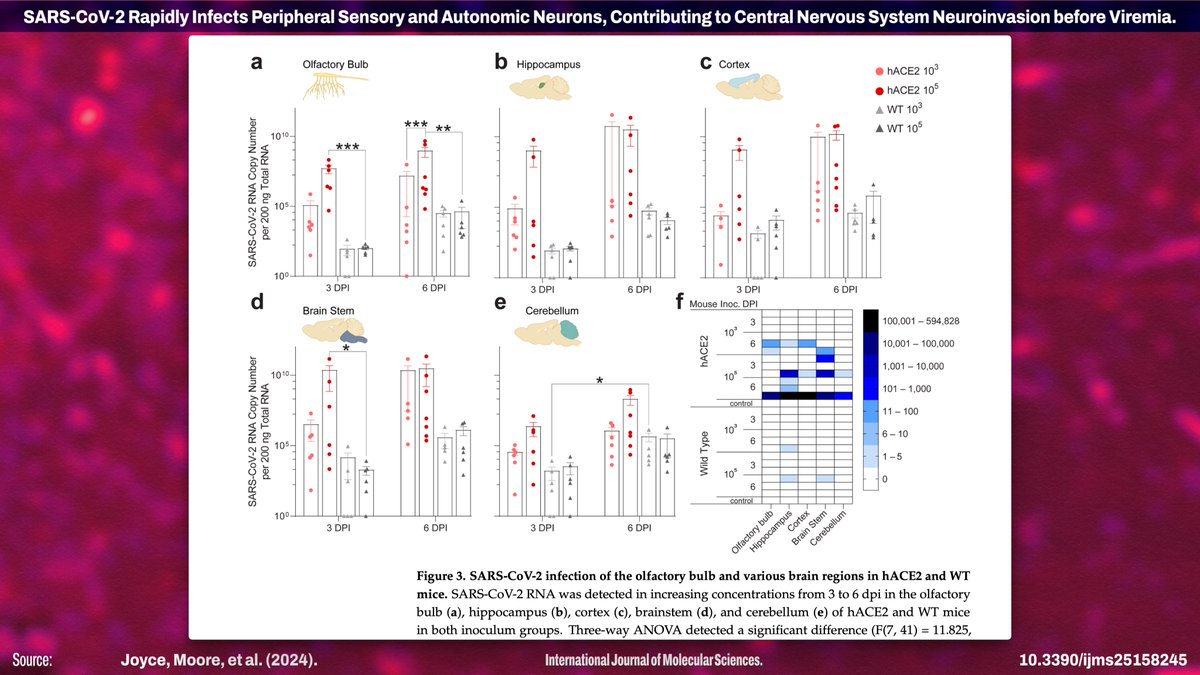
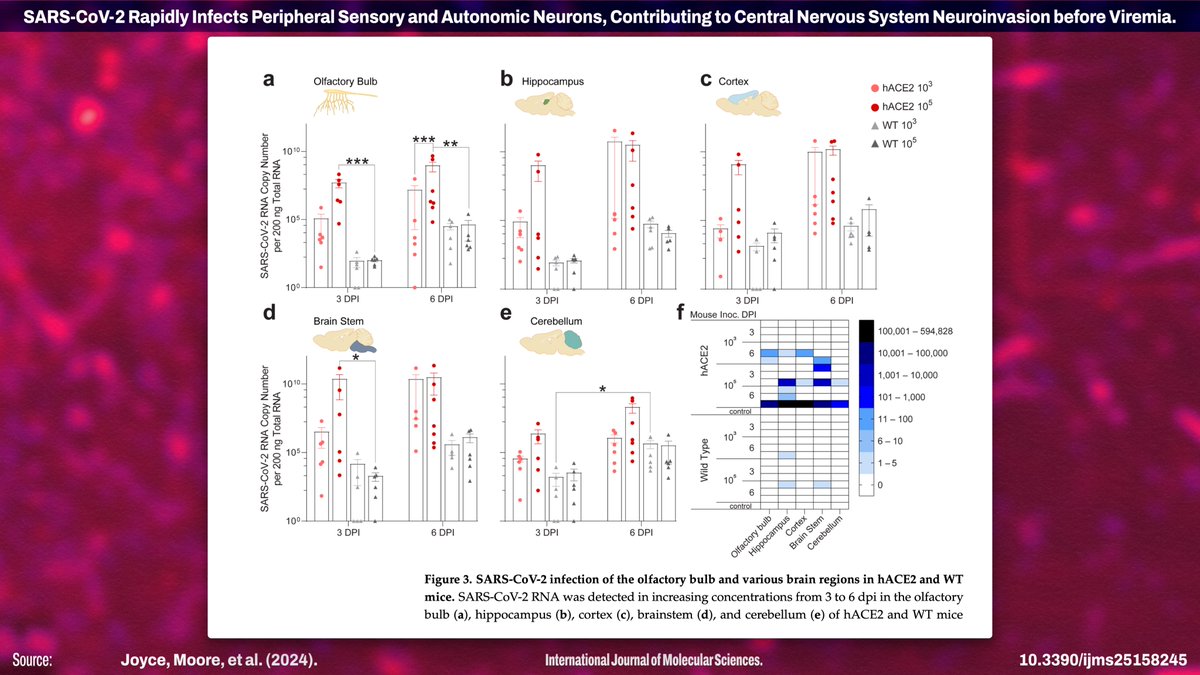
Next, they looked at multiple brain regions (olfactory bulb, hippocampus, cortex, brainstem, and cerebellum).
They found viral RNA in all of them at 3 days post-infection, which then increased at 6 dpi.
The quantities of RNA in WT mice suggests ACE2-independent spread!
18/
They found viral RNA in all of them at 3 days post-infection, which then increased at 6 dpi.
The quantities of RNA in WT mice suggests ACE2-independent spread!
18/
!["2.4. Individual Brain Regions Support Varying Levels of Viral Invasion and Reproduction To determine if SARS-CoV-2 was present in specific brain regions with functional connections to PNS ganglia, we assessed the olfactory bulb, hippocampus, cortex, brainstem, and cerebellum. Previous studies have tested brain homogenates to assess viral RNA and infectious virus in the brain, which does not allow for spatial analysis and may obscure detection of low levels of virus in specific brain regions [14,16,26–28]. We detected viral RNA in all brain regions at 3 dpi, which increased by 6 dpi, ...](https://pbs.twimg.com/media/GTn6NNwXUAAi0-r.jpg)
Viral RNA and infectious virus were recovered from allll over the brains of both the hACE2 mice and (unexpectedly) the WT mice. They note that "viral RNA and the infectious virus were readily recoverable throughout WT brains"
19/
19/
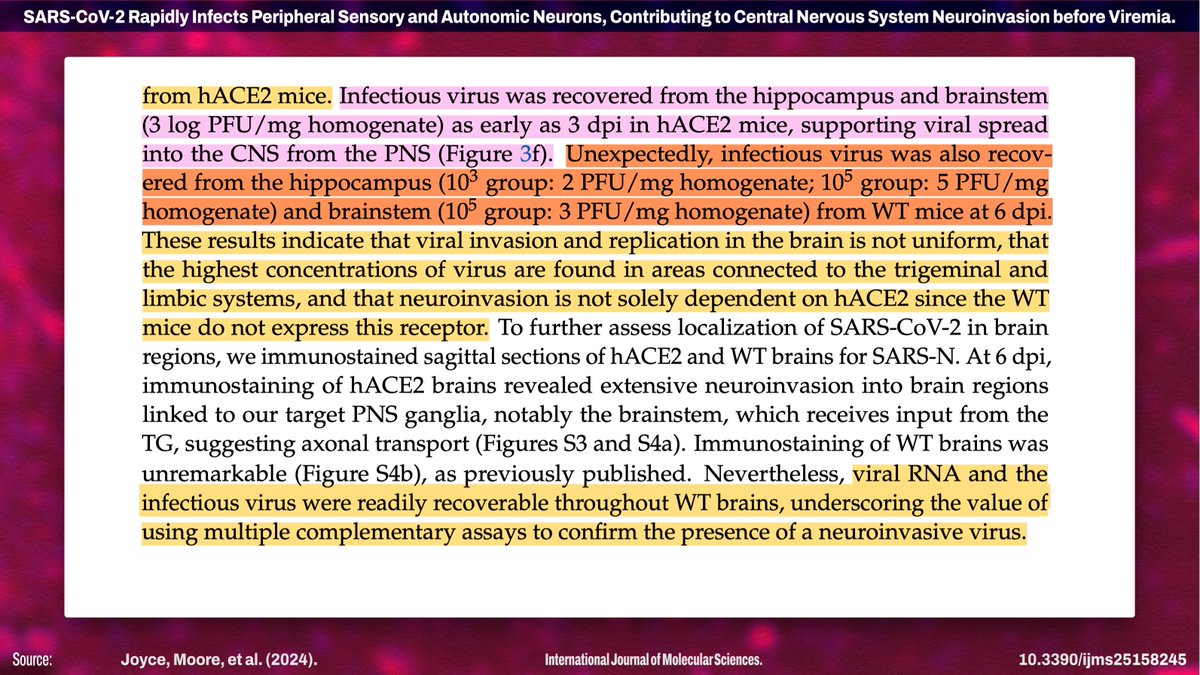
They conclude: "These results indicate that viral invasion and replication in the brain is not uniform, that the highest concentrations of virus are found in areas connected to the trigeminal and limbic systems, and that neuroinvasion is not solely dependent on hACE2..."
20/
20/
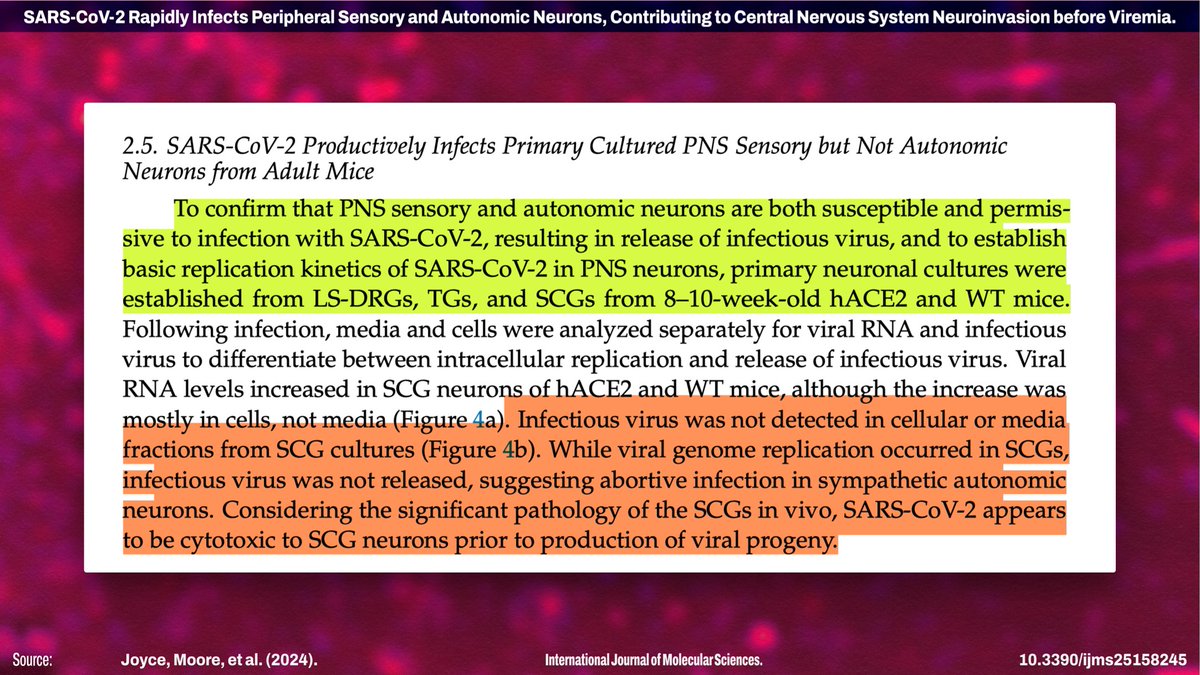
Then, when they cultured the virus in neurons, they found infectious virus in the PNS sensory neurons, but not the autonomic neurons. This suggests that while autonomic neurons can be infected, they can't produce viral progeny.
Weird!
21/
Weird!
21/
Headline result: Does neuroinvasion of the PNS/CNS occur BEFORE the virus enters the bloodstream?
"By 18 [hours post-infection], although no viral RNA was detected in blood..., viral RNA was detected in all PNS ganglia and the majority of functionally connected CNS tissues"
22/
"By 18 [hours post-infection], although no viral RNA was detected in blood..., viral RNA was detected in all PNS ganglia and the majority of functionally connected CNS tissues"
22/
Then, at 42 hours post infection, the virus was still only found in the blood of a single hACE2 mouse, but there was increased viral RNA in the brain.
They replicated this study with a different animal model and got roughly the same results. This is thorough work!
23/
They replicated this study with a different animal model and got roughly the same results. This is thorough work!
23/
In the other animal model (hamsters), they conclude "neuroinvasion occurs rapidly..., is mediated by invasion of and transport along neurons, can occur independent of hACE2, and functionally impacts PNS sensory neurons, resulting in allodynia [pain from mild stimulation]."
24/
24/
So what's the deal with non-hACE2 mice and hamsters getting infected? How is infection occurring independent of ACE2 receptors?
It just uses a different receptor to enter the cells: NRP-1.
It was previously known SARS-CoV-2 could use this receptor, and this supports that!
25/
It just uses a different receptor to enter the cells: NRP-1.
It was previously known SARS-CoV-2 could use this receptor, and this supports that!
25/
!["2.7. Neuronal Entry in the PNS Involves Neuropilin-1 (NRP-1) NRP-1 has been shown to interact with SARS-S, thereby enhancing viral binding/ entry in non-neuronal cells [30-32]. ...we investigated the contribution of NRP-1 to entry in primary PNS sensory neurons. ... Primary cultured LS-DRG neurons from hACE2 and WT mice were pretreated with EG00229, a selective NRP-1 antagonist, infected with SARS-CoV-2, and viral RNA concentrations were assessed 2 dpi, the first peak for genome replication as determined in our growth curves. Neurons were observed daily for cytopathic effect from tre...](https://pbs.twimg.com/media/GTn6eqgXgAAuYjk.jpg)
Three big takeways:
1. SARS-CoV-2 can infect PNS neurons very rapidly after exposure, long before it gets near the bloodstream
2. The virus can move from PNS to CNS via axonal transport before it enters the blood
3. NRP-1 is how it does it independently of hACE2
26/
1. SARS-CoV-2 can infect PNS neurons very rapidly after exposure, long before it gets near the bloodstream
2. The virus can move from PNS to CNS via axonal transport before it enters the blood
3. NRP-1 is how it does it independently of hACE2
26/
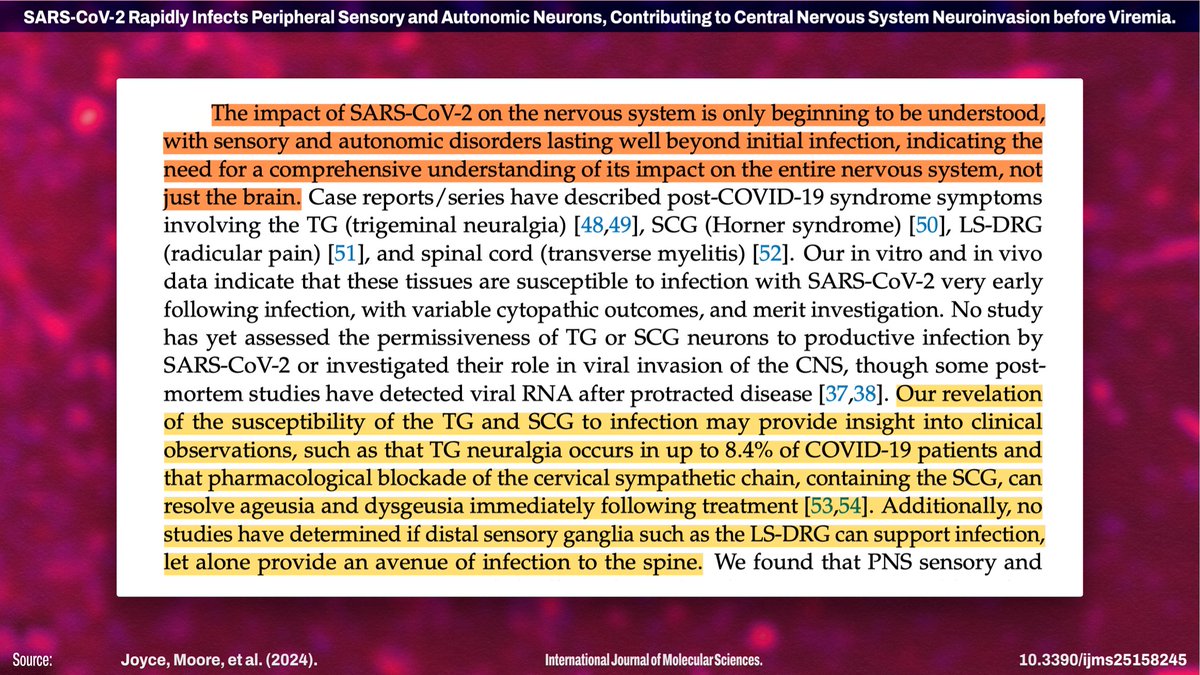
But here's the thing: Not ALL of these results are new. Some of them are just now being tied together neatly in this one study.
IMO, widespread short-sighted research practices made these conclusions take so long to reach. The ball is being dropped with autopsy studies!
27/
IMO, widespread short-sighted research practices made these conclusions take so long to reach. The ball is being dropped with autopsy studies!
27/
!["Invasion of the brainstem along projections of the TG could damage nuclei important in cardiorespiratory regulation, a feature of severe COVID-19, and at least one imaging study of a COVID-19 patient with AHNE suggested invasion of the brainstem via the TG [7]. While viral RNA and proteins have been detected in salivary glands of COVID-19 patients, and infectious virus has been recovered from saliva, no assessments of the SCG have been made in human autopsies [39-42]. The SCG provides sympathetic nervous system innervation to the oronasal mucosa, salivary and lacrimal glands, and oron...](https://pbs.twimg.com/media/GTn81-GX0AANOso.jpg)
At this point, we are only BEGINNING to understand the impact COVID can have on the brain and nervous system.
You know what we DO understand well? How to filter airborne particulate! Wear a filtering respirator in shared air to protect yourself.
28/
You know what we DO understand well? How to filter airborne particulate! Wear a filtering respirator in shared air to protect yourself.
28/
https://x.com/NickAnderegg/status/1769194320249201045
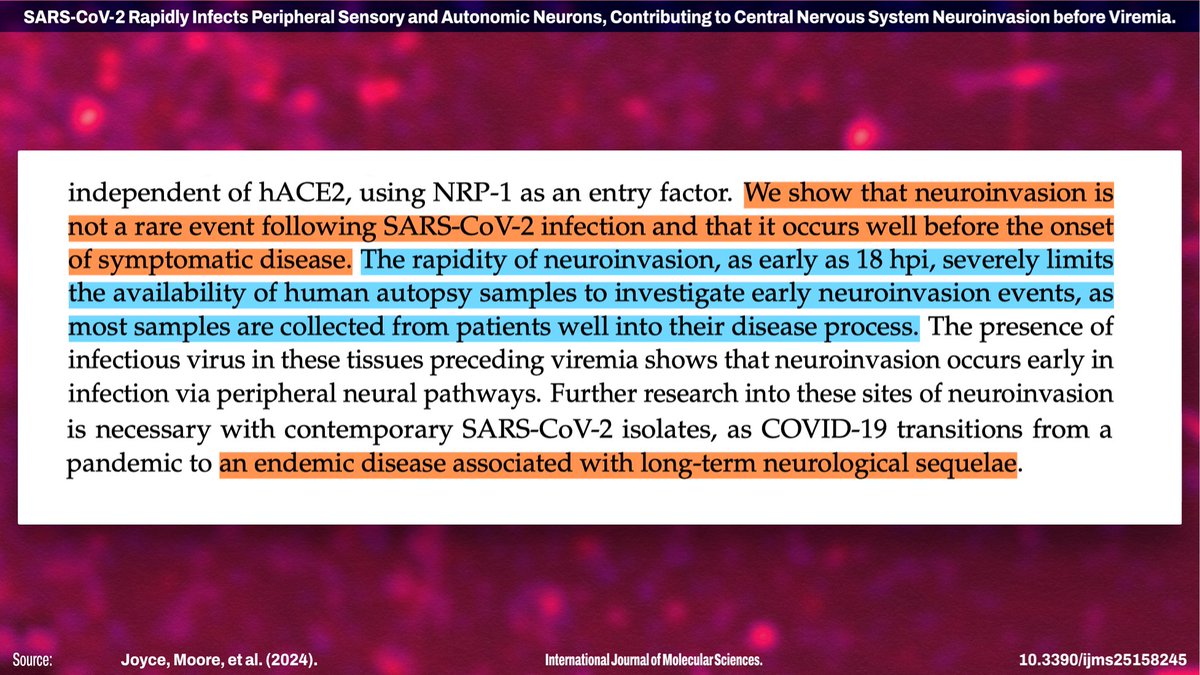
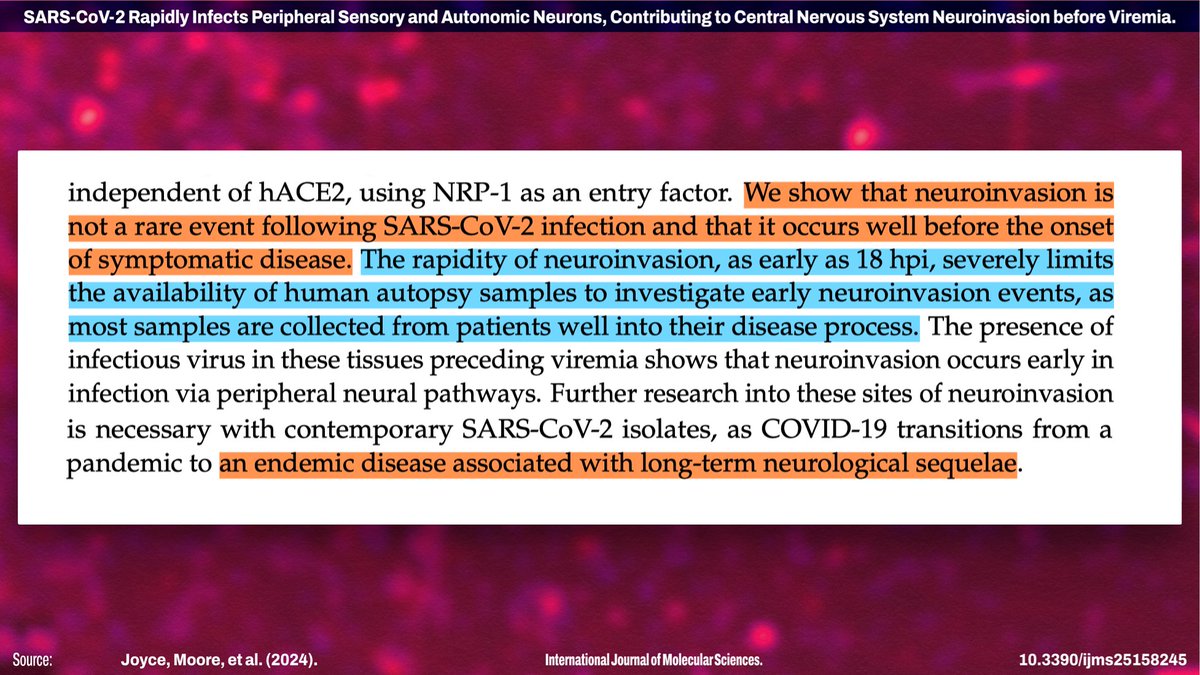
Neuroinvasion "is not a rare event following SARS-CoV-2 infection" and occurs "well before the onset of symptomatic disease."
Now that the pandemic has been DECLARED over, COVID-19 is transitioning to "an endemic disease associated with long-term neurological sequelae."
29/
Now that the pandemic has been DECLARED over, COVID-19 is transitioning to "an endemic disease associated with long-term neurological sequelae."
29/
Endemic doesn't mean "good." It just means "now we're stuck with it."
Just sit there and stew in that for a minute: "an endemic disease associated with long-term neurological sequelae."
You can ignore it, but it doesn't give a shit what you think! You're just an incubator.
30/
Just sit there and stew in that for a minute: "an endemic disease associated with long-term neurological sequelae."
You can ignore it, but it doesn't give a shit what you think! You're just an incubator.
30/
This paper, however, is pretty damn solid! It really ties a LOT of different lines of research together.
Published today (July 28, 2024) in IJMS, open access:
31/31mdpi.com/1422-0067/25/1…
Published today (July 28, 2024) in IJMS, open access:
31/31mdpi.com/1422-0067/25/1…
Even if you're specifically familiar with it in the context of SIRS, it doesn't change the fact that "viremia" literally means, BY DEFINITION, "presence of viruses in the blood."
Your "correction" is 45 years out of date.
32/31
meshb.nlm.nih.gov/record/ui?ui=D…
Your "correction" is 45 years out of date.
32/31
meshb.nlm.nih.gov/record/ui?ui=D…
https://x.com/wecarryon2/status/1817872495313400314


Believe me, I went deep on looking for flaws in this one! My day yesterday was just picking apart this paper and cross-referencing every claim that seemed too convenient or tidy. Unfortunately, they did their due diligence and it's pretty solid!
33/31
33/31
https://x.com/BoldsHeidi/status/1817981939250511907
Moreover, there's not really anything new about this study *methodologically*!
When the references are solid, the stats are solid, and the method is basically just "we followed manufacturer instructions for this protocol x10," there's not much else to poke at for flaws!
34/31
When the references are solid, the stats are solid, and the method is basically just "we followed manufacturer instructions for this protocol x10," there's not much else to poke at for flaws!
34/31
Yup, it's EXACTLY why!
Anosmia is frequently a result of damage to the olfactory nerve:
And several issues people have in LC (including with chewing!) also aligns with the trigeminal nerve:
35/31
ncbi.nlm.nih.gov/books/NBK55605…
ncbi.nlm.nih.gov/books/NBK48228…
Anosmia is frequently a result of damage to the olfactory nerve:
And several issues people have in LC (including with chewing!) also aligns with the trigeminal nerve:
35/31
ncbi.nlm.nih.gov/books/NBK55605…
ncbi.nlm.nih.gov/books/NBK48228…
https://x.com/MrJFix3/status/1817954175184937438


Oh, yeah... wasn't there some quack on here a few days ago who was saying there's no "disease mechanism" that could explain why chewing is difficult in LC?
It must be humiliating to be a doctor and not be familiar with the concept of trigeminal nerve dysfunction!
36/31
It must be humiliating to be a doctor and not be familiar with the concept of trigeminal nerve dysfunction!
36/31

Here is the entire thread about "SARS-CoV-2 Rapidly Infects Peripheral Sensory and Autonomic Neurons, Contributing to Central Nervous System Neuroinvasion before Viremia" on a single page: readwise.io/reader/shared/…
• • •
Missing some Tweet in this thread? You can try to
force a refresh


![CONSTITUTION OF THE WHO […] Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition. The health of all peoples is fundamental to the attainment of peace and security and is dependent upon the fullest co-operation of individuals and States. Informed opinion and active co-operation on the part of the public are of the utmost impor...](https://pbs.twimg.com/media/HEYSQdLW0AAomwA.png)


![“8. Performance of Nuclear Power Plants Affected by the Blackout On August 14, 2003, nine U.S. nuclear power plants experienced rapid shutdowns (reactor trips) as a consequence of the power outage. Seven nuclear power plants in Canada operating at high power levels at the time of the event also experienced rapid shutdowns. […]. Many non-nuclear generating plants in both countries also tripped during the event. Numerous other nuclear plants observed disturbances on the electrical grid but continued to generate electrical power without interruption. […] - The severity of the grid transient...](https://pbs.twimg.com/media/G0Q9wDEXkAAknYM.jpg)








