
THIS IS BIG. WOW. New paper in PLOS Pathogens has findings about:
- the effect of the SARS-CoV-2 spike protein on cardiac cells (and mitochondrial dysfunction!),
- a treatment to be investigated, and
- how this is NOT caused by mRNA vaccines!
Buckle up, we're diving in...
1/![Published August 5, 2024 in PLOS Pathogens: "SARS-CoV-2 spike-induced syncytia are senescent and contribute to exacerbated heart failure" "Author Summary In this paper, we directly linked SARS-2-S-triggered syncytium [fused cells] formation in the absence of infection with the ensuing induction of cellular senescence and its pathophysiological contribution to heart failure. We propose that both SARS-2-S expression and SARS-2-S protein internalization were sufficient to induce senescence in nonsenescent ACE2expressing cells. This is important because of the persistent existe...](/images/1px.png)
- the effect of the SARS-CoV-2 spike protein on cardiac cells (and mitochondrial dysfunction!),
- a treatment to be investigated, and
- how this is NOT caused by mRNA vaccines!
Buckle up, we're diving in...
1/
![Published August 5, 2024 in PLOS Pathogens: "SARS-CoV-2 spike-induced syncytia are senescent and contribute to exacerbated heart failure" "Author Summary In this paper, we directly linked SARS-2-S-triggered syncytium [fused cells] formation in the absence of infection with the ensuing induction of cellular senescence and its pathophysiological contribution to heart failure. We propose that both SARS-2-S expression and SARS-2-S protein internalization were sufficient to induce senescence in nonsenescent ACE2expressing cells. This is important because of the persistent existe...](https://pbs.twimg.com/media/GURP49TW0AAb71d.jpg)
[This paper is an uncorrected proof; it's been peer-reviewed, but not copyedited yet.]
A bit of background: syncytia (sin-sih-sha) are giant cells with multiple nuclei that form from the fusion of multiple cells. Viral infections are a common cause of syncytia.
2/
A bit of background: syncytia (sin-sih-sha) are giant cells with multiple nuclei that form from the fusion of multiple cells. Viral infections are a common cause of syncytia.
2/


The authors had two motivations for this study:
1. Cardiac complications are a major feature of COVID.
2. Patients with heart failure tend to experience very poor outcomes from COVID.
Really, it hasn't been entirely clear *how* COVID leads to heart failure... until now?
3/
1. Cardiac complications are a major feature of COVID.
2. Patients with heart failure tend to experience very poor outcomes from COVID.
Really, it hasn't been entirely clear *how* COVID leads to heart failure... until now?
3/
!["Introduction ...Although symptoms resulting from infection typically resolve within weeks, some individuals experience persistent symptoms following the acute phase of COVID-19, the so-called post-acute sequelae of COVID-19 (PASC) or long COVID [2–4]. SARS-CoV-2 infection predominantly offends the respiratory system. Currently, evidence has suggested cardiac complications as one of the important pathogenic features of COVID-19 [5,6]. More importantly, compared with patients without heart failure, those with diagnosed heart failure experienced a longer length of hospital stay, increas...](https://pbs.twimg.com/media/GURP9_CWQAA3NX-.jpg)
Syncytia form when the spike protein present on the surface of one cell makes contact with another cell.
This study went a step further by looking at how *extracellular* vesicles containing the spike protein can fuse cells... *without* active infection.
4/
This study went a step further by looking at how *extracellular* vesicles containing the spike protein can fuse cells... *without* active infection.
4/
!["SARS-CoV-2 syncytium constitutes a hallmark of COVID-19-associated pathology and may potentially contribute to pathology by facilitating viral dissemination, cytopathy, immune evasion, and the inflammatory response [12]. ... In addition to mediate viral-cell fusion, the presence of SARS-2-S on the cell surface is sufficient to mediate cell-cell fusion, a mechanism called fusion from within (FFWI)[14,15]. The fusogenic activity of SARS-2-S is potent, as even undetectable amounts of SARS-2-S can cause cell-cell fusion [14]. In addition to mediating FFWI, viruslike particles or lipid ves...](https://pbs.twimg.com/media/GURP_YMXkAAnRtS.jpg)
Why do syncytia matter?
They're a potential route for the spike protein to cause damage even AFTER an active infection has subsided.
Like some other viruses, SARS-CoV-2 can cause cell senescence—which is when the cell replication cycle stops, and the cells degrades.
5/
They're a potential route for the spike protein to cause damage even AFTER an active infection has subsided.
Like some other viruses, SARS-CoV-2 can cause cell senescence—which is when the cell replication cycle stops, and the cells degrades.
5/

So before we dive into results, what is the headline?
Although cytokine storm has long been thought the cause of COVID-related cardiac issues, this study found that the SARS-CoV-2 spike protein "led to profound cardiac fibrosis without affecting baseline cariac function."
6/
Although cytokine storm has long been thought the cause of COVID-related cardiac issues, this study found that the SARS-CoV-2 spike protein "led to profound cardiac fibrosis without affecting baseline cariac function."
6/

Moreover, they found a drug target that may be able to prevent "the downregulation of mitochondrial metabolism," and it has shown potential promise in treating heart failure overall.
It would treat the "increased risk of developing heart failure and sudden cardiac death"!
7/
It would treat the "increased risk of developing heart failure and sudden cardiac death"!
7/
!["Previous studies have shown that small-molecule inhibition of WNK1 prevents the downregulation of mitochondrial metabolism and improves RV function and survival in pulmonary arterial hypertension. We found that WNK1 inhibition alleviated SARS-2-Saggravated heart failure and reduced serum cTnT and IL-1ß levels. cTnT is released into circulation during injury to cardiac myocytes(51]. Individuals with higher cTnT levels are at an increased risk of developing heart failure and sudden cardiac death. Therefore, through its metabolism-rescue and anti-inflammatory properties, WNK463 may have ...](https://pbs.twimg.com/media/GURQD7ZW4AAdheV.jpg)
Let's dive in to the results! I'm going to jump around a bit, because this paper is EXTENSIVE.
First up, when they cultured cells expressing the spike (S) protein and the ACE2 receptor in a 1:1 ratio, the cells started fusing within four hours. Basic premise confirmed!
8/
First up, when they cultured cells expressing the spike (S) protein and the ACE2 receptor in a 1:1 ratio, the cells started fusing within four hours. Basic premise confirmed!
8/

In the cultures with SARS-2-S syncytia, the cells secreted more senescence-related cytokines, including IL-6, IL-8, and IL-2, compared to the cells exposed to a mutant spike protein that can't cause senesense!
They found similar syncytia formation in other cell types.
9/
They found similar syncytia formation in other cell types.
9/

They also tested the spike from four Omicron variants (BA.1, BA.5, BA.2.75, BA.2.75.2). Previous work has found BA.1 has a 5x reduction in ability to fuse cells (compared to wild-type), but the others have a 1.2-1.7x reduction.
All formed syncytia, just a bit more slowly.
10/
All formed syncytia, just a bit more slowly.
10/
!["We next compared the senescence potential of four Omicron variants, SARS-2-SBA.1 , SARS-2-SBA.5 , SARS-2-SBA.2.75 , and SARS-2-SBA.2.75.2 , with that of SARS-2-S (S1C Fig). As reported, the Omicron BA.1 variant showed significantly weaker fusogenic activity than SARS-2-S [26] (5× reduction). The fusogenic capacity of BA.5 (1.2× reduction), BA.2.75 (1.7× reduction), and BA.2.75.2 (1.7× reduction) was modestly lower than that of SARS-2-S [27,28]. Notably, the percentage of SA-β-gal-positive syncytia was comparable to that of SARS-2-S, although they formed more slowly (Fig 1F and 1G). .....](https://pbs.twimg.com/media/GURQH9SWoAAwhah.jpg)
Here's where it gets REALLY concerning: Extracellular vesicles—little packets, emitted by cells, containing a protein or some other type of small molecule—have been found carrying the S protein in patients' blood long after initial infection...
11/
11/
!["SARS-2-S delivery by EVs or mRNA confers the ability to trigger syncytial senescence Since SARS-2-S was shown to be incorporated into extracellular vesicles circulating in patient blood [29], we then asked if SARS-2-S protein internalization by S-EVs has the ability to trigger syncytium formation and cell senescence in an FFWO-dependent manner. To this end, we first used ultracentrifugation to purify EVs from the supernatant of HeLa- or SARS-2-Sexpressing HeLa cells and confirmed their identity by probing for exosome markers and the EVs were normalized by NTA (S2A-S2C Fig). We next l...](https://pbs.twimg.com/media/GURQJTBW8AEnnOS.jpg)
...and they found that these extracellular vesicles, once taken up by a cell, can cause the cell to fuse to another ACE2-expressing cell.
The fused cells then showed signs of senescence (including increased transcription of TNF, IL6, IL8, and CDKN1A genes).
Not great!
12/
The fused cells then showed signs of senescence (including increased transcription of TNF, IL6, IL8, and CDKN1A genes).
Not great!
12/

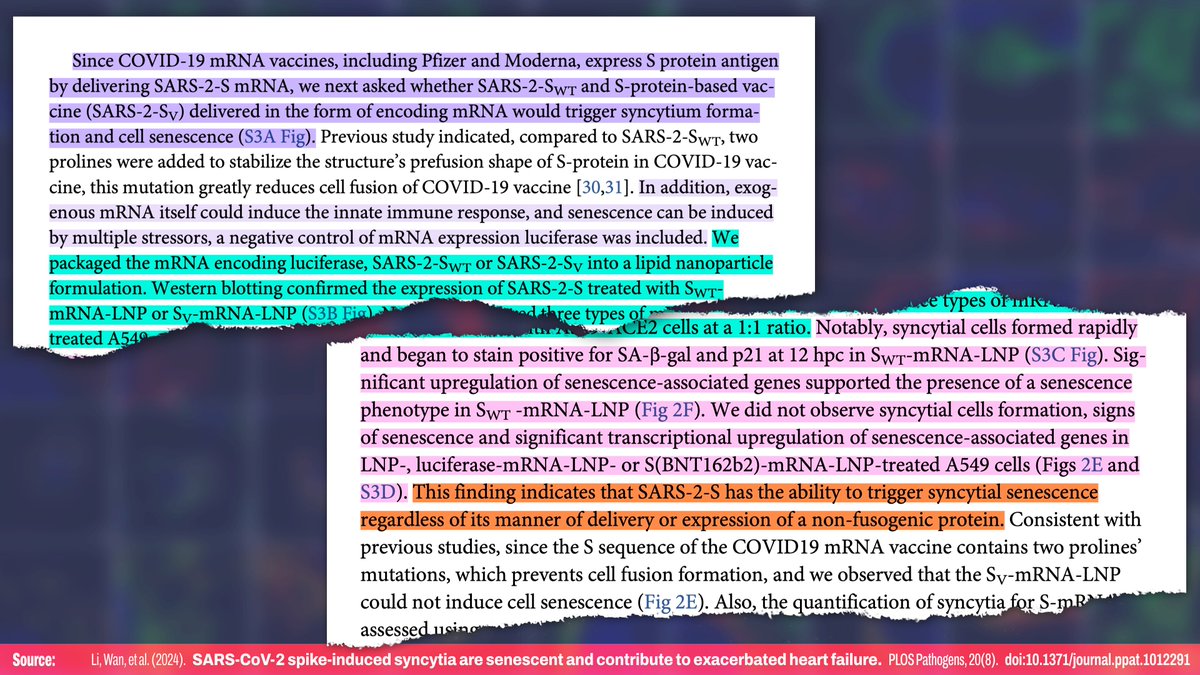
What about the mRNA vaccines—they produce a spike protein, so can they also cause this problem? Nope!
The spike design used in the vaccines has a couple of tweaks to make it more stable, and those changes prevent it the vaccine-based spike protein from causing cell fusion!
13/
The spike design used in the vaccines has a couple of tweaks to make it more stable, and those changes prevent it the vaccine-based spike protein from causing cell fusion!
13/
To be really sure that the S protein can cause this type of syncytial senescence to occur in real organs, they injected mice with a virus that causes them to express human ACE2 in their livers.
When injected with the wild S protein, it induced senescence in their livers!
14/
When injected with the wild S protein, it induced senescence in their livers!
14/
!["Finally, we explored whether cell senescence related to SARS-2-S-mediated cell fusion would also occur in vivo. To this end, we injected AAV-hACE2 constructs into the tail veins of 8-week-old C57BL/6] mice to drive mainly hepatic hACE2 expression. Four weeks later, we intramuscularly administered a single dose of S-mRNA-LNP or LNP to hACE2-expressing mice and examined the induction of senescence. Immunohistochemical analysis revealed robust SARS-2-S expression and the increased appearance of multinucleated cells with at least four nuclei in the livers of S-mRNA-LNP-treated mice compar...](https://pbs.twimg.com/media/GURQNbAXEAAKixf.jpg)
Next up, they looked at mitochondrial regulation.
Long story story, MAVS (mitochondrial antiviral signaling) proteins, which detect foreign double-stranded RNA, cause mitochondrial senescence in response to the SARS-2-S syncytia.
15/
Long story story, MAVS (mitochondrial antiviral signaling) proteins, which detect foreign double-stranded RNA, cause mitochondrial senescence in response to the SARS-2-S syncytia.
15/
!["These data suggest the involvement of RIG-I, the primary sensor of nonself-derived dsRNA [this means it detects double-stranded RNA of a foreign-source (e.g. from a virus)], in functional MAVS aggregation in SARS-2-S syncytia." --- "SARS-2-S syncytia provoke the formation of functional MAVS aggregates ...We then focused on mitochondrial antiviral signalling adaptor protein (MAVS), a mitochondrial adaptor protein that links the cytoplasmic RNA sensor RIG-I to its downstream signalling molecules by forming well-ordered prion-like aggregates. .... Furthermore, MAVS aggregat...](https://pbs.twimg.com/media/GURQO2OWcAAdH7U.jpg)

Jumping ahead a bit, they found that "senescent SARS-2-S syncytia exhibit [shrunken] morphology, leading to the activation of WNK1," which is a molecule involved in regulating cell senesence.
It is activated by the fused cells losing their volume.
16/
It is activated by the fused cells losing their volume.
16/
!["...Previous study indicated that with-no-lysine (WNK) kinasel is a molecular crowding sensor that undergoes cell shrinkage-dependent phase separation to restore cell volume, the shrinkage of senescent SARS-2-S syncytia made us wonder whether WNK1 was activated [41]. Notably, we observed a significant shift of WNK1 from a diffuse to punctate distribution in senescent SARS-2-S syncytia of A549 and AC16 cells (Fig 5E-5I), but not in those cells treated with palbociclib (Fig 5J-5M). This phase behaviour appeared as early as 12 hpc in AC16 cells (Fig 5E). Accordingly, WNK1-triggered SPAK p...](https://pbs.twimg.com/media/GURQRK_WQAAhe_5.jpg)
They found WNK1 activation led to significantly decreased "mitochondrial oxidative capacity of the cocultured cardiomyocyte"
But "inhibition of WNK1 via WNK463 [which prevents down-regulation of metabolic enzymes] was sufficient to rescue impaired mitochondrial respiration"
17/
But "inhibition of WNK1 via WNK463 [which prevents down-regulation of metabolic enzymes] was sufficient to rescue impaired mitochondrial respiration"
17/
!["So, we try to study energy metabolism of cardiomyocytes syncytia whether dependent on WNK1 activation [42,43]. We next explored the possibility that senescent SARS-2-S syncytia in cardiomyocytes with WNK1 activation might contribute to impaired metabolism in the setting of heart dysfunction. Compared to non-fusion controls, the mitochondrial oxidative capacity of the cocultured cardiomyocytes was significantly decreased at 48 hpc as indicated by reduced basal respiration, ATP-linked respiration, spare respiratory, and maximal respiration (Fig 6A and 6B). In addition, these senescent c...](https://pbs.twimg.com/media/GURQSd-WsAAOzUW.jpg)
Jumping ahead again, we're getting to the headline experiments.
They administered the SARS-2-S protein to some mice that express the human ACE2 receptor, and syncytia formed, as expected.
18/
They administered the SARS-2-S protein to some mice that express the human ACE2 receptor, and syncytia formed, as expected.
18/

They concluded that "SARS-2-S promotes fibrosis without causing baseline cardiac abnormalities," and in the mice with pre-existing heart failure, it "exacerbated heart failure progression"
"fibrosis without causing baseline cardiac abnormalities"... not great!
19/
"fibrosis without causing baseline cardiac abnormalities"... not great!
19/

Finally, they examined if WNK1 inhibition can "alleviate heart failure exacerbated by SARS-2-S through rescuing metabolic dysfunction." They found positive results, "further supporting the notion that senescent SARS-2-S syncytia contribute to exacerbated heart failure."
20/
20/

What do they conclude?
The S protein can contribute to heart failure. This is important for acute infections AND long-term complications, because the "persistence of circulating SARS-2-S protein ... increase the likelihood of cell-cell fusion in uninfected cells."
21/
The S protein can contribute to heart failure. This is important for acute infections AND long-term complications, because the "persistence of circulating SARS-2-S protein ... increase the likelihood of cell-cell fusion in uninfected cells."
21/

They also note that syncytia expressed senescence-related cytokines, including TNF-alpha, IL-6, and IFN-gamma, among others, and these seem related to the metabolic regulation.
22/
22/

And, importantly, the mRNA vaccines CANNOT cause cellular senescence using this mechanism, as they have a couple of mutations which "effectively inhibit the formation of syncytia, mitigate cellular senescence, and prevent the release of" senescence-relate signals.
23/
23/

Because patients with heart failure show elevated ACE2 expression, while those with Long COVID exhibit "persistent circulating SARS-2-S and EVs harboring SARS-2-S," this combination "may increase the likelihood of syncytium formation."
24/
24/

This is very much a basic research paper and doesn't have anything directly *usable* in clinical practice. However, it really illuminates the pathophysiology of cardiac complications of SARS-CoV-2 infection—EVEN ASYMPTOMATIC INFECTIONS.
Paper:
25/25journals.plos.org/plospathogens/…
Paper:
25/25journals.plos.org/plospathogens/…
AFAIK, it’s totally a non-issue with the non-mRNA vaccines, because they don’t even have a full spike protein.
And I think their statements about how mRNA vaccines with a different design could have more complications was a veiled reference to one of China’s vaccines
26/25
And I think their statements about how mRNA vaccines with a different design could have more complications was a veiled reference to one of China’s vaccines
26/25
https://twitter.com/deejaysas/status/1820716926995161100
No idea what to do about denialism at this point, other than continuing to educate and hope it gets through!
That's the goal with my threads: Hopefully, they can help give people the knowledge and language they need to discuss the science directly!
27/25
That's the goal with my threads: Hopefully, they can help give people the knowledge and language they need to discuss the science directly!
27/25
https://x.com/DiaBraveSid/status/1820832641236570541
At this point, it's a *potential* treatment that still needs further study, but it's a solid lead!
- Inhibiting the *WNK1 molecule* with a *WNK463 molecule* is the new option uncovered here
- Two existing preventative drugs should be investigated
28/25
- Inhibiting the *WNK1 molecule* with a *WNK463 molecule* is the new option uncovered here
- Two existing preventative drugs should be investigated
28/25
https://x.com/sarahga89137569/status/1820838220420038840

Glad you asked, because I was conflating previous vector vaccines with ones under development!
It seems that Novavax and Janssen use the same STABILIZED spike protein as Pfizer and Moderna:
But oddly enough...
29/25
pubs.acs.org/doi/10.1021/ac…
It seems that Novavax and Janssen use the same STABILIZED spike protein as Pfizer and Moderna:
But oddly enough...
29/25
pubs.acs.org/doi/10.1021/ac…
https://x.com/fagiolinux/status/1820901632516731204

...it seems that a bunch of Russian viral vector vaccines—and AstraZeneca—used the regular spike protein!?
So that kind of explains the issues with the AstraZeneca vaccine! Weird.
30/25 ncbi.nlm.nih.gov/pmc/articles/P…
So that kind of explains the issues with the AstraZeneca vaccine! Weird.
30/25 ncbi.nlm.nih.gov/pmc/articles/P…


• • •
Missing some Tweet in this thread? You can try to
force a refresh









![Published July 28, 2024 in IJMS: "SARS-CoV-2 Rapidly Infects Peripheral Sensory and Autonomic Neurons, Contributing to Central Nervous System Neuroinvasion before Viremia" Abstract: "...little attention has been paid to susceptibility of the PNS to infection [by SARS-CoV-2] or to its contribution to CNS invasion. Here we show that sensory and autonomic neurons in the PNS are susceptible to productive infection with SARS-CoV-2 and outline physiological and molecular mechanisms mediating neuroinvasion. Our infection of K18-hACE2 mice, wild-type mice, and golden Syrian hamsters...](https://pbs.twimg.com/media/GTn4kqaWkAASZTk.jpg)
!["Up to 80% of people infected with SARS-CoV-2, the virus responsible for COVID-19, report neurological symptoms. ... including [with] sensory and autonomic systems [1–3]. Both central and peripheral symptoms, such as fatigue, memory issues, “brain fog”, hyper/hypoesthesia, and autonomic dysfunction, can persist as part of postCOVID-19 syndrome (“long COVID”) long after acute infection [4]. Detection of the virus, viral RNA, and antigens in the cerebrospinal fluid and brains of COVID-19 patients indicates SARS-CoV-2 is neuroinvasive, which has also been documented for common cold and ep...](https://pbs.twimg.com/media/GTn4uWGWkAANAnX.jpg)


![[Note: The 1st wave (Alpha) is referred to as D614G throughout the paper. The 4th wave (Omicron) is referred to as Omicron.] "This high-intensity sampling scheme allowed us to reconstruct the cohort participants’ SARS-CoV-2 infection histories with high fidelity, and to monitor infection-induced antibody responses over time. Blood samples collected immediately before Delta and Omicron waves offered a unique opportunity to investigate serum immune marker levels in close proximity to the next SARS-CoV-2 exposure. Furthermore, vaccine-derived immunity remained low at the onset of the Omi...](https://pbs.twimg.com/media/GTi4_X1XwAAzR1N.jpg)







