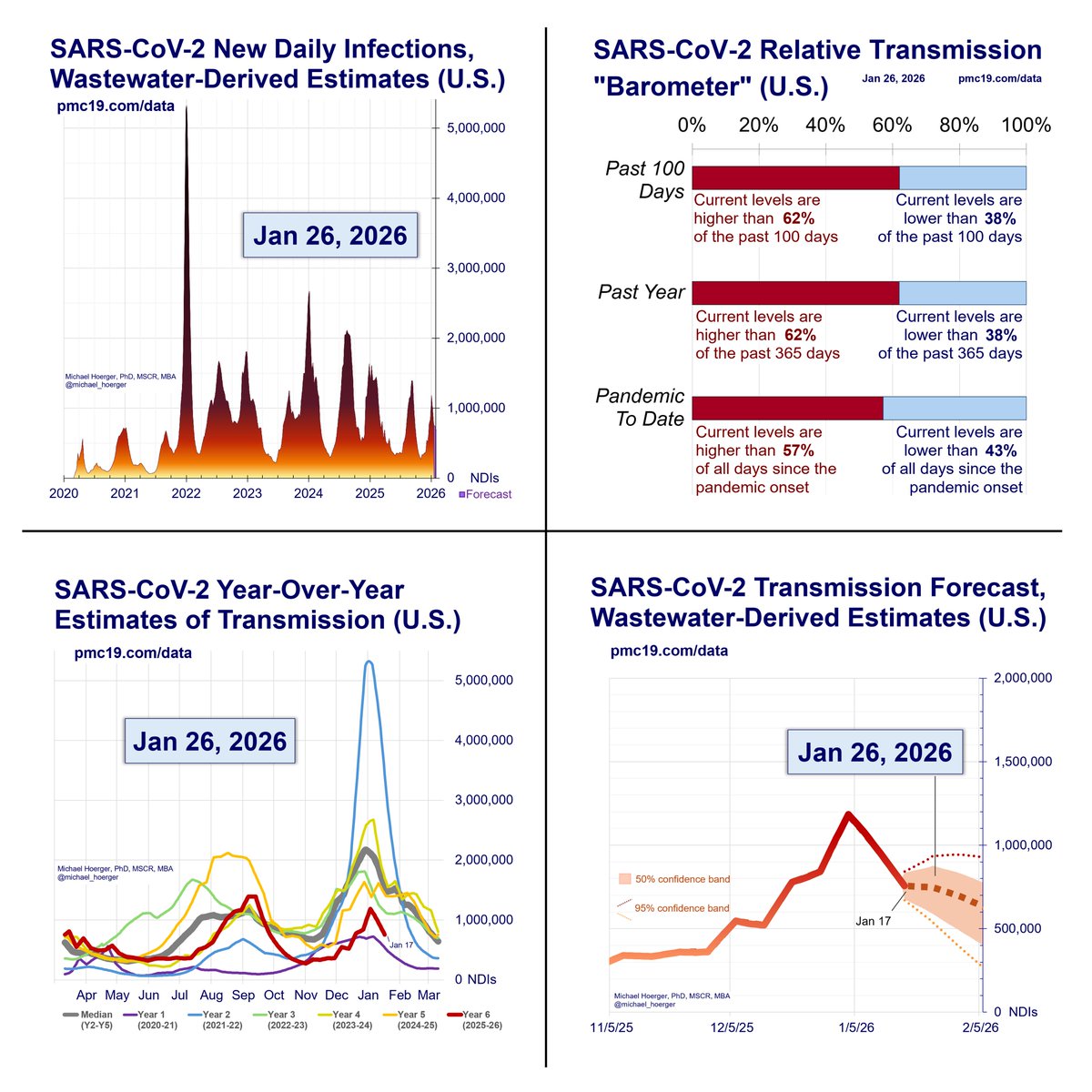
Just plugged today's CDC numbers into my new forecasting model (releases Mon). My initial reaction was "Jesus Christ. That's bad. That's really really bad."
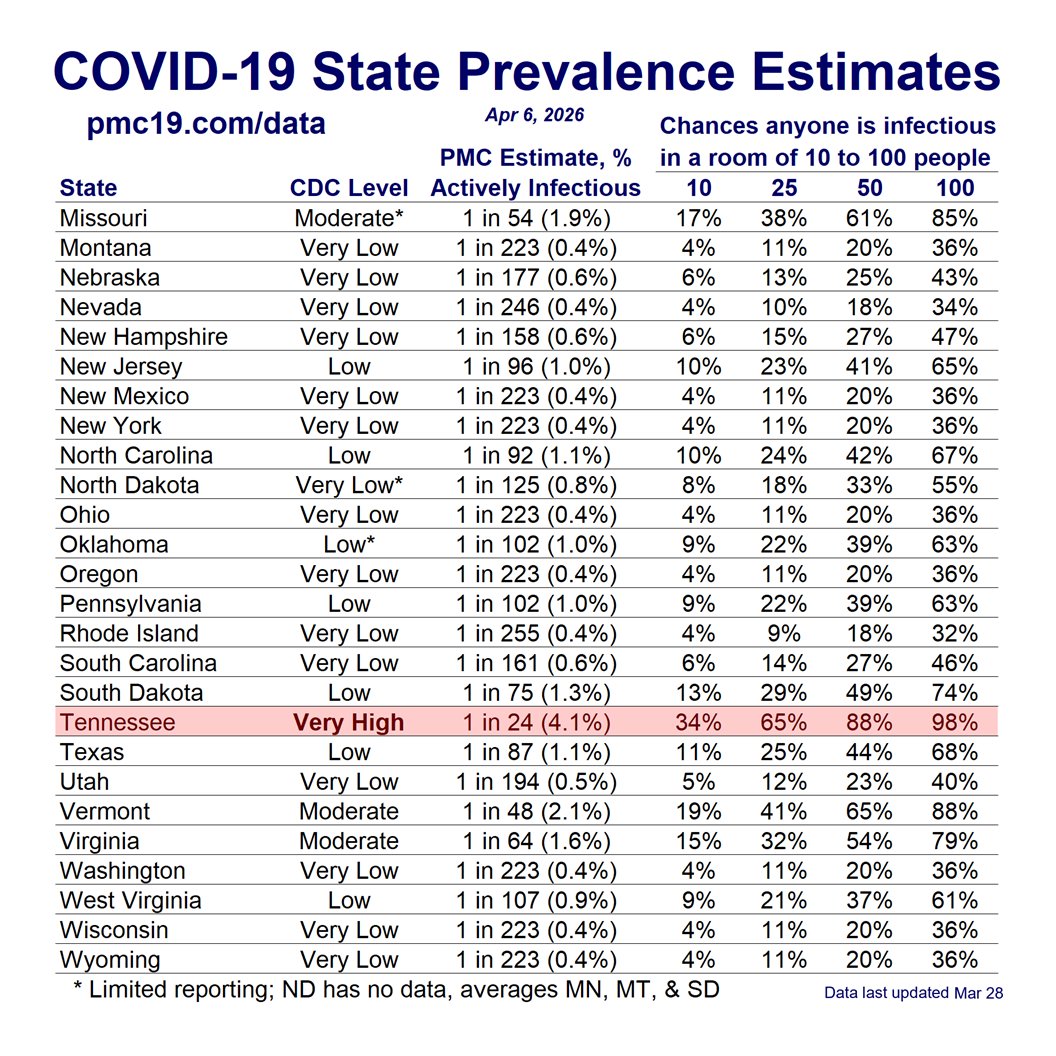
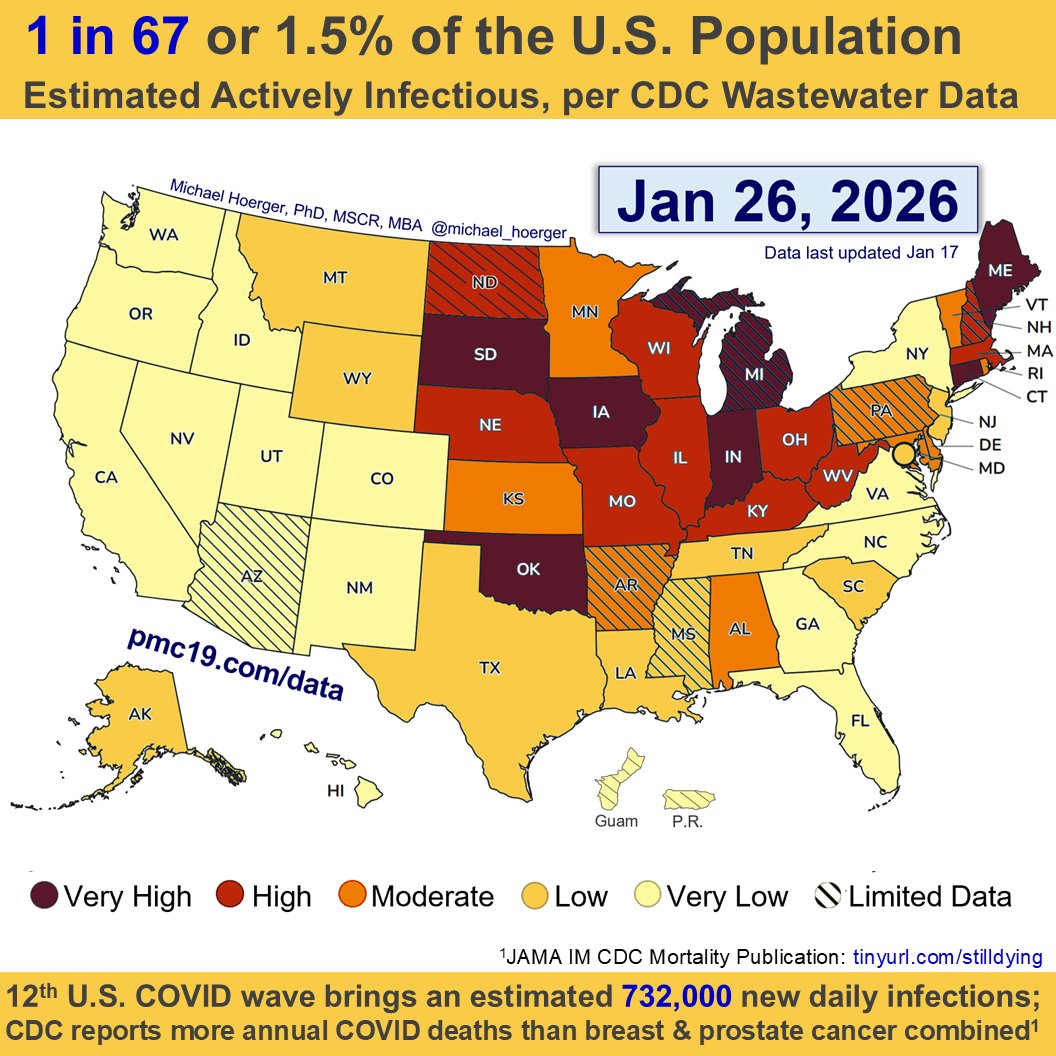
If you live in the West in particular, it's currently about as bad as last winter. About 1 in 23 infectious out West.
If you live in the West in particular, it's currently about as bad as last winter. About 1 in 23 infectious out West.

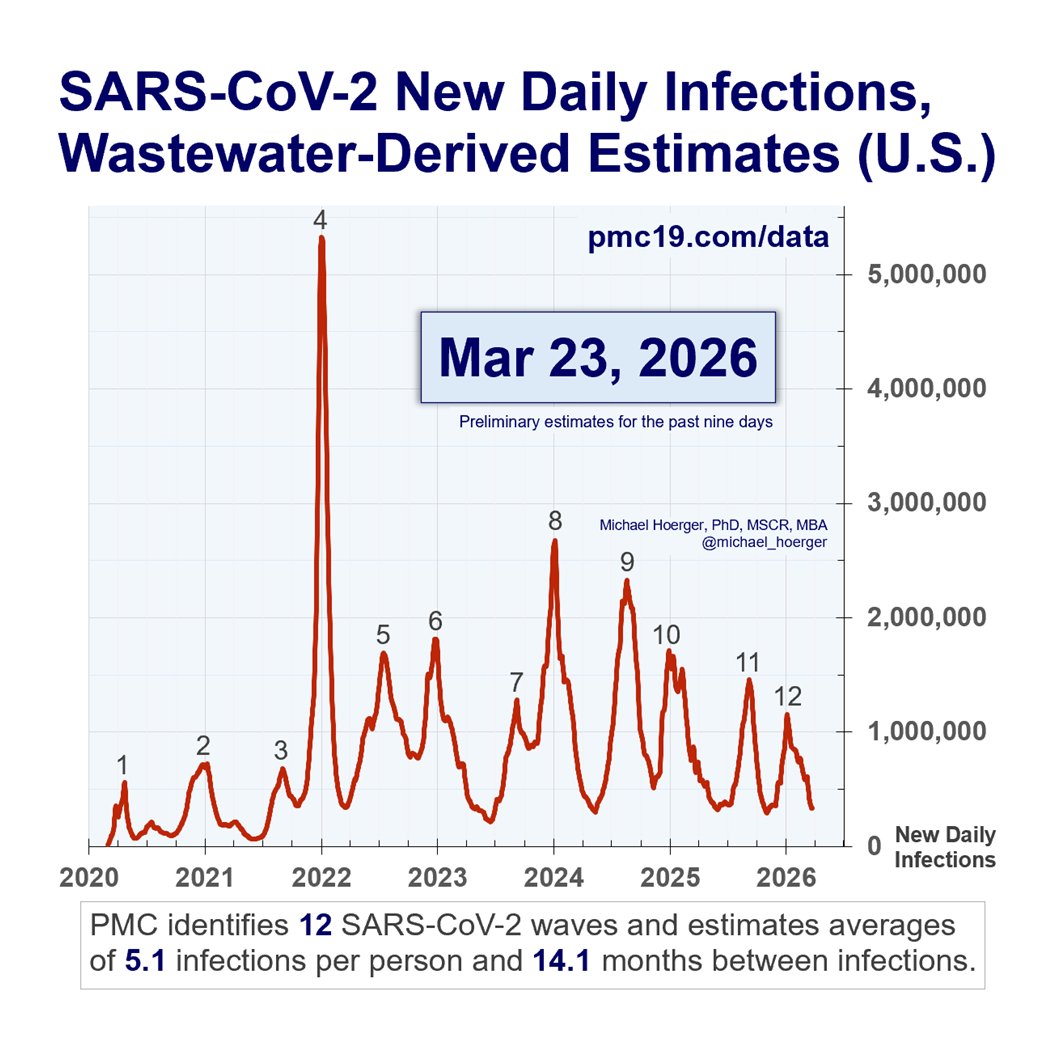
Those of us modeling have been talking about the late-summer wave -- all year -- as a given.
The 1-day isolation policy, the lack of a twice-annual updated vax, & the vilification of masks are emblematic of #LaissezFairePublicHealth. A wintery summer surge is the result.
The 1-day isolation policy, the lack of a twice-annual updated vax, & the vilification of masks are emblematic of #LaissezFairePublicHealth. A wintery summer surge is the result.
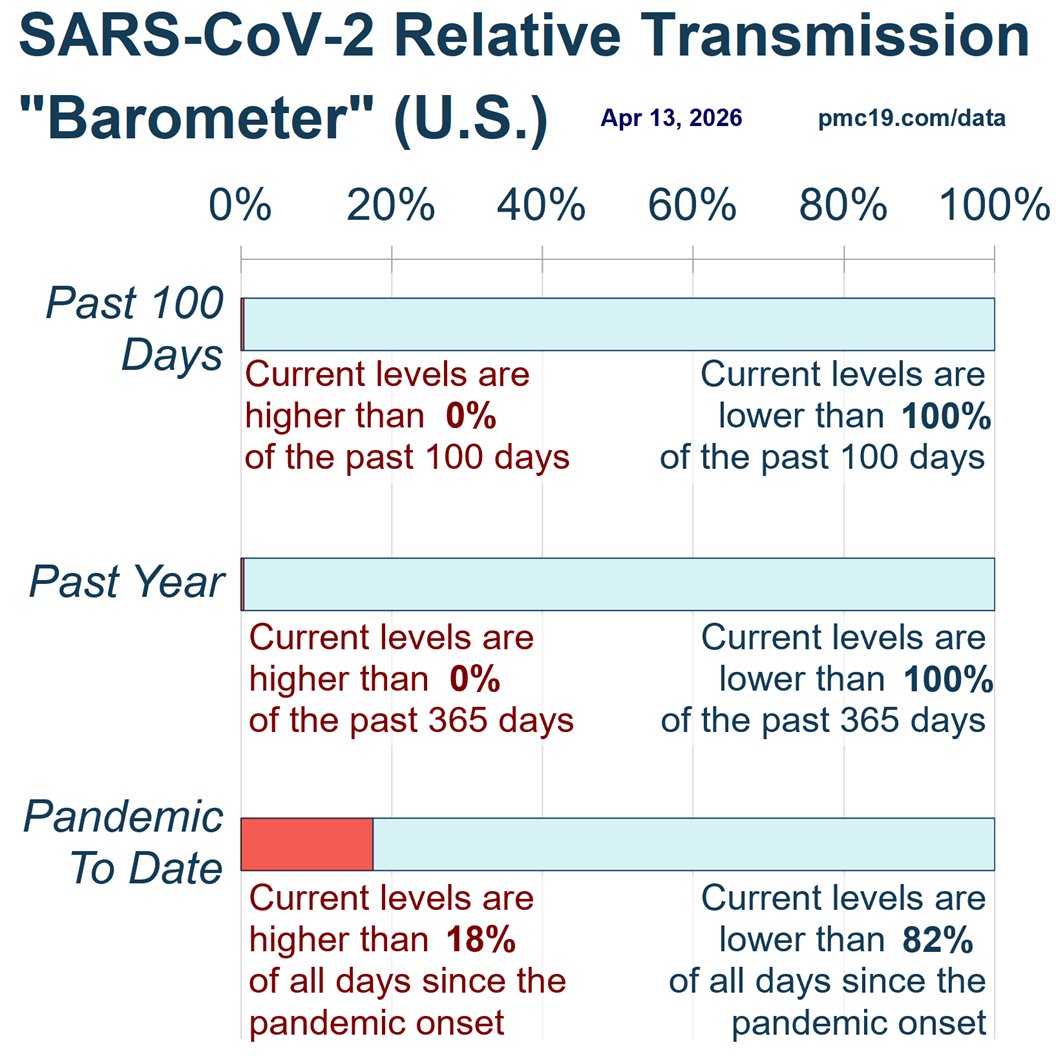
I hope the present numbers are revised downward, but there is no reason to suspect that. In my view, the current estimates are as likely to be overestimates as underestimates.
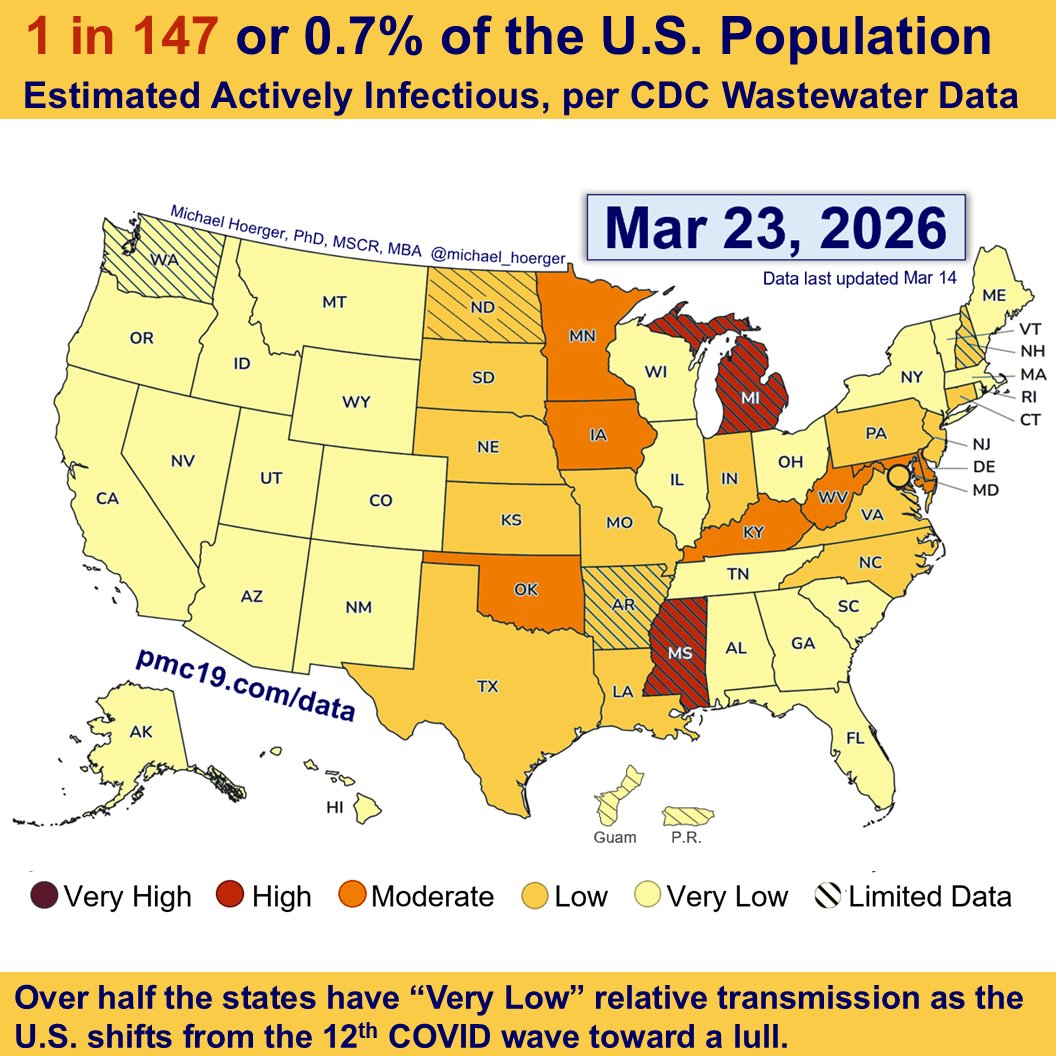
Here's the updated CDC COVID "heat" map released today, recolored with dark red to equal more transmission.

• • •
Missing some Tweet in this thread? You can try to
force a refresh