1/Do questions about brainstem anatomy cause you to suddenly get a case of locked in syndrome?!
Do you try to localize the lesion or just wait for the MR?
Wait no more!
Here’s a thread about the brainstem Rule of Four to help you localize brainstem lesions!
Do you try to localize the lesion or just wait for the MR?
Wait no more!
Here’s a thread about the brainstem Rule of Four to help you localize brainstem lesions!
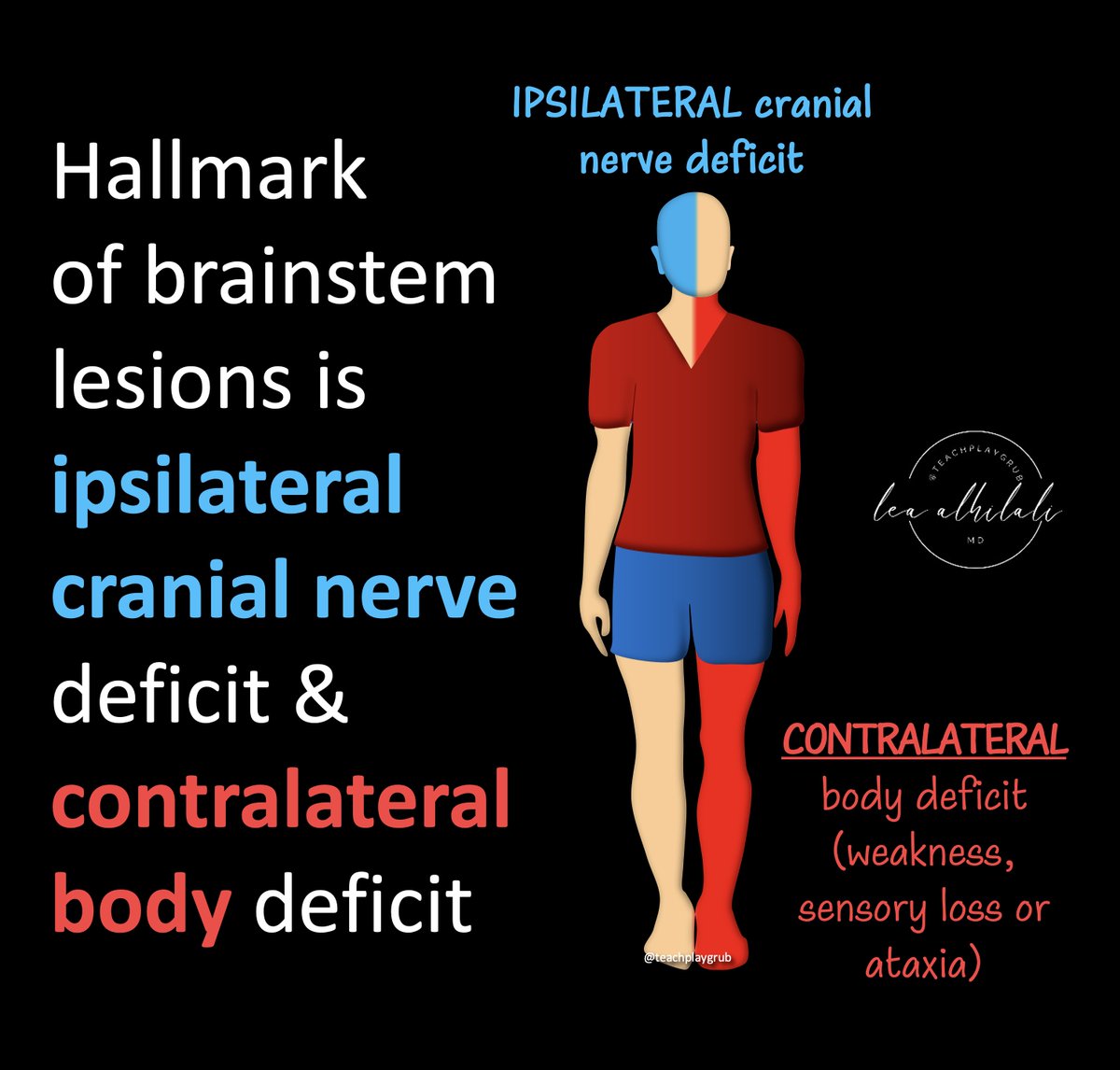
2/The hallmark of a brainstem lesion/syndrome is:
(1) Ipsilateral cranial nerve deficit
(2) Contralateral body deficit (be it weakness, sensory loss, or ataxia)
(1) Ipsilateral cranial nerve deficit
(2) Contralateral body deficit (be it weakness, sensory loss, or ataxia)
3/You can remember this because often your head has certain feelings that opposite the feelings in your heart/body.
Similarly, the cranial nerve deficit can be the opposite of the body deficit
This split between head and body is key for recognizing brainstem syndromes
Similarly, the cranial nerve deficit can be the opposite of the body deficit
This split between head and body is key for recognizing brainstem syndromes

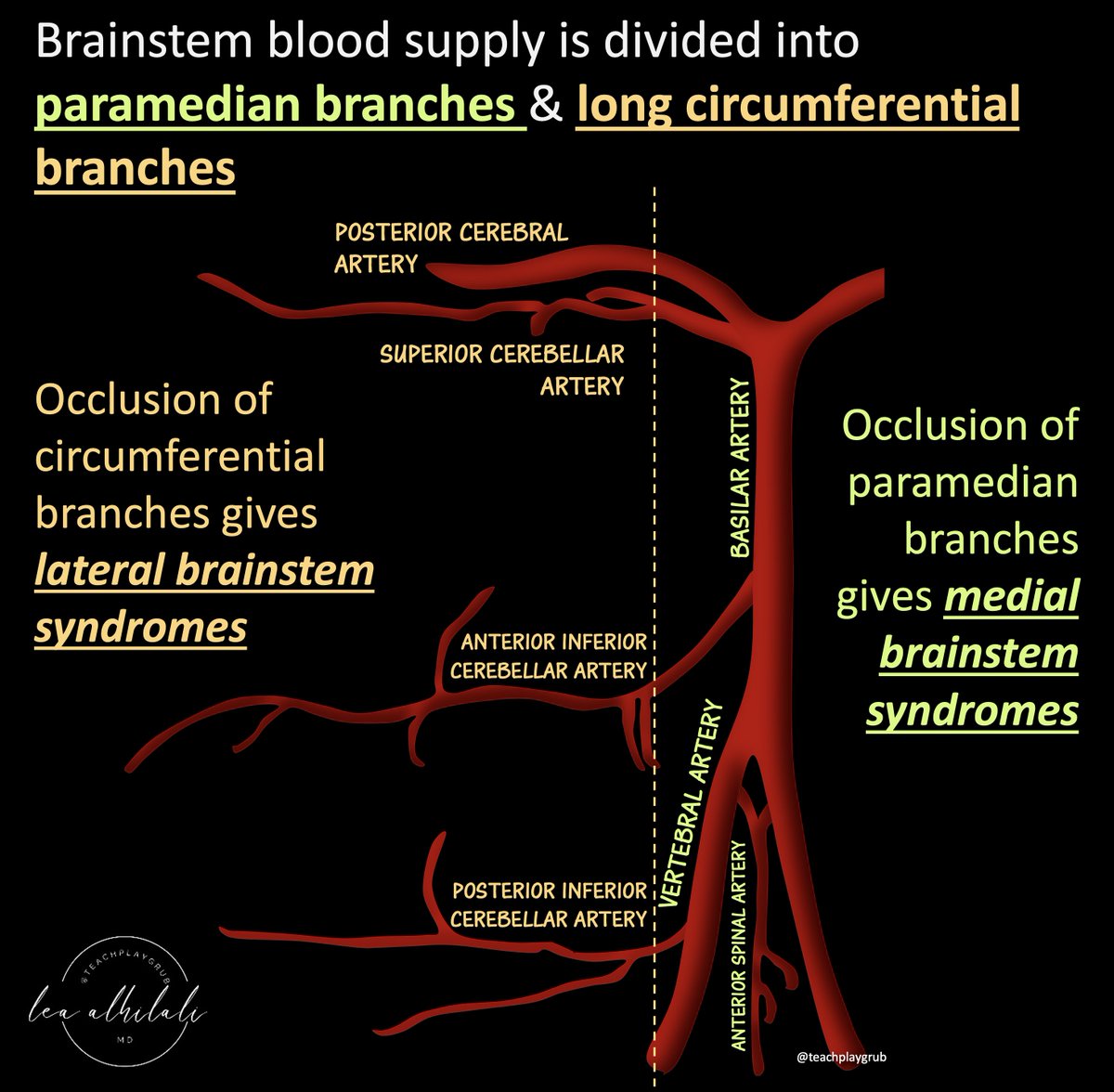
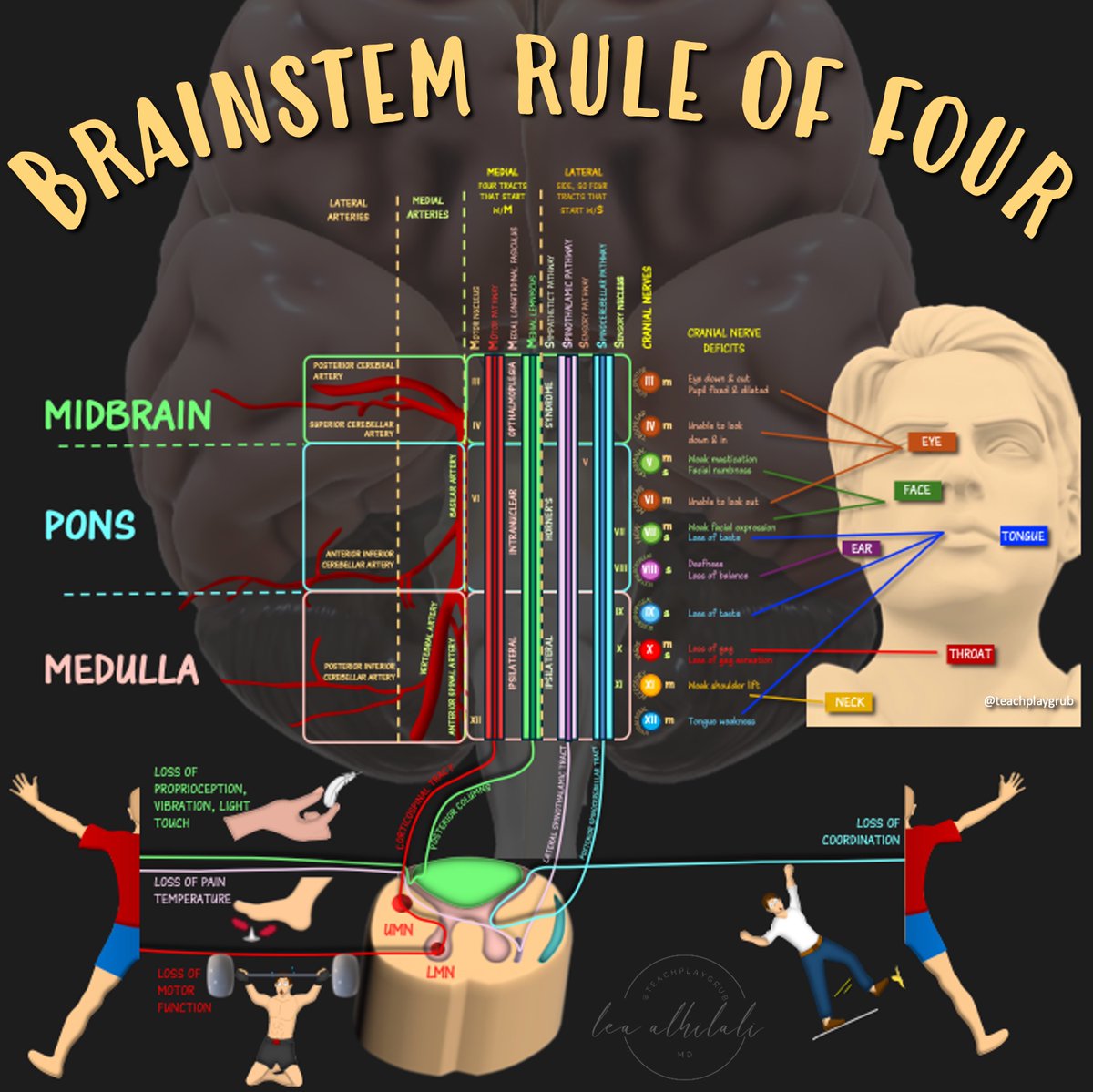
4/There is a medial & lateral organization to the brainstem blood supply.
Medially, there are paramedian vessels & laterally long circumferential branches
As a result of this design, you tend to get medial & lateral brainstem syndromes depending on where the occlusion is!
Medially, there are paramedian vessels & laterally long circumferential branches
As a result of this design, you tend to get medial & lateral brainstem syndromes depending on where the occlusion is!
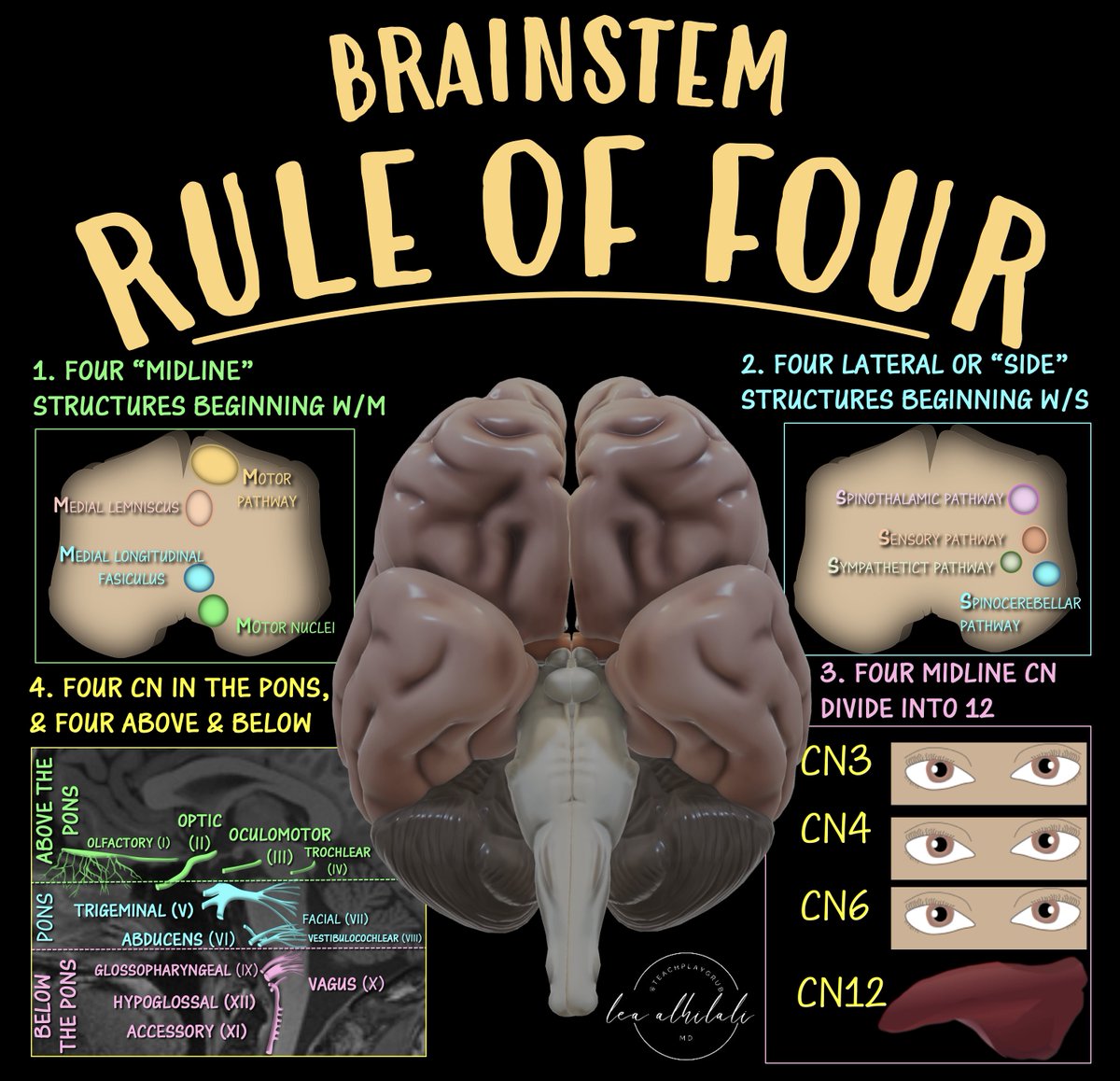
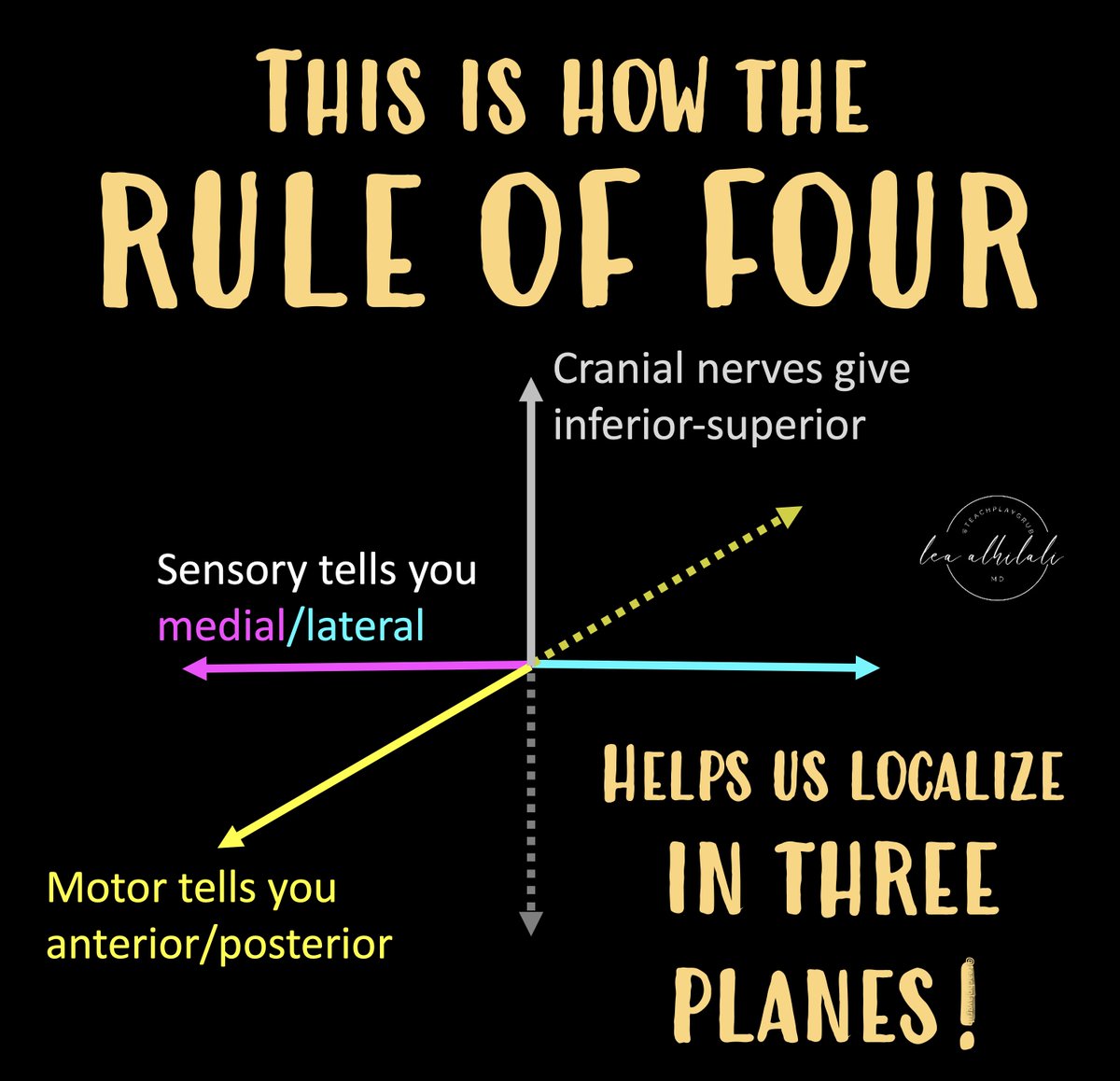
5/There are 4 rules of 4 to help us to localize brainstem lesions.
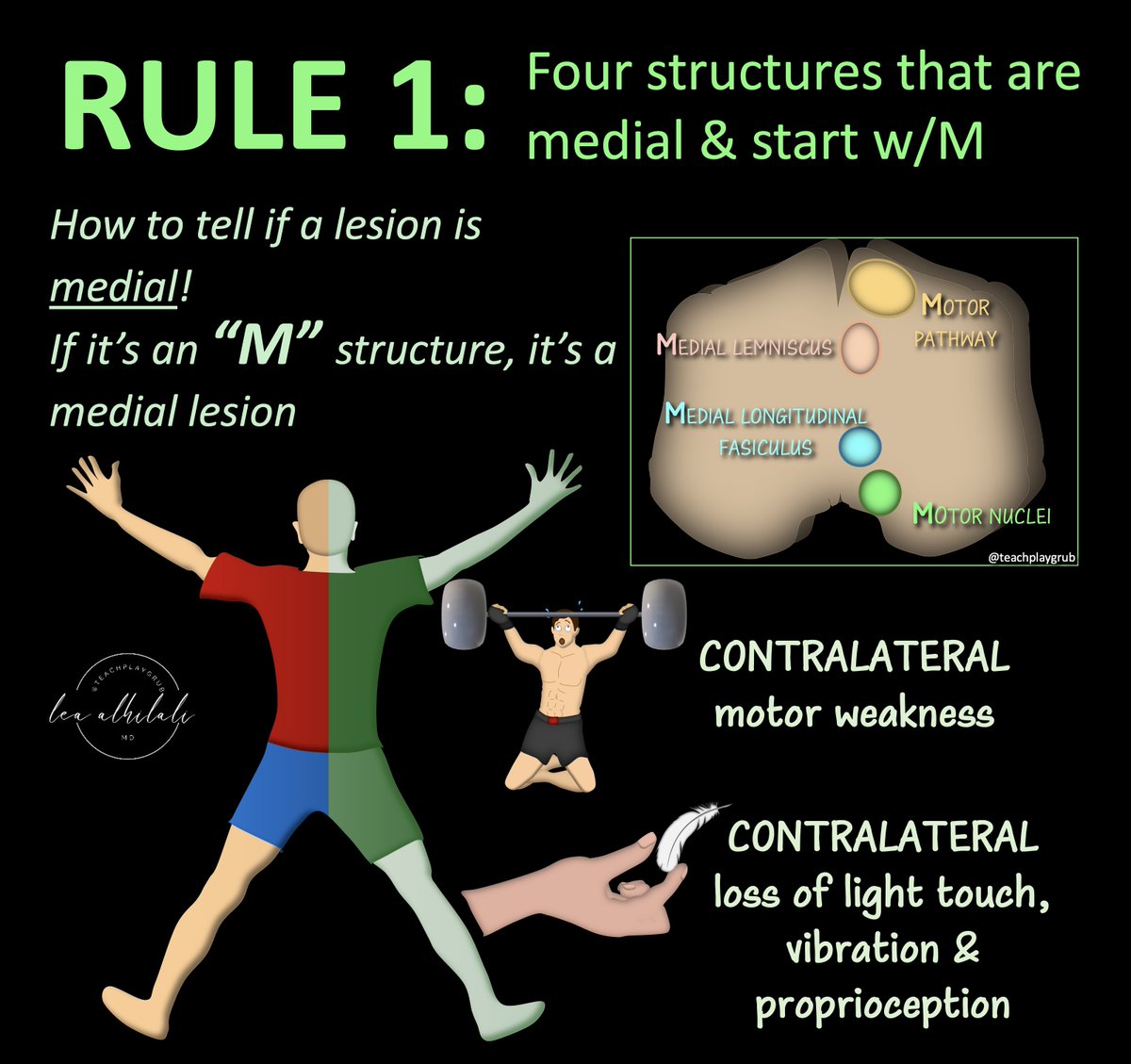
Rule 1: Four structures that are Medial that begin w/M
This helps us tell if the lesion is medial
It's medial if there's contralateral motor weakness or loss of light touch, vibration & proprioception
Rule 1: Four structures that are Medial that begin w/M
This helps us tell if the lesion is medial
It's medial if there's contralateral motor weakness or loss of light touch, vibration & proprioception
6/Rule 2: Fours structures on the Side that begin w/S
Involvement of these structures tells us that it is a lateral lesion
Results in contralateral loss of pain & temperature sensation
Involvement of these structures tells us that it is a lateral lesion
Results in contralateral loss of pain & temperature sensation

7/Motor is anterior.
Motor involvement tells you if the lesion is anterior or posterior.
So now we can localize not only medial & lateral, but anterior & posterior!
Motor involvement tells you if the lesion is anterior or posterior.
So now we can localize not only medial & lateral, but anterior & posterior!

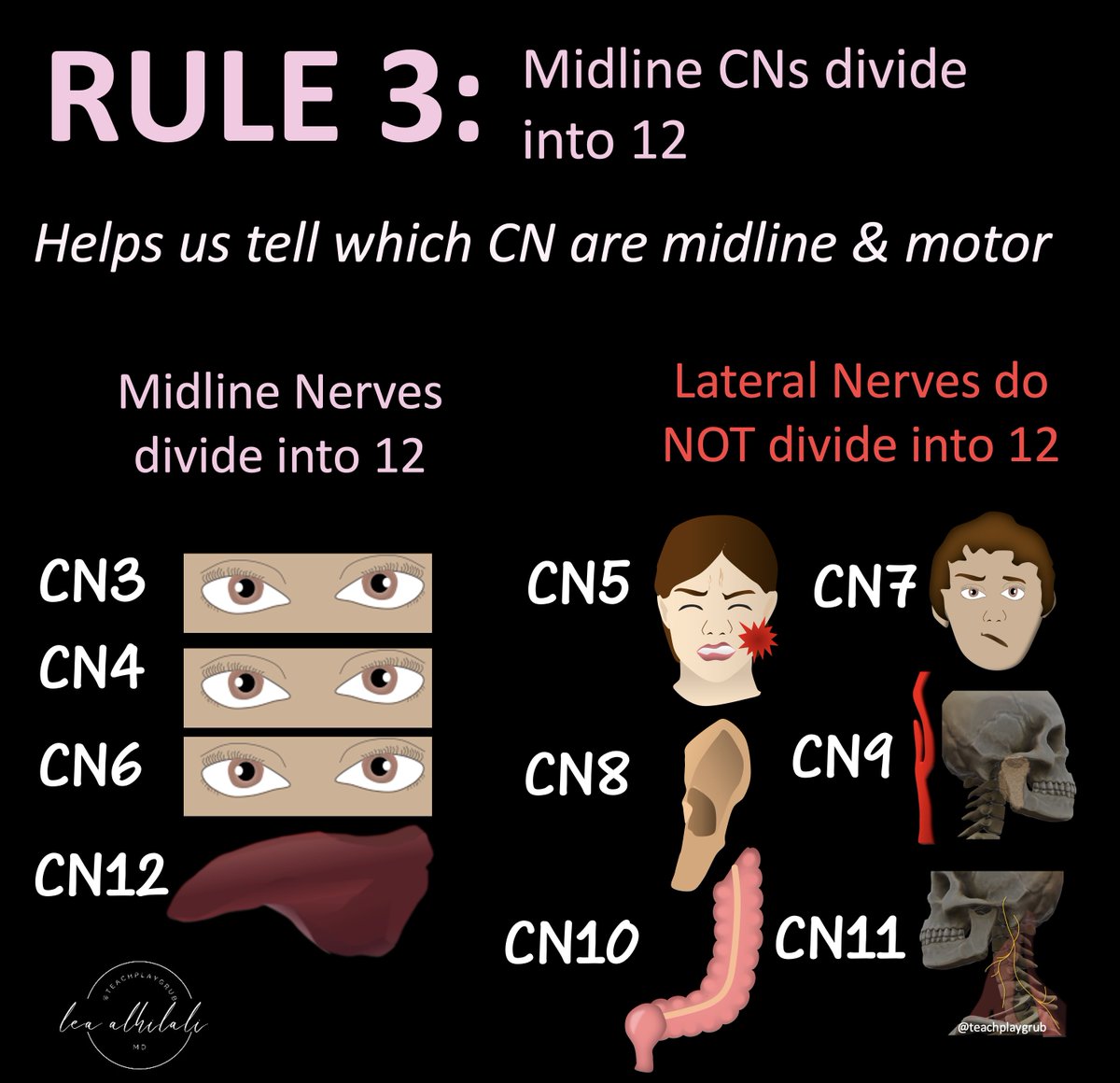
8/Rule 3: Motor/medial cranial nerves divide into 12
This helps us know which CNs are medial & which are lateral
If the cranial nerve can divide into 12, then it's a motor nerve and it's medial. This means a medial lesion!
This helps us know which CNs are medial & which are lateral
If the cranial nerve can divide into 12, then it's a motor nerve and it's medial. This means a medial lesion!
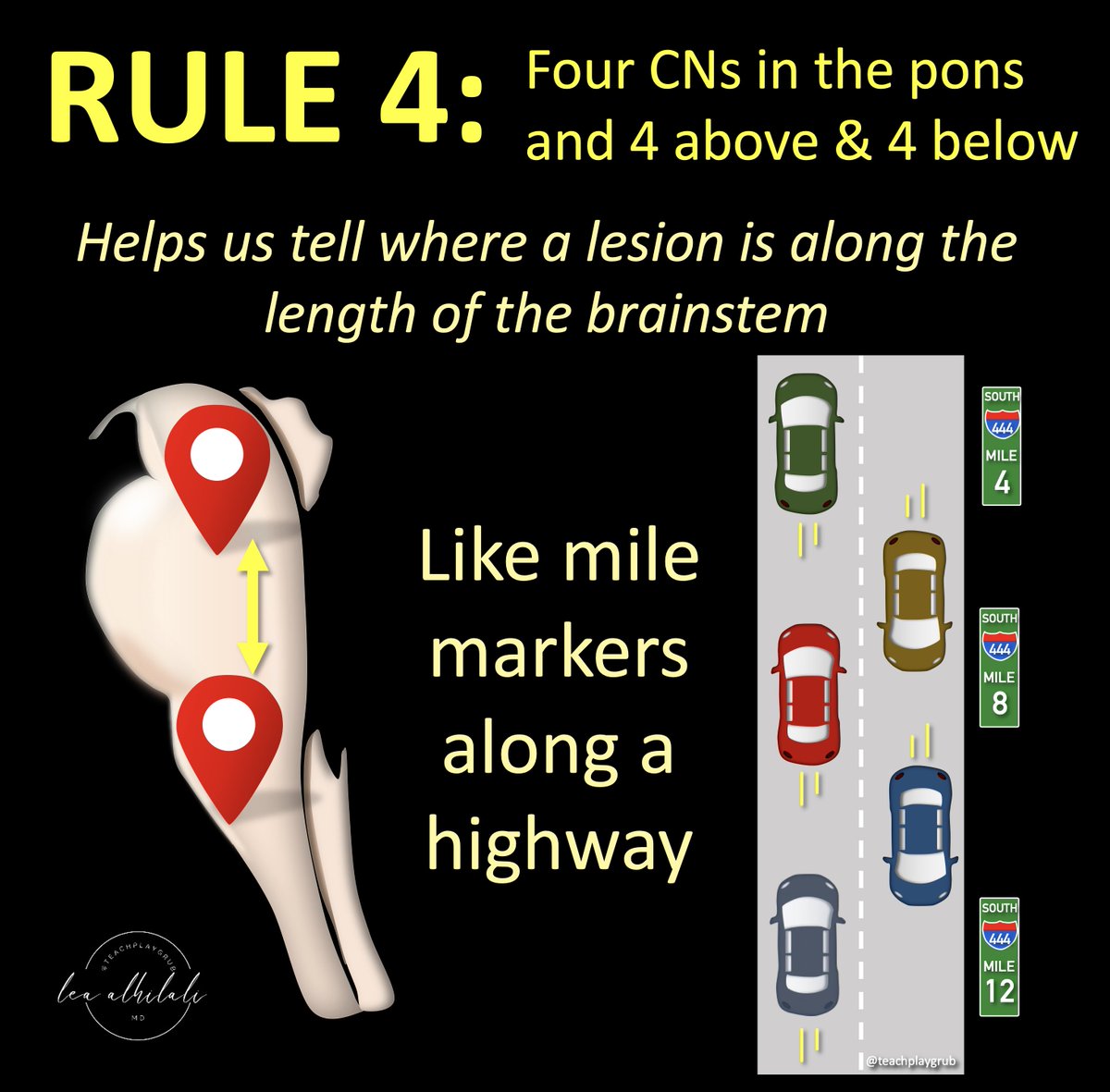
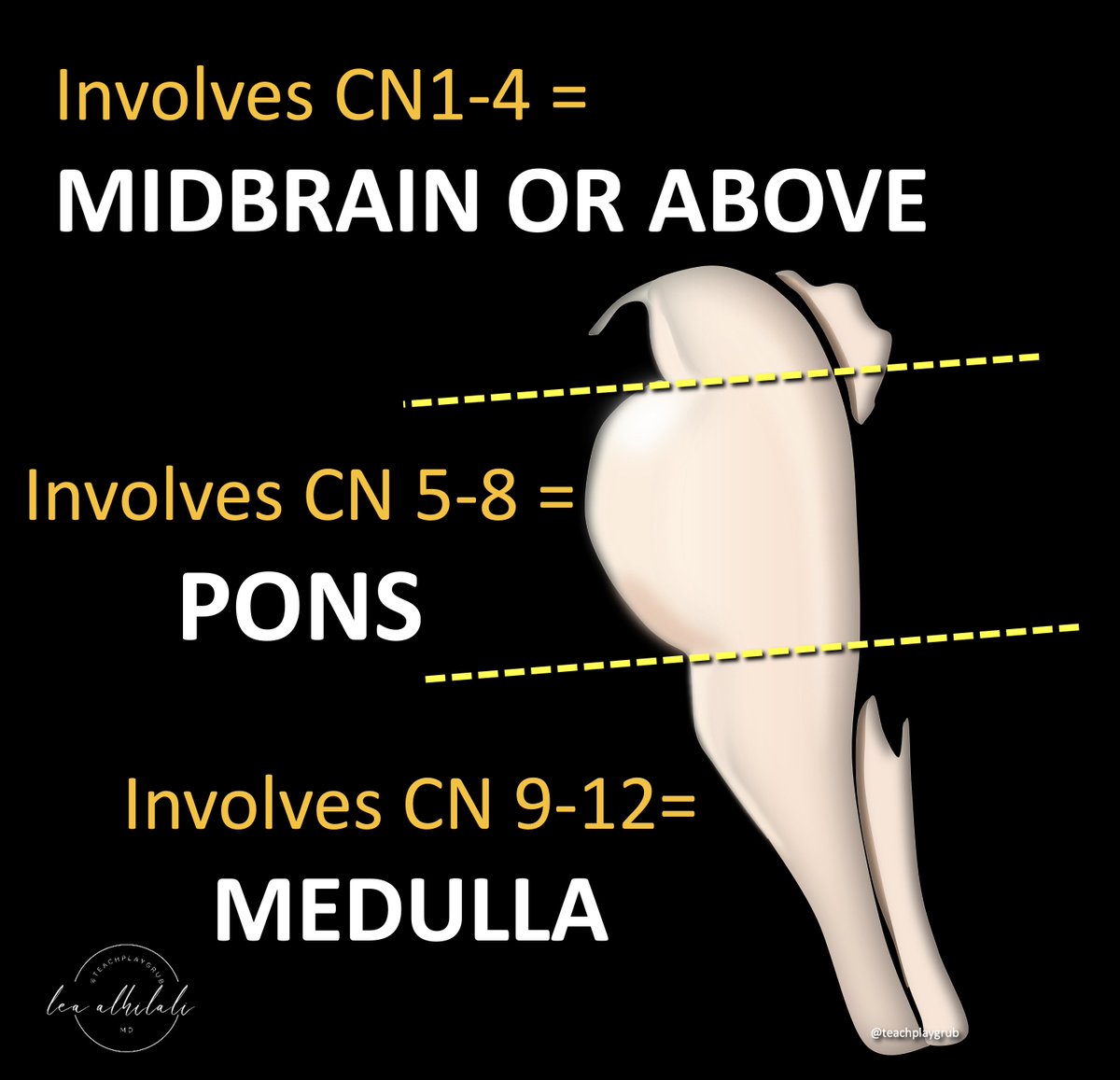
9/Rule 4: Four CN in the pons w/4 above the pons & 4 below
Helps to localize superior/inferior in the brainstem by which CN is involved
CNs are like mile markers along a highway--they let you know how far along you are
Helps to localize superior/inferior in the brainstem by which CN is involved
CNs are like mile markers along a highway--they let you know how far along you are
10/There are 4 CNs in each section (medulla, pons, & above the pons).
Counting up from 12, we see 9-12 are in the medulla, 5-8 in the pons, and 1-4 above the pons.
So depending on what CN is involved, we know if the lesions is in the pons, below the pons or above the pons!
Counting up from 12, we see 9-12 are in the medulla, 5-8 in the pons, and 1-4 above the pons.
So depending on what CN is involved, we know if the lesions is in the pons, below the pons or above the pons!
11/So for every brainstem lesion, you can now do 3 things:
1. Find where it is along the length of the brainstem using CN involvement
2. See if it’s ant or post based on whether motor is involved
3. Determine if it’s med or lat based on type of sensory deficit & CN involvement
1. Find where it is along the length of the brainstem using CN involvement
2. See if it’s ant or post based on whether motor is involved
3. Determine if it’s med or lat based on type of sensory deficit & CN involvement
12/Now you can localize brainstem lesions in all 3 planes based on their clinical presentation!
Localization is actually quite complex, but the Rule of Four is a great foundation!
Hopefully now when confronted w/a brainstem syndrome, you will no longer be locked in!
Localization is actually quite complex, but the Rule of Four is a great foundation!
Hopefully now when confronted w/a brainstem syndrome, you will no longer be locked in!
• • •
Missing some Tweet in this thread? You can try to
force a refresh