
* very important study results*
- patients with long Covid with normal CTPA ( scan looking for pulmonary embolism) found to have abnormal lung perfusion ( blood supply) on VQ scanning
-shortness of breath is one of the most common symptoms in long Covid

- patients with long Covid with normal CTPA ( scan looking for pulmonary embolism) found to have abnormal lung perfusion ( blood supply) on VQ scanning
-shortness of breath is one of the most common symptoms in long Covid



Many patients have not been given an explanation for this shortness of breath
- many still drop their oxygen levels 5 years on and have no reason or treatment
- we have long suspected this is a problem with blood vessel damage
- it has been difficult to get this message out
- many still drop their oxygen levels 5 years on and have no reason or treatment
- we have long suspected this is a problem with blood vessel damage
- it has been difficult to get this message out
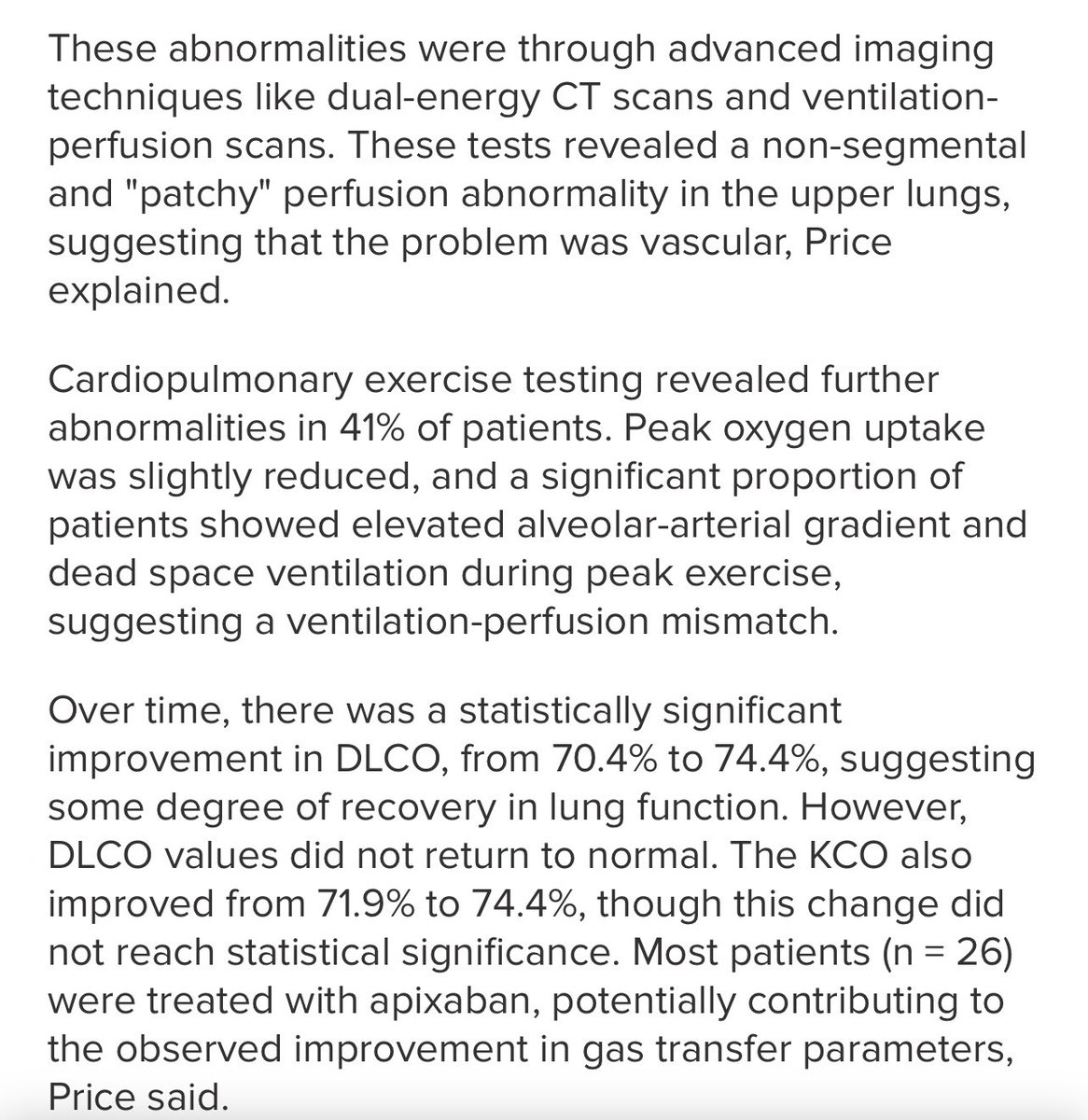
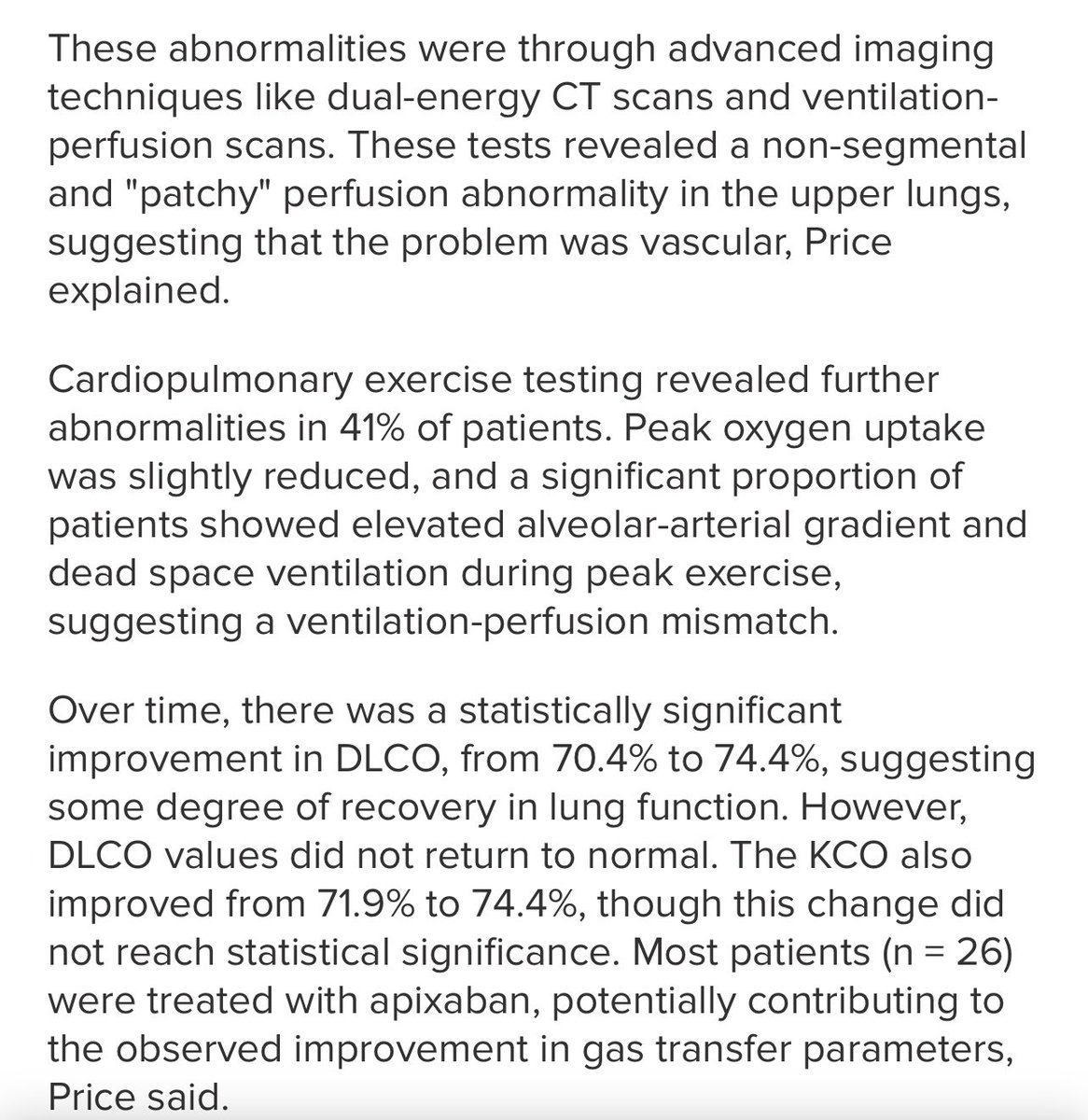
Exercise intolerance was the predominant symptom, affecting 95.1% of the group. A significant proportion (46.3%) presented with myopericarditis, while a smaller subset (n = 5) exhibited dysautonomia.
This is what we all see in long Covid clinics over and over again
This is what we all see in long Covid clinics over and over again

"These patients are young, female, nonsmokers, and previously healthy. This is not what you would expect to see," Price said.
Again, this is exactly what we have been saying for 4 years. Anyone can get long Covid.
Again, this is exactly what we have been saying for 4 years. Anyone can get long Covid.

Most patients (26) were treated with apixaban, potentially contributing to the observed improvement in gas transfer parameters, Price said.
There has been much criticism of this approach previously,leading to dramatic headlines about patients going abroad for unproven treatment
There has been much criticism of this approach previously,leading to dramatic headlines about patients going abroad for unproven treatment
We currently have national long Covid guidelines with no treatment.
We don’t even have national POTS guidelines
How would most doctors know that this shortness of breath may well be vascular?
They look at the guideline and it is years out of date.
We don’t even have national POTS guidelines
How would most doctors know that this shortness of breath may well be vascular?
They look at the guideline and it is years out of date.
I have written many times to say although a patient has a normal CTPA I think they need a VQ scan
- prior to The pandemic we did VQ scan as gold standard test for blood clots
- CTPA is quicker and we needed a way to scan lots of people in 2020
- prior to The pandemic we did VQ scan as gold standard test for blood clots
- CTPA is quicker and we needed a way to scan lots of people in 2020
However, we have never really went back to doing them as standard
- DECT scanning is not available in many areas of the country
- DECT scanning is not available in many areas of the country
Dr Dr Price identified a distinct ‘phenotype of patients with persistent’ post-COVID-19 infection symptoms characterized by abnormal lung perfusion and reduced gas diffusion capacity, even when CT scans appear normal.

Gas diffusion capacity is measured on ‘pulmonary function tests’, a standard test for shortness of breath.
- on its own an abnormal
Result is often not acted upon
- on its own an abnormal
Result is often not acted upon

What this study shows is that if the CTPA is normal ( usual for long Covid) but gas transfer is low, the VQ scan will often show a problem with perfusion.
Price explains
‘this pulmonary microangiopathy may explain the persistent symptoms. However, questions remain about the underlying mechanisms, potential treatments, and long-term outcomes for this patient population.’
‘this pulmonary microangiopathy may explain the persistent symptoms. However, questions remain about the underlying mechanisms, potential treatments, and long-term outcomes for this patient population.’
PULMONARY MICROANGIOPATHY
Pulmonary= lung
Microangiopathy=disease of the small blood vessels
We know Covid causes inflammation of the lining of the blood vessels ( endothelium)
Pulmonary= lung
Microangiopathy=disease of the small blood vessels
We know Covid causes inflammation of the lining of the blood vessels ( endothelium)

Inflammation of the small blood vessels is not seen on
The most common test CTPA.
But perfusion defects can be seen on VQ or DECT.
All of a sudden, the mysterious shortness of breath is not a mystery.
The most common test CTPA.
But perfusion defects can be seen on VQ or DECT.
All of a sudden, the mysterious shortness of breath is not a mystery.
‘It is possible these patients have had inflammation insults that have damaged the pulmonary vascular endothelium, which predisposes them to either clotting at a microscopic level or ongoing inflammation," said Hinks.
@resiapretorius and @dbkell have published extensively about ‘Microclots’
Others have published about ‘micro aggregates’
Others have published about ‘micro aggregates’
Dr Graham Lloyd Jones is a radiologist who years ago raised the alarm about Covid- 19 not causing a typical pneumonia, but blood vessel inflammation @DrGrahamLJ
radiologymasterclass.co.uk/tutorials/covi…
radiologymasterclass.co.uk/tutorials/covi…
A radiologist specialises in interpreting scans. He could see from the scans that what we were dealing with was not normal. That blood vessels may not always show big clots ( pulmonary embolus) on CT scans but other scans may eg DECT
This is a 2020 paper
pubs.rsna.org/radiology/doi/…
This is a 2020 paper
pubs.rsna.org/radiology/doi/…
Whatever we call it, inflammation begets inflammation. This causes a collection of immune cells in the vessels.
We know that risk of heart attack, pulmonary embolism and stroke increases with Covid infection
We know that risk of heart attack, pulmonary embolism and stroke increases with Covid infection
‘Price encouraged physicians to look beyond conventional diagnostic tools when visiting a patient whose CT scan looks normal yet experiences fatigue& breathlessness.
Not knowing what causes the abnormalities observed in these patients makes treatment challenging’
Not knowing what causes the abnormalities observed in these patients makes treatment challenging’
The work of people like
@resiapretorius @PutrinoLab and others helps with linking
the pathology with the clinical symptoms, PFTs and scan results.
@resiapretorius @PutrinoLab and others helps with linking
the pathology with the clinical symptoms, PFTs and scan results.
This was presented at a conference- I would expect a research paper to drop soon
medscape.com/viewarticle/pa…
medscape.com/viewarticle/pa…
This study was done in London. There are ongoing studies.
Progress is slow especially to get things into practice, but it is so encouraging to see what you suspect being proved. And knowing that work is being done to further knowledge that will hopefully turn into treatment.
Progress is slow especially to get things into practice, but it is so encouraging to see what you suspect being proved. And knowing that work is being done to further knowledge that will hopefully turn into treatment.
And for those at the back:
Covid infection is never good.
Each infection is the role of a dice
You may be ok
Or you may end up exercise intolerant, fatigued, unable to tolerate being upright& relapsing on any activity.
Please take care out there.
Covid infection is never good.
Each infection is the role of a dice
You may be ok
Or you may end up exercise intolerant, fatigued, unable to tolerate being upright& relapsing on any activity.
Please take care out there.
*as always, only take medical advice from your treating clinician. However, if you have concerns something is being overlooked please send them papers like this. If something doesn’t feel right, it probably isn’t.

Link to previous post in 2022
https://x.com/drclairetaylor/status/1534659652901822465?s=46&t=x5zAnjMFOis7mfC5WZbcIA
https://twitter.com/drclairetaylor/status/1534659652901822465
Link to previous post about ‘finding the clots’
https://twitter.com/drclairetaylor/status/1589369595726823424
• • •
Missing some Tweet in this thread? You can try to
force a refresh






