This is Dr Lisa Ritchie who was the Head of Infection Prevention & Control for NHS England & Chair of the IPC Cell.
In this video, she explains why patients should never wear FFP3 masks - even if they are known to be highly infectious or if they are clinically vulnerable…
/1
In this video, she explains why patients should never wear FFP3 masks - even if they are known to be highly infectious or if they are clinically vulnerable…
/1
The rationale she gives is that FFP3 masks have valves which the infectious particles can ‘leak’ out through.
Surely the obvious next question is:
So why don’t they recommend UNVALVED FFP3 masks for infectious or clinically vulnerable patients?
/2
Surely the obvious next question is:
So why don’t they recommend UNVALVED FFP3 masks for infectious or clinically vulnerable patients?
/2

Even more bizarre is the fact that, just 20 minutes earlier, she had been shown a document which she herself had co-authored.
This document included IPC guidance for SARS-CoV-1 and *supposedly* formed the initial basis for SARS-CoV-2 (Covid) IPC guidance…
/3
This document included IPC guidance for SARS-CoV-1 and *supposedly* formed the initial basis for SARS-CoV-2 (Covid) IPC guidance…
/3
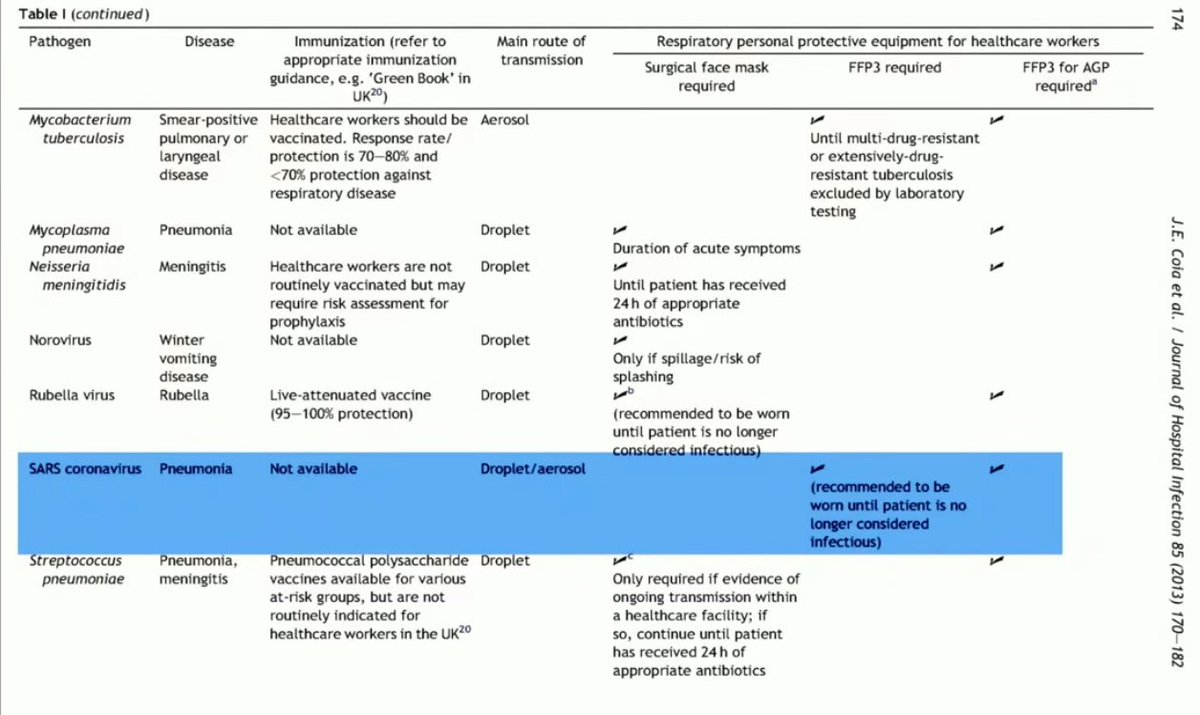
In this document (which supposedly formed the basis for initial Covid IPC guidance), it clearly states that, for SARS-1:
▪️Main route of transmission was droplets & aerosols
▪️FFP3 masks are REQUIRED & recommended to be worn until patient is no longer considered infectious
/4
▪️Main route of transmission was droplets & aerosols
▪️FFP3 masks are REQUIRED & recommended to be worn until patient is no longer considered infectious
/4
So, as Baroness Hallett points out:
…if FFP3 masks *were* recommended to be worn until patients were no longer considered infectious for SARS-CoV-1…
…and if SARS-CoV-1 was meant to be guiding the initial IPC guidance for Covid…
…why on earth didn’t it?
/5
…if FFP3 masks *were* recommended to be worn until patients were no longer considered infectious for SARS-CoV-1…
…and if SARS-CoV-1 was meant to be guiding the initial IPC guidance for Covid…
…why on earth didn’t it?
/5
We were then shown an extract from Prof Beggs’ report:
“By end of Sept 2020 there was enough moderate certainty evidence to strongly suggest that SARS-CoV-2 could be transmitted via the airborne route, and to justify precautionary measures being taken by health authorities”.
/6
“By end of Sept 2020 there was enough moderate certainty evidence to strongly suggest that SARS-CoV-2 could be transmitted via the airborne route, and to justify precautionary measures being taken by health authorities”.
/6
Counsel then asks: “From the IPC cell's perspective was there ever a point where you collectively reached the view that <airborne transmission> was a significant threat & needed to be guarded against with, for example, routine respirators being used?”
Dr Ritchie: “No.”
/7
Dr Ritchie: “No.”
/7
• • •
Missing some Tweet in this thread? You can try to
force a refresh