“Calories in, calories out.”
You’ve surely heard this phrase if you’ve spent any time in the health space. You’ve probably heard it if you’ve spent no time in the health space. This oversimplification of the body’s divine complexity is a relic of outdated nutritional pop-science, and it’s time for it to be thoroughly debunked.
Preamble
I would never outright deny CICO—it can certainly be a useful tool in someone’s weight loss journey. My issue with CICO is the absolutism and rigidity in failing to acknowledge how much it can vary.
When an adult is struggling to lose weight despite eating less food than is recommended for their height, they’re told either “you’re counting wrong” or “just eat less”. What is seldom considered is whether or not that person has a metabolic problem. As we will see, this is very often the case.
What you eat matters just as much as how much you eat.[1] The goal is to increase basal metabolic rate—or “calories out”—not to perpetually decrease “calories in”.
Overview
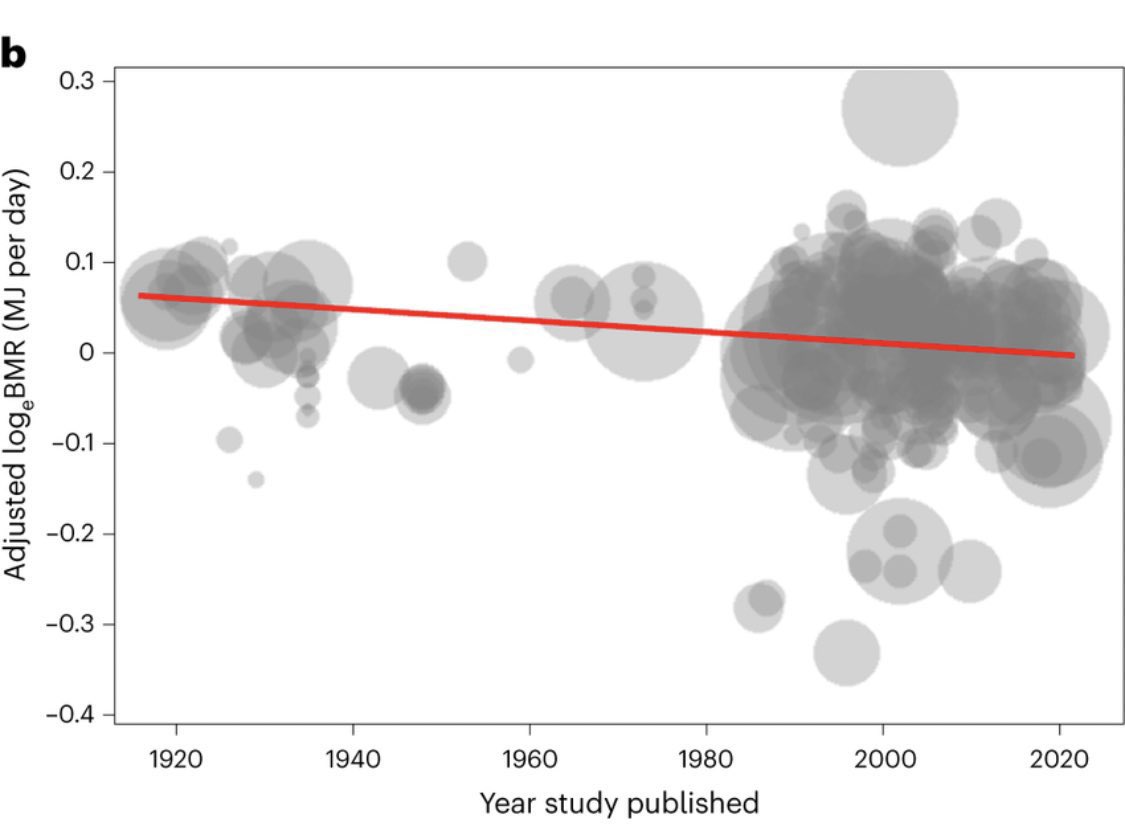
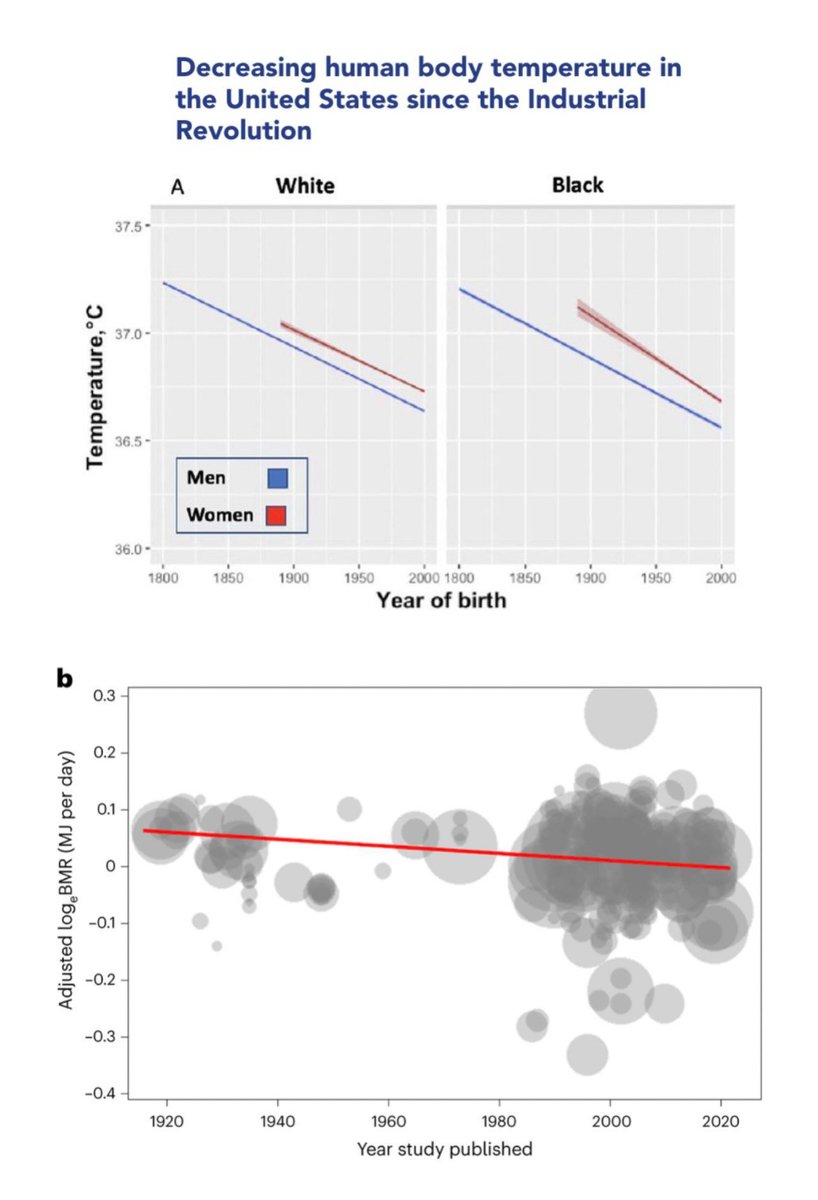
● Metabolic rate has been decreasing for over a century[2][3]
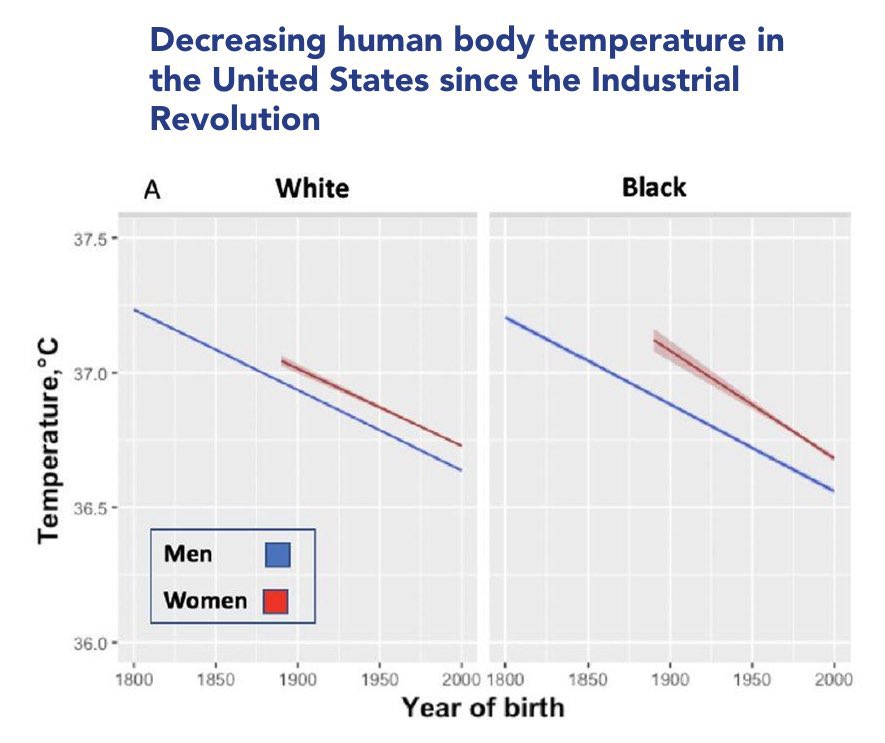
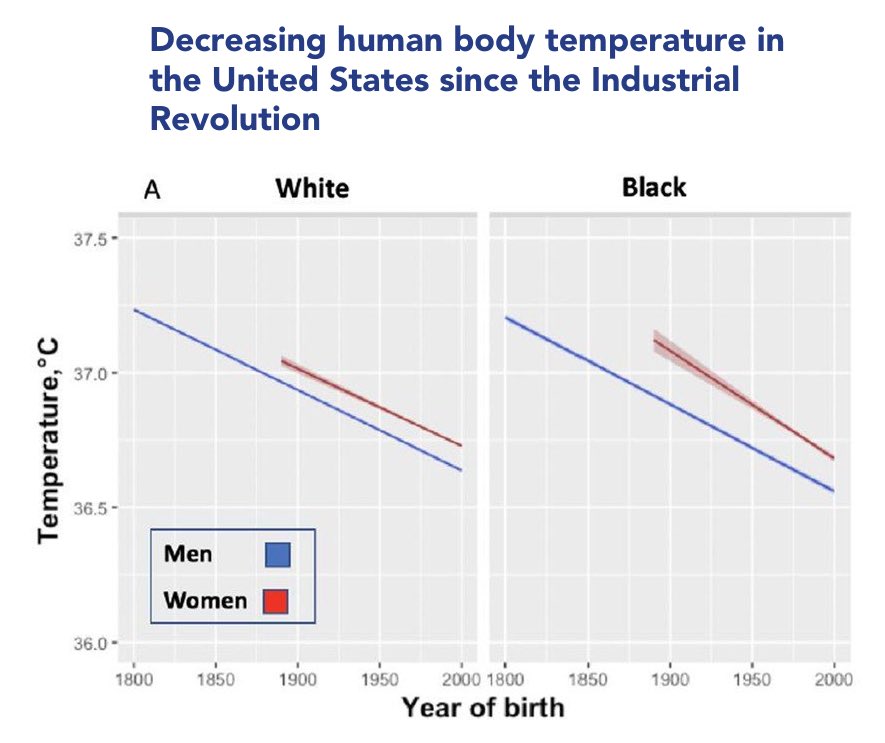
● Average body temperature has been decreasing for over a century[4]
● Daily energy expenditure has declined over the past 3 decades due to decreased basal metabolic rate—not reduced activity[5]
● We consumed more food in the past yet we were thinner[6][7][8]
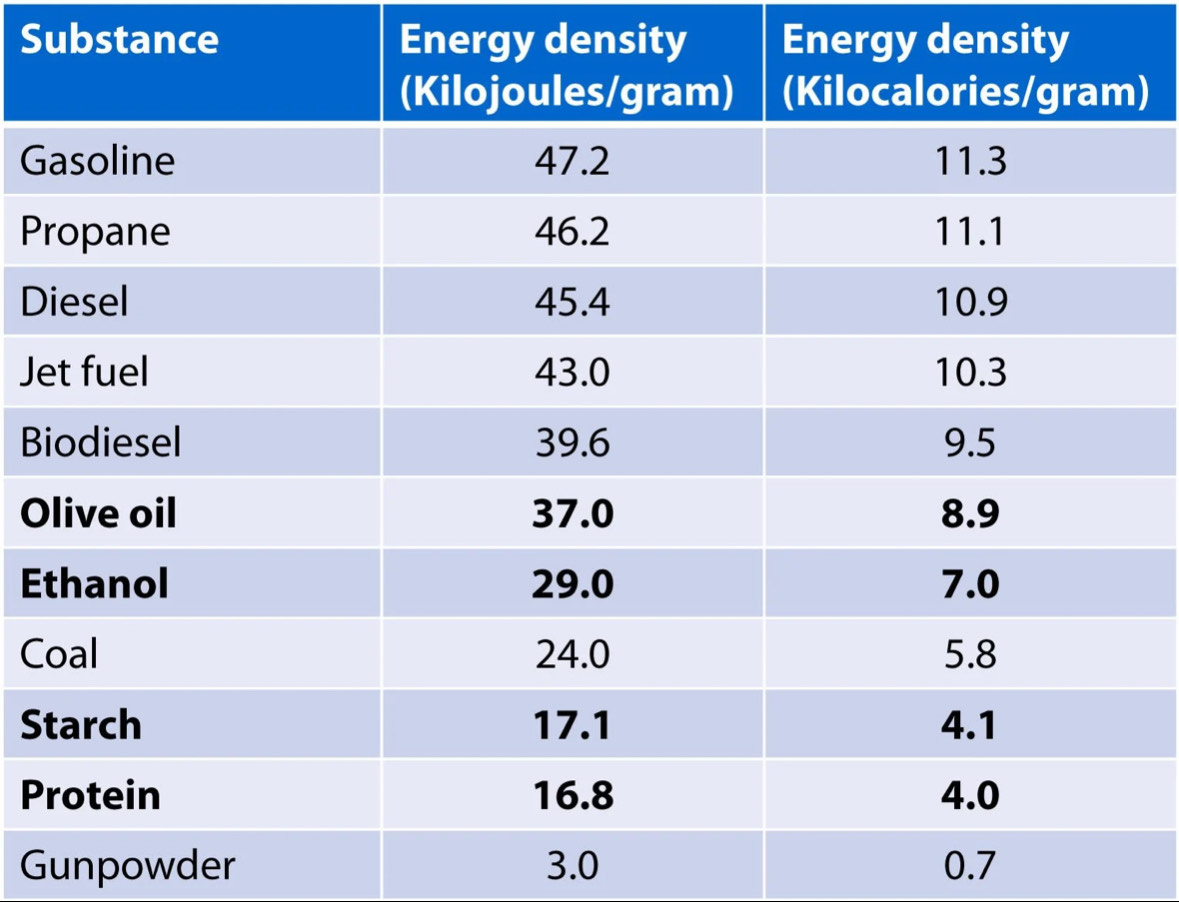
● Different macronutrients yield different amounts of ATP
● Different macronutrient ratios impact hormonal profile, which in turn influences both metabolic rate and body composition[9][10]
● We can ballpark “calories in”, but we can’t definitively know what happens between that and “calories out” without understanding all the metabolic pathway variance that can occur along the way
● Counting calories is useful only as a gauge of current basal metabolic rate, but it must be understood that this is subject to change
● Excessive caloric restriction slows metabolism and makes fat gain more likely upon return to maintenance[11]
● Some people would benefit from simply eating less while others would be much better served focusing on increasing basal metabolic rate with intentional daily choices
You’ve surely heard this phrase if you’ve spent any time in the health space. You’ve probably heard it if you’ve spent no time in the health space. This oversimplification of the body’s divine complexity is a relic of outdated nutritional pop-science, and it’s time for it to be thoroughly debunked.
Preamble
I would never outright deny CICO—it can certainly be a useful tool in someone’s weight loss journey. My issue with CICO is the absolutism and rigidity in failing to acknowledge how much it can vary.
When an adult is struggling to lose weight despite eating less food than is recommended for their height, they’re told either “you’re counting wrong” or “just eat less”. What is seldom considered is whether or not that person has a metabolic problem. As we will see, this is very often the case.
What you eat matters just as much as how much you eat.[1] The goal is to increase basal metabolic rate—or “calories out”—not to perpetually decrease “calories in”.
Overview
● Metabolic rate has been decreasing for over a century[2][3]
● Average body temperature has been decreasing for over a century[4]
● Daily energy expenditure has declined over the past 3 decades due to decreased basal metabolic rate—not reduced activity[5]
● We consumed more food in the past yet we were thinner[6][7][8]
● Different macronutrients yield different amounts of ATP
● Different macronutrient ratios impact hormonal profile, which in turn influences both metabolic rate and body composition[9][10]
● We can ballpark “calories in”, but we can’t definitively know what happens between that and “calories out” without understanding all the metabolic pathway variance that can occur along the way
● Counting calories is useful only as a gauge of current basal metabolic rate, but it must be understood that this is subject to change
● Excessive caloric restriction slows metabolism and makes fat gain more likely upon return to maintenance[11]
● Some people would benefit from simply eating less while others would be much better served focusing on increasing basal metabolic rate with intentional daily choices
CICO and thermodynamics
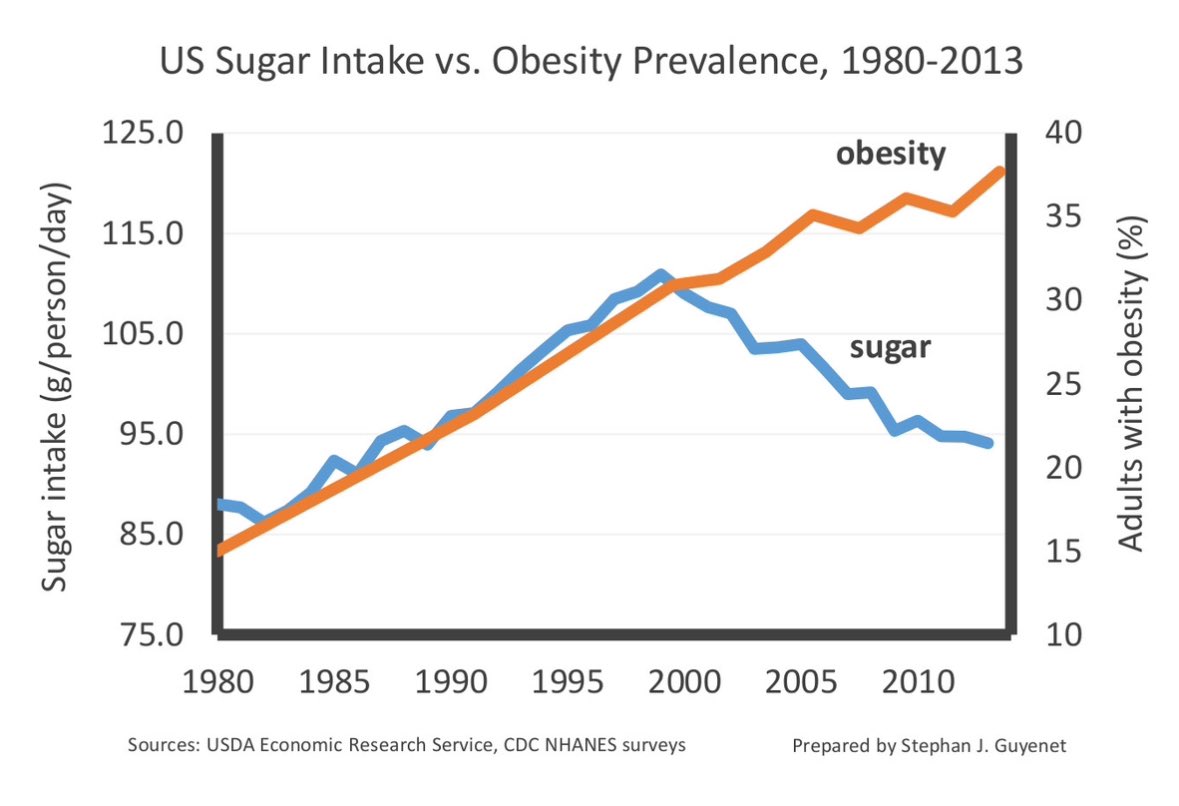
“We are currently expending about 220 calories per day less for males and 122 calories per day less for females than people of our age and body composition were in the late 1980s. These changes are sufficient to explain the obesity epidemic in the USA.”[12]
—John Speakman (@johnspeakman4), biologist
CICO absolutists will say that weight loss and gain come down to “thermodynamics”, yet the graphs of body temperature and basal metabolic rate (BMR) steadily decreasing every decade seem to be lost on them.
According to a study in Metabolism Journal, a drop in body temperature of one degree Celsius is equal to a 10-13% reduction in metabolic rate.
Thermodynamics is not reducible to elementary math. In fact, as we’ll see, “a calorie is a calorie”—and CICO, by extension—violates the second law of thermodynamics because of variances in metabolic efficiency.
“We are currently expending about 220 calories per day less for males and 122 calories per day less for females than people of our age and body composition were in the late 1980s. These changes are sufficient to explain the obesity epidemic in the USA.”[12]
—John Speakman (@johnspeakman4), biologist
CICO absolutists will say that weight loss and gain come down to “thermodynamics”, yet the graphs of body temperature and basal metabolic rate (BMR) steadily decreasing every decade seem to be lost on them.
According to a study in Metabolism Journal, a drop in body temperature of one degree Celsius is equal to a 10-13% reduction in metabolic rate.
Thermodynamics is not reducible to elementary math. In fact, as we’ll see, “a calorie is a calorie”—and CICO, by extension—violates the second law of thermodynamics because of variances in metabolic efficiency.
We used to eat more (and move less)
“Eat less, move more” is another mantra you’ll hear alongside “calories in, calories out”. As it turns out, we used to do the opposite… with better results.
● A study on US Army soldiers found that they were eating between 5,250 and 5,650 calories a day (even more when temperatures dropped) despite only weighing an average of 157 pounds[13] In addition to a balanced diet of meat, milk, potatoes, fruits and vegetables, the soldiers were eating ¾ cup to half a pound of refined sugar daily
● In Denmark, sedentary people were consistently recorded eating over 3,000 calories daily[14]
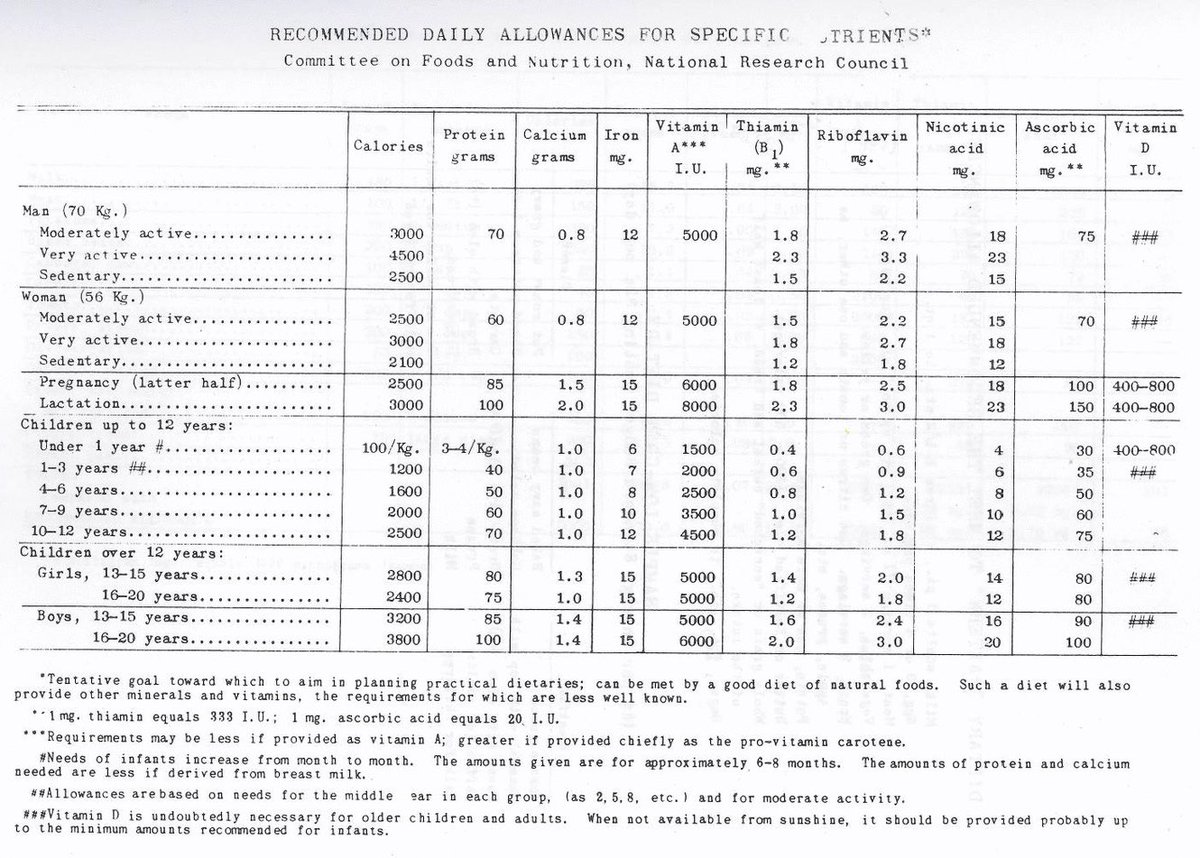
● According to the 1939 US Yearbook of Agriculture, we consumed anywhere from 3,500-4,000 calories daily and averaged 154 pounds while being only moderately active[15]
● As @NangaParbat1618 points out, lumberjacks in the late 16th century were averaging 6,000-7,700 calories a day and even the lowest estimated caloric intake recorded at that time was still over 3,000 calories a day[16][17]
The idea that increasing the “CO” portion of CICO is “violating the laws of thermodynamics” comically oversimplifies the process of energy metabolism and assumes that everybody breaks down food equally efficiently.
This is not the case.
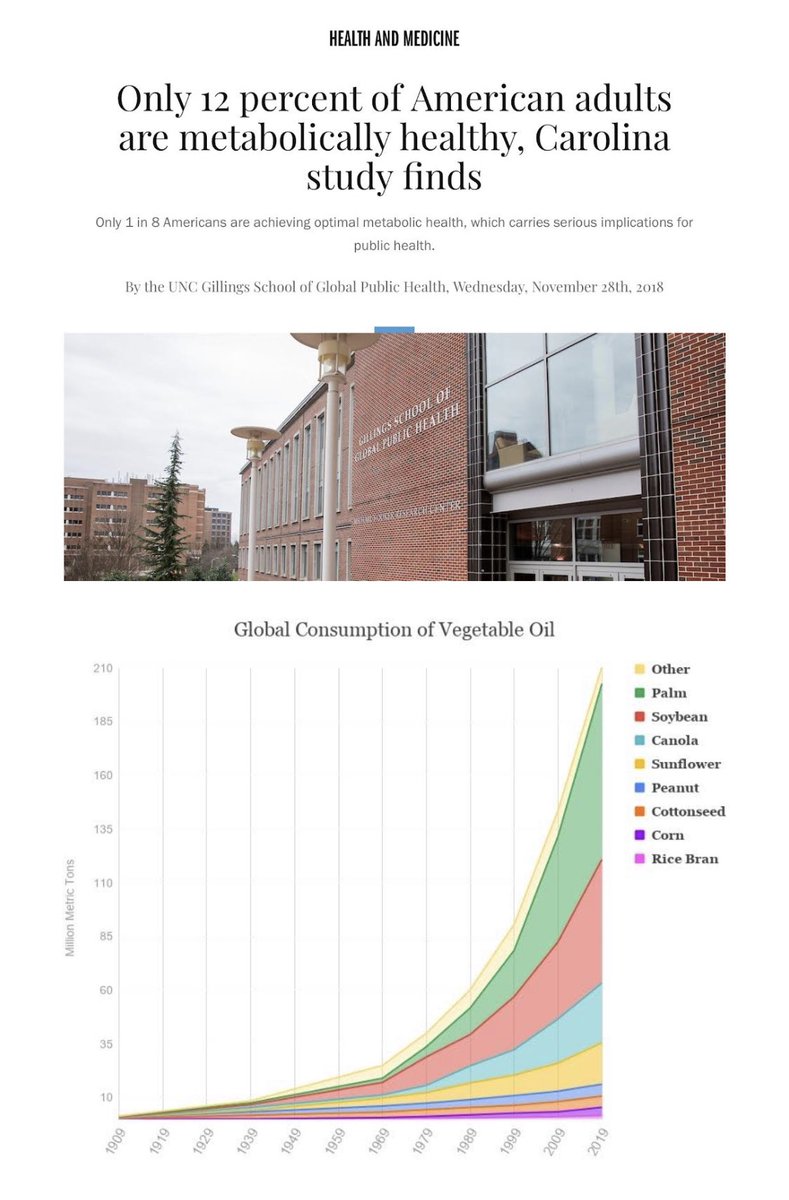
Studies show only 12% of people now are metabolically healthy,[18] meaning only 12% of people are making efficient use of the food they eat.
“The second law of thermodynamics says that variation of efficiency for different metabolic pathways is to be expected. Thus, ironically the dictum that a "calorie is a calorie" violates the second law of thermodynamics, as a matter of principle.”[19]
Not only is there variance in the ATP produced from dietary macros, but protein broken down for fuel (as seen in gluconeogenesis) and fat (liberated from storage by adrenaline during stress) also make differing amounts of ATP and have different impacts on our hormones, which, in turn, effect body composition.
There is a world of nuance we skip over in that space between “calories in” and “calories out”.
“Eat less, move more” is another mantra you’ll hear alongside “calories in, calories out”. As it turns out, we used to do the opposite… with better results.
● A study on US Army soldiers found that they were eating between 5,250 and 5,650 calories a day (even more when temperatures dropped) despite only weighing an average of 157 pounds[13] In addition to a balanced diet of meat, milk, potatoes, fruits and vegetables, the soldiers were eating ¾ cup to half a pound of refined sugar daily
● In Denmark, sedentary people were consistently recorded eating over 3,000 calories daily[14]
● According to the 1939 US Yearbook of Agriculture, we consumed anywhere from 3,500-4,000 calories daily and averaged 154 pounds while being only moderately active[15]
● As @NangaParbat1618 points out, lumberjacks in the late 16th century were averaging 6,000-7,700 calories a day and even the lowest estimated caloric intake recorded at that time was still over 3,000 calories a day[16][17]
The idea that increasing the “CO” portion of CICO is “violating the laws of thermodynamics” comically oversimplifies the process of energy metabolism and assumes that everybody breaks down food equally efficiently.
This is not the case.
Studies show only 12% of people now are metabolically healthy,[18] meaning only 12% of people are making efficient use of the food they eat.
“The second law of thermodynamics says that variation of efficiency for different metabolic pathways is to be expected. Thus, ironically the dictum that a "calorie is a calorie" violates the second law of thermodynamics, as a matter of principle.”[19]
Not only is there variance in the ATP produced from dietary macros, but protein broken down for fuel (as seen in gluconeogenesis) and fat (liberated from storage by adrenaline during stress) also make differing amounts of ATP and have different impacts on our hormones, which, in turn, effect body composition.
There is a world of nuance we skip over in that space between “calories in” and “calories out”.

A calorie is not a calorie is not a calorie
Jay Feldman breaks down the variance between fuel substrates in a recent video,[20] but here’s a quick summary of some key points:
Weight and calories are not equivalent.
● 1 lb of pure protein is about 1,800 calories
● 1 lb of pure fat is about 4,000 calories
● 1 lb of pure water is 0 calories
Drinking a pound of water before stepping on a scale is not comparable to eating 1 pound of lean protein (hello hypoglycemia) before stepping on a scale.
● 100 calories of palmitate (a fatty acid) = 4.7 moles of ATP
● 100 calories of glucose (a carbohydrate) = 4.4 moles of ATP
● 100 calories of leucine (an amino acid) = 3.8 moles of ATP
● 100 calories of aspartate via gluconeogenesis (an amino acid, in this case being broken down from our own tissue) = 2.2 moles of ATP
“Unless one measures heat and the biomolecules synthesized using ATP, it is inappropriate to assume that the only thing that counts in terms of food consumption and energy balance is the intake of dietary calories and weight storage.”[21]
A tablespoon of canola oil a day will eventually yield dramatically different results than a tablespoon of coconut oil a day. In fact, the reason we call “essential fatty acids” “essential” is due to a misconception borne out of this fact.
Jay Feldman breaks down the variance between fuel substrates in a recent video,[20] but here’s a quick summary of some key points:
Weight and calories are not equivalent.
● 1 lb of pure protein is about 1,800 calories
● 1 lb of pure fat is about 4,000 calories
● 1 lb of pure water is 0 calories
Drinking a pound of water before stepping on a scale is not comparable to eating 1 pound of lean protein (hello hypoglycemia) before stepping on a scale.
● 100 calories of palmitate (a fatty acid) = 4.7 moles of ATP
● 100 calories of glucose (a carbohydrate) = 4.4 moles of ATP
● 100 calories of leucine (an amino acid) = 3.8 moles of ATP
● 100 calories of aspartate via gluconeogenesis (an amino acid, in this case being broken down from our own tissue) = 2.2 moles of ATP
“Unless one measures heat and the biomolecules synthesized using ATP, it is inappropriate to assume that the only thing that counts in terms of food consumption and energy balance is the intake of dietary calories and weight storage.”[21]
A tablespoon of canola oil a day will eventually yield dramatically different results than a tablespoon of coconut oil a day. In fact, the reason we call “essential fatty acids” “essential” is due to a misconception borne out of this fact.
PUFA and torpor; the Burrs and the bears
The Burr and Burr experiments of 1929 and 1930 were said to have found that omega-3 and omega-6 fatty acids (PUFA) were “essential” because the rats deprived of them developed skin issues.
The “essential” fatty acids
● α-linolenic acid (ALA), omega-3
● Eicosapentaenoic acid (EPA), omega-3
● Docosahexaenoic acid (DHA), omega-3
● Linoleic acid (LA), omega-6
● Arachidonic acid (AA), omega-6
The Burrs’ very minimal rat diet consisted of purified casein and sucrose, along with a vitamin concentrate and some minerals. Both groups of rats received the diet with one group receiving methyl esters of LA and ALA and the other group no fat source.
What the Burrs failed to account for was that the rats deprived of PUFA had a significantly increased basal respiration and metabolic rate.[22][23] When metabolism increases, so too does the need for nutrients. Back then, many essential nutrients weren’t known: several B vitamins weren’t yet discovered, and selenium, while discovered as an element, was not identified as an essential nutrient until 1957. B7, zinc, selenium, and collagen would have surely helped the rats, but were not provided. Predictably, the PUFA-deficient rats became sick. In reality, all that the Burrs observed were nutrient-deprived rats with fast metabolisms.
Subsequent studies proved this to be the case,[24] finding that PUFA-deprived rats had an increased metabolic rate paralleling increased cytochrome oxidase activity (a crucial component of ATP production in the electron transport chain).[25]
A few years after the Burrs’ rat studies, a man named William Brown agreed to eat a diet in the same vein as the EFA-deficient rats. He consumed a diet of 2500 calories of sugar syrup, skimmed milk, cottage cheese, some orange juice and a potato starch biscuit. Iron, vitamin D, and carotene were supplemented.
Brown had suffered from weekly migraines since he was young, and his blood pressure was slightly elevated at the start of the diet. After a month and a half eating the diet, his migraines stopped and never returned, his blood pressure dropped from an average of 145/98 to 130/87, and he noted a disappearance of fatigue at the end of his day’s work.
On the diet, Brown’s metabolic rate shot up from 9-12% below normal to only 2% below normal, and his weight dropped from 152 pounds to 138. His respiratory quotient (the ratio of CO2 produced to O2 consumed during metabolism) increased to 1.0, meaning his oxidation of glucose improved. In diabetes, the respiratory quotient is low, meaning diabetics are oxidizing fat preferentially while struggling to oxidize carbs.[26]
In other words, Brown avoided PUFA and his thyroid health improved. The thyroid is the master regulator of metabolism; how can its inhibition be irrelevant to the equation?
The lipid peroxidation cascade from PUFA alone is highly energy-wasting: it costs energy to produce antioxidants and repair the damage. Not only this, but PUFA blocks the uptake, transport,[27] and secretion of thyroid hormone.
Since 1909, there has been an over 1000-fold increase in soy oil (mostly PUFA) consumption.[28] Along the same timeline, butter (mostly saturated fat) consumption has gone from 18 pounds consumed per person per year to just about 5.[29]
As @lowmegatron points out in his article “How to Eat Fewer Calories and Gain More Fat”[30], in the period with the greatest increase in obesity rates (1970-2010), seed oil consumption almost tripled. He points out another study where scientists found that rats gained 20% more fat on the same amount of calories from PUFA.[31]
PUFA slows metabolism to a crawl, comparative to a pre-hibernation state. In fact, bears[32] and squirrels[33] increase their consumption of high-PUFA foods before they hibernate. This slowing effect that PUFA has on the metabolism is contrasted beautifully with coconut oil’s (a saturated fat) opposite effect.
The Burr and Burr experiments of 1929 and 1930 were said to have found that omega-3 and omega-6 fatty acids (PUFA) were “essential” because the rats deprived of them developed skin issues.
The “essential” fatty acids
● α-linolenic acid (ALA), omega-3
● Eicosapentaenoic acid (EPA), omega-3
● Docosahexaenoic acid (DHA), omega-3
● Linoleic acid (LA), omega-6
● Arachidonic acid (AA), omega-6
The Burrs’ very minimal rat diet consisted of purified casein and sucrose, along with a vitamin concentrate and some minerals. Both groups of rats received the diet with one group receiving methyl esters of LA and ALA and the other group no fat source.
What the Burrs failed to account for was that the rats deprived of PUFA had a significantly increased basal respiration and metabolic rate.[22][23] When metabolism increases, so too does the need for nutrients. Back then, many essential nutrients weren’t known: several B vitamins weren’t yet discovered, and selenium, while discovered as an element, was not identified as an essential nutrient until 1957. B7, zinc, selenium, and collagen would have surely helped the rats, but were not provided. Predictably, the PUFA-deficient rats became sick. In reality, all that the Burrs observed were nutrient-deprived rats with fast metabolisms.
Subsequent studies proved this to be the case,[24] finding that PUFA-deprived rats had an increased metabolic rate paralleling increased cytochrome oxidase activity (a crucial component of ATP production in the electron transport chain).[25]
A few years after the Burrs’ rat studies, a man named William Brown agreed to eat a diet in the same vein as the EFA-deficient rats. He consumed a diet of 2500 calories of sugar syrup, skimmed milk, cottage cheese, some orange juice and a potato starch biscuit. Iron, vitamin D, and carotene were supplemented.
Brown had suffered from weekly migraines since he was young, and his blood pressure was slightly elevated at the start of the diet. After a month and a half eating the diet, his migraines stopped and never returned, his blood pressure dropped from an average of 145/98 to 130/87, and he noted a disappearance of fatigue at the end of his day’s work.
On the diet, Brown’s metabolic rate shot up from 9-12% below normal to only 2% below normal, and his weight dropped from 152 pounds to 138. His respiratory quotient (the ratio of CO2 produced to O2 consumed during metabolism) increased to 1.0, meaning his oxidation of glucose improved. In diabetes, the respiratory quotient is low, meaning diabetics are oxidizing fat preferentially while struggling to oxidize carbs.[26]
In other words, Brown avoided PUFA and his thyroid health improved. The thyroid is the master regulator of metabolism; how can its inhibition be irrelevant to the equation?
The lipid peroxidation cascade from PUFA alone is highly energy-wasting: it costs energy to produce antioxidants and repair the damage. Not only this, but PUFA blocks the uptake, transport,[27] and secretion of thyroid hormone.
Since 1909, there has been an over 1000-fold increase in soy oil (mostly PUFA) consumption.[28] Along the same timeline, butter (mostly saturated fat) consumption has gone from 18 pounds consumed per person per year to just about 5.[29]
As @lowmegatron points out in his article “How to Eat Fewer Calories and Gain More Fat”[30], in the period with the greatest increase in obesity rates (1970-2010), seed oil consumption almost tripled. He points out another study where scientists found that rats gained 20% more fat on the same amount of calories from PUFA.[31]
PUFA slows metabolism to a crawl, comparative to a pre-hibernation state. In fact, bears[32] and squirrels[33] increase their consumption of high-PUFA foods before they hibernate. This slowing effect that PUFA has on the metabolism is contrasted beautifully with coconut oil’s (a saturated fat) opposite effect.

Hormones and metabolism
The task of turning food into useful energy and structure is too complex to be reduced to a black box input/output model. It bears repeating: what we eat matters as much as how much we eat.
Many young adults disregard this precisely because they’re young. Youth-associated hormones blunt a lot of metabolic damage.[34][35][36] This doesn’t deny that basal metabolic rate controls CICO; rather, it speaks to how stabilizing these hormones are. For these people, however, CICO, with all its flaws, is probably good enough. But we can’t continue to allow predictable euthyroid physiology to turn CICO into absolutist dogma.
Different macronutrient splits can help or hurt thyroid health and hormonal profile. Hormonal profile has huge impacts on not only basal metabolic rate but body composition as well.[37]
Hormones that positively impact metabolism
● Pregnenolone[38]
● Progesterone[39]
● DHEA[40]
● Thyroid[41]
● Testosterone[42]
● DHT[43]
Hormones that negatively impact metabolism
● Cortisol[44][45]
● Estrogen[46][47]
● Aldosterone[48]
● Prolactin[49][50]
● PTH[51]
● TSH[52]
● Leptin[53]
The task of turning food into useful energy and structure is too complex to be reduced to a black box input/output model. It bears repeating: what we eat matters as much as how much we eat.
Many young adults disregard this precisely because they’re young. Youth-associated hormones blunt a lot of metabolic damage.[34][35][36] This doesn’t deny that basal metabolic rate controls CICO; rather, it speaks to how stabilizing these hormones are. For these people, however, CICO, with all its flaws, is probably good enough. But we can’t continue to allow predictable euthyroid physiology to turn CICO into absolutist dogma.
Different macronutrient splits can help or hurt thyroid health and hormonal profile. Hormonal profile has huge impacts on not only basal metabolic rate but body composition as well.[37]
Hormones that positively impact metabolism
● Pregnenolone[38]
● Progesterone[39]
● DHEA[40]
● Thyroid[41]
● Testosterone[42]
● DHT[43]
Hormones that negatively impact metabolism
● Cortisol[44][45]
● Estrogen[46][47]
● Aldosterone[48]
● Prolactin[49][50]
● PTH[51]
● TSH[52]
● Leptin[53]
Crash dieting: never worth the rebound
A major issue with CICO absolutism is that it encourages weight loss strategies such as “crash dieting” (severe caloric restriction). This is a bad idea.
Crash dieting leads to a rebound weight gain and can even speed up fat gain upon a return to maintenance. Crash dieting is the reason for “yo-yo dieting”. Furthermore, it has been shown that basal temperature takes a hit and remains low afterwards, indicating a decline in metabolic rate.[54]
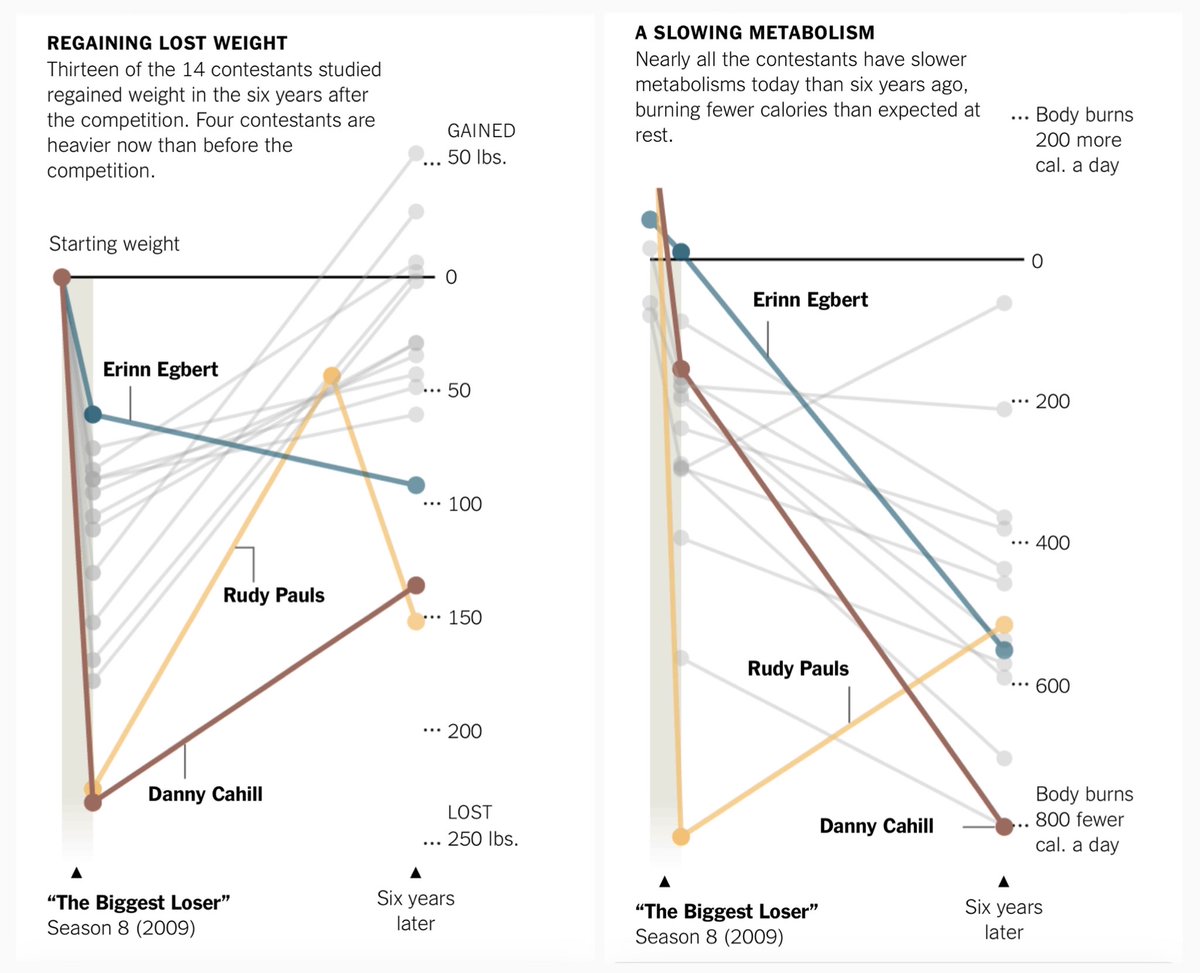
A notable example of this was The Biggest Loser.
Season 8 contestants of The Biggest Loser ended up regaining the weight lost (and then some, in a few instances) after the show ended. Even more confusing—they did it while eating at what should have been their new, healthy maintenance:
“When [the show] ended, their metabolisms had slowed radically and their bodies were not burning enough calories to maintain their thinner sizes.”[55]
Worse still, their metabolic rates failed to return to normal:
“As the years went by and the numbers on the scale climbed, the contestants’ metabolisms did not recover.”[56]
Other studies have found that more exercise does not always yield better results:
“After adjusting for body size and composition, total energy expenditure was positively correlated with physical activity, but the relationship was markedly stronger over the lower range of physical activity.”[57]
With this in mind, short bouts of strength training with adequate rest would be much more effective than hours of breathless exercise.
Why? Part of the reason is energy conservation. It’s actually pretty intuitive: when the body perceives famine (or self-imposed pseudo-famine such as crash dieting and exhaustive exercise), it has evolved mechanisms to stay alive, like slowing metabolism adaptively to focus on core processes, de-prioritizing energetic luxuries like hair growth, nail growth, muscle growth, feeling good, and more.
But a more technical answer would involve PUFA metabolites and something called (get ready for a mouthful) peroxisome proliferator-activated receptor alpha (PPAR-α), a protein tasked with the job of turning genes on and off.
Activation of PPAR-α by fasting, keto diet, or caloric restriction
Brad Marshall (@fire_bottle) has outlined this well[58], but, to summarize:
● PPAR-α controls fat detoxification
● PPAR-α is activated by caloric restriction, fasting, and the keto diet—all of which involve lipolysis
● PPAR-α is especially activated by oleic acid and omega-3s
● PPAR-α oxidizes PUFA (likely to get rid of it)
● The downside to oxidized PUFA is that it causes insulin resistance
● All HETEs are involved in the progression of human obesity
● 12-HETE activates the aryl hydrocarbon receptor (AhR), also involved in obesity
PUFA hurts metabolism, and metabolism should be important to anyone interested in weight loss.
Losing a lot of weight at once liberates a lot of PUFA from storage[59]—particularly LA and AA—and this PUFA can go on to create reactive oxygen species (ROS) via lipid peroxidation chain reactions in the body.[60] Vitamin E effectively breaks these chain reactions,[61] so a good E product should be a priority to anyone losing weight rapidly.
A major issue with CICO absolutism is that it encourages weight loss strategies such as “crash dieting” (severe caloric restriction). This is a bad idea.
Crash dieting leads to a rebound weight gain and can even speed up fat gain upon a return to maintenance. Crash dieting is the reason for “yo-yo dieting”. Furthermore, it has been shown that basal temperature takes a hit and remains low afterwards, indicating a decline in metabolic rate.[54]
A notable example of this was The Biggest Loser.
Season 8 contestants of The Biggest Loser ended up regaining the weight lost (and then some, in a few instances) after the show ended. Even more confusing—they did it while eating at what should have been their new, healthy maintenance:
“When [the show] ended, their metabolisms had slowed radically and their bodies were not burning enough calories to maintain their thinner sizes.”[55]
Worse still, their metabolic rates failed to return to normal:
“As the years went by and the numbers on the scale climbed, the contestants’ metabolisms did not recover.”[56]
Other studies have found that more exercise does not always yield better results:
“After adjusting for body size and composition, total energy expenditure was positively correlated with physical activity, but the relationship was markedly stronger over the lower range of physical activity.”[57]
With this in mind, short bouts of strength training with adequate rest would be much more effective than hours of breathless exercise.
Why? Part of the reason is energy conservation. It’s actually pretty intuitive: when the body perceives famine (or self-imposed pseudo-famine such as crash dieting and exhaustive exercise), it has evolved mechanisms to stay alive, like slowing metabolism adaptively to focus on core processes, de-prioritizing energetic luxuries like hair growth, nail growth, muscle growth, feeling good, and more.
But a more technical answer would involve PUFA metabolites and something called (get ready for a mouthful) peroxisome proliferator-activated receptor alpha (PPAR-α), a protein tasked with the job of turning genes on and off.
Activation of PPAR-α by fasting, keto diet, or caloric restriction
Brad Marshall (@fire_bottle) has outlined this well[58], but, to summarize:
● PPAR-α controls fat detoxification
● PPAR-α is activated by caloric restriction, fasting, and the keto diet—all of which involve lipolysis
● PPAR-α is especially activated by oleic acid and omega-3s
● PPAR-α oxidizes PUFA (likely to get rid of it)
● The downside to oxidized PUFA is that it causes insulin resistance
● All HETEs are involved in the progression of human obesity
● 12-HETE activates the aryl hydrocarbon receptor (AhR), also involved in obesity
PUFA hurts metabolism, and metabolism should be important to anyone interested in weight loss.
Losing a lot of weight at once liberates a lot of PUFA from storage[59]—particularly LA and AA—and this PUFA can go on to create reactive oxygen species (ROS) via lipid peroxidation chain reactions in the body.[60] Vitamin E effectively breaks these chain reactions,[61] so a good E product should be a priority to anyone losing weight rapidly.
Macronutrient ratios matter
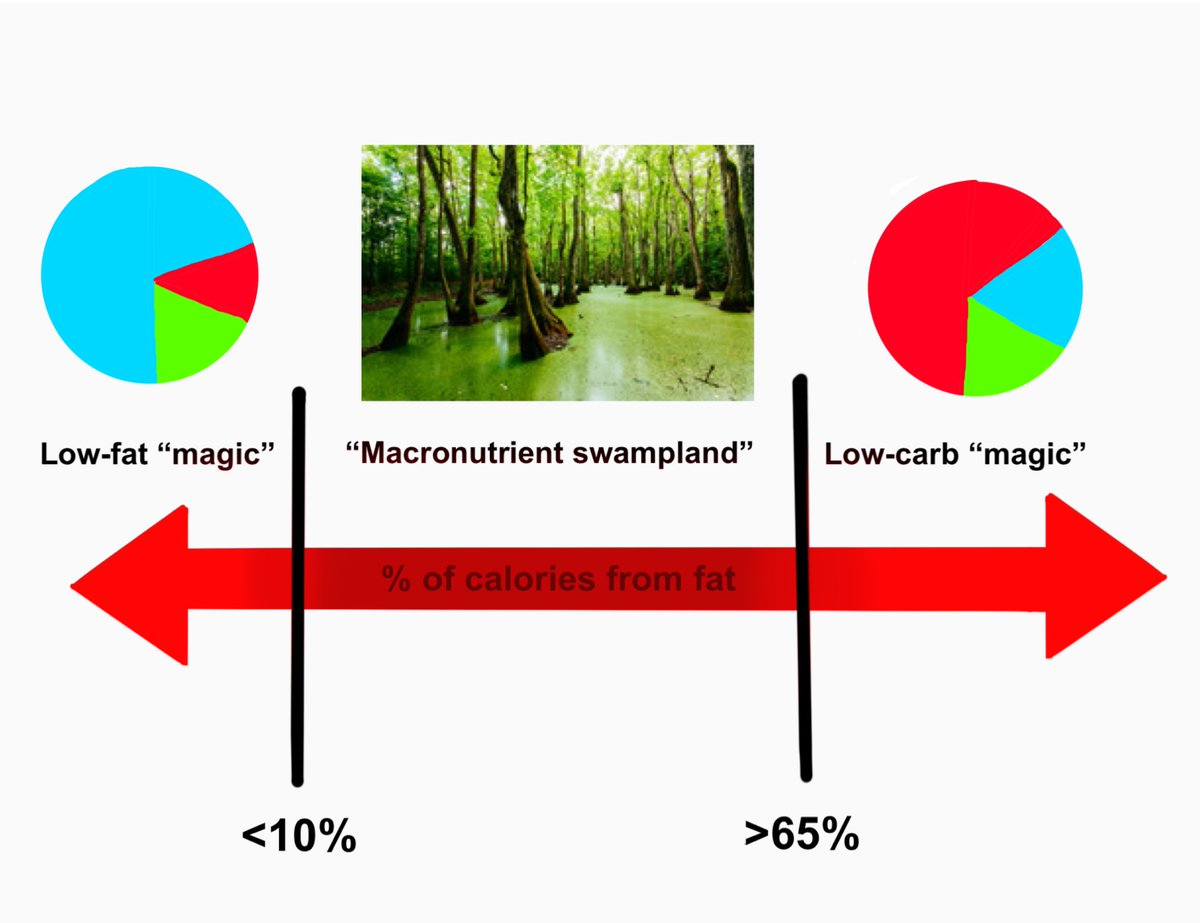
Denise Minger's (@deniseminger) "macronutrient swampland" is a simple concept which grows out of the Randle cycle: if one makes either carbs or fat a dominant macronutrient (minimizing the other), the body becomes adept at using whichever fuel source is prioritized.[62][63]
A meta-analysis of weight loss trials showed a slight benefit in low-carb diets to low-fat, but results converged after about a year.[64] Keep in mind that the definition of low-fat in many low-fat studies is dubious, likely falling into “macronutrient swampland” territory, and that most clinical studies do not extend nearly as long as they should. While a low-carb diet might help with weight loss in more acute stages, the problem is how that weight loss is achieved and what happens afterward.
Here Denise outlines some examples of healthy groups of people with truly low fat diets:
● Okinawans: 12% of calories as fat
● Tarahumara Indians: 12% of calories as fat
● pre-industrialized Thai: 8.9% of calories as fat
● traditional Hawaiian: 10% of calories as fat
● traditional Taiwanese: 16% of calories as fat
● African Bantu: 14 – 17% of calories as fat
● traditional Pima: 8 – 12% of calories as fat
● highlanders of Papua New Guinea: 3% of calories as fat
Contrast these with Americans who average 34% of calories from fat with comparably poor health metrics and you’ll see Denise may be onto something.
In addition to high-carb and (truly) low-fat, there’s evidence of protein restriction (specifically branched-chain amino acid restriction) increasing the metabolic rate. Mice studies showed that restriction of BCAAs (valine, leucine, and isoleucine) lead to a significant reduction in body weight, most notably isoleucine restriction.[65] Fat gain in mice increased with increased dietary protein despite consuming fewer calories overall. In fact, the leanest mice ate the least protein and the most calories (predominantly carbohydrates).[66] In another study, rats with a caloric intake four times higher than their counterparts (via fructose-rich Coca Cola) maintained almost identical weight and blood glucose levels.[67]
With all this in mind, it’s clear that macronutrient ratios matter a lot.
Denise Minger's (@deniseminger) "macronutrient swampland" is a simple concept which grows out of the Randle cycle: if one makes either carbs or fat a dominant macronutrient (minimizing the other), the body becomes adept at using whichever fuel source is prioritized.[62][63]
A meta-analysis of weight loss trials showed a slight benefit in low-carb diets to low-fat, but results converged after about a year.[64] Keep in mind that the definition of low-fat in many low-fat studies is dubious, likely falling into “macronutrient swampland” territory, and that most clinical studies do not extend nearly as long as they should. While a low-carb diet might help with weight loss in more acute stages, the problem is how that weight loss is achieved and what happens afterward.
Here Denise outlines some examples of healthy groups of people with truly low fat diets:
● Okinawans: 12% of calories as fat
● Tarahumara Indians: 12% of calories as fat
● pre-industrialized Thai: 8.9% of calories as fat
● traditional Hawaiian: 10% of calories as fat
● traditional Taiwanese: 16% of calories as fat
● African Bantu: 14 – 17% of calories as fat
● traditional Pima: 8 – 12% of calories as fat
● highlanders of Papua New Guinea: 3% of calories as fat
Contrast these with Americans who average 34% of calories from fat with comparably poor health metrics and you’ll see Denise may be onto something.
In addition to high-carb and (truly) low-fat, there’s evidence of protein restriction (specifically branched-chain amino acid restriction) increasing the metabolic rate. Mice studies showed that restriction of BCAAs (valine, leucine, and isoleucine) lead to a significant reduction in body weight, most notably isoleucine restriction.[65] Fat gain in mice increased with increased dietary protein despite consuming fewer calories overall. In fact, the leanest mice ate the least protein and the most calories (predominantly carbohydrates).[66] In another study, rats with a caloric intake four times higher than their counterparts (via fructose-rich Coca Cola) maintained almost identical weight and blood glucose levels.[67]
With all this in mind, it’s clear that macronutrient ratios matter a lot.
CICO is a tool—not a religion
A large part of this conversation is ideological: we have seen what the body positivity movement has done to men and women. We have seen gluttony and shamelessness, and we are rightfully disgusted.
But we have also seen the “edtwt” (eating disorder Twitter) and “proana” (promotion of anorexia) movements. We have seen women eating 700 calories a day and ballooning when they eat a normal-sized meal, reinforcing their unhealthy relationship with food. Because metabolism underpins every crucial bodily process, and because this constant starvation wrecks metabolism, these women are destined for hormonal issues, chronic health issues, autoimmune issues, and frailty. No woman eating so little can age gracefully, and no woman eating so little can remain in good health after the production of youth-associated hormones drops off in their mid-twenties.
Both the body positivity and the eating disorder groups greatly misunderstand metabolism and are casualties of CICO dogma.
Furthermore, there are many adults who are tracking calories, remaining active, and trying to lose weight while still failing. They are not anomalies. Like the previously mentioned groups, they are simply looking at the problem the wrong way.
Metabolism declines with age due to declining thyroid production, and aging is accelerated when production of hormones that protect against cortisol and estrogen decline alongside it. Aging and disease are the same process, accelerated greatly by damaged mitochondria.[68] Almost every overweight adult is somewhere on the spectrum of hypothyroidism.
“Mitochondria produce cellular energy in the human body, and energy availability is the lowest common denominator needed for the functioning of all biological systems.”
—David C. Geary, PhD
A large part of this conversation is ideological: we have seen what the body positivity movement has done to men and women. We have seen gluttony and shamelessness, and we are rightfully disgusted.
But we have also seen the “edtwt” (eating disorder Twitter) and “proana” (promotion of anorexia) movements. We have seen women eating 700 calories a day and ballooning when they eat a normal-sized meal, reinforcing their unhealthy relationship with food. Because metabolism underpins every crucial bodily process, and because this constant starvation wrecks metabolism, these women are destined for hormonal issues, chronic health issues, autoimmune issues, and frailty. No woman eating so little can age gracefully, and no woman eating so little can remain in good health after the production of youth-associated hormones drops off in their mid-twenties.
Both the body positivity and the eating disorder groups greatly misunderstand metabolism and are casualties of CICO dogma.
Furthermore, there are many adults who are tracking calories, remaining active, and trying to lose weight while still failing. They are not anomalies. Like the previously mentioned groups, they are simply looking at the problem the wrong way.
Metabolism declines with age due to declining thyroid production, and aging is accelerated when production of hormones that protect against cortisol and estrogen decline alongside it. Aging and disease are the same process, accelerated greatly by damaged mitochondria.[68] Almost every overweight adult is somewhere on the spectrum of hypothyroidism.
“Mitochondria produce cellular energy in the human body, and energy availability is the lowest common denominator needed for the functioning of all biological systems.”
—David C. Geary, PhD

Calories out: compromised by hypothyroidism?
Hypothyroidism used to be diagnosed by symptoms and thus had an estimated prevalence of 40% in the '40s and '50s—when we were skinny—but it is now estimated that only 5% of the population is hypothyroid.
That’s not because we got healthier—in fact, we're sicker by just about every meaningful metric now.[69][70][71][72][73][74][75][76][77] That changed because of a faulty test called the protein-bound iodine (PBI) test and was amplified by pharmaceutical companies when levothyroxine (T4 monotherapy as opposed to a T3:T4 mixture) became the preferred thyroid supplement for those "rare" hypothyroid patients.
In the ‘60s, it was found that the PBI test had little to do with thyroid health, yet this pernicious idea that "only 5% of people are hypothyroid" persisted. In fact, we took this new 5% figure and retroactively widened the “normal” ranges in our thyroid bloodwork.
As Ray Peat points out, if we took any other biomarker and gave it as wide a range as we give TSH (an indicator of thyroid status), we would have "normal" blood sugar levels ranging from the level at which we see convulsion and death into the low-diabetic range... and we'd call that "normal". We'd have the low cholesterol ranges associated with cancer and strokes or levels as high as 400 mg... and we'd call that "normal" too.
Blood biomarkers are merely a glimpse into what's going on in the body—they fail to indicate what's happening at the cellular or tissue level. Making simple bloodwork the end-all-be-all is myopic and naive.
Most people see declining metabolic rate as inevitable, bound only to age. That’s the impression you would be left with if you internalized mainstream medicine’s view of pathophysiology. Metabolism is highly variable. A decent nutritionist—even one operating under an outdated mainstream paradigm—recognizes this basic concept as "metabolic age".
Of course one will lose weight eating at a deficit, and of course people who starve themselves can stay skinny for a long time—nobody in their right mind would dispute this. But eating at too great a deficit compensatorily slows metabolism, and intentionally slowing metabolism will negatively impact health. The metabolic conditions brought about by starvation are unsustainable and eventually lead to disastrous results.
Hypothyroidism used to be diagnosed by symptoms and thus had an estimated prevalence of 40% in the '40s and '50s—when we were skinny—but it is now estimated that only 5% of the population is hypothyroid.
That’s not because we got healthier—in fact, we're sicker by just about every meaningful metric now.[69][70][71][72][73][74][75][76][77] That changed because of a faulty test called the protein-bound iodine (PBI) test and was amplified by pharmaceutical companies when levothyroxine (T4 monotherapy as opposed to a T3:T4 mixture) became the preferred thyroid supplement for those "rare" hypothyroid patients.
In the ‘60s, it was found that the PBI test had little to do with thyroid health, yet this pernicious idea that "only 5% of people are hypothyroid" persisted. In fact, we took this new 5% figure and retroactively widened the “normal” ranges in our thyroid bloodwork.
As Ray Peat points out, if we took any other biomarker and gave it as wide a range as we give TSH (an indicator of thyroid status), we would have "normal" blood sugar levels ranging from the level at which we see convulsion and death into the low-diabetic range... and we'd call that "normal". We'd have the low cholesterol ranges associated with cancer and strokes or levels as high as 400 mg... and we'd call that "normal" too.
Blood biomarkers are merely a glimpse into what's going on in the body—they fail to indicate what's happening at the cellular or tissue level. Making simple bloodwork the end-all-be-all is myopic and naive.
Most people see declining metabolic rate as inevitable, bound only to age. That’s the impression you would be left with if you internalized mainstream medicine’s view of pathophysiology. Metabolism is highly variable. A decent nutritionist—even one operating under an outdated mainstream paradigm—recognizes this basic concept as "metabolic age".
Of course one will lose weight eating at a deficit, and of course people who starve themselves can stay skinny for a long time—nobody in their right mind would dispute this. But eating at too great a deficit compensatorily slows metabolism, and intentionally slowing metabolism will negatively impact health. The metabolic conditions brought about by starvation are unsustainable and eventually lead to disastrous results.
Opportunities for derangements in energy metabolism
● Inhibition of pyruvate dehydrogenase by PDK (as seen in the Randle cycle), blocking entry into the Krebs cycle
● Low NAD+/NADH ratio causing lactate dehydrogenase to convert pyruvate to lactate
● α-Ketoglutarate dehydrogenase in the Krebs cycle inhibition by excessive NADH in relation to NAD+
● Complex I of the electron transport chain inhibition by prescription drugs such as Metformin, Haloperidol, and Clofibrate
● Complex III of the electron transport chain inhibition by Acetaminophen
● Oxygen availability: as the terminal acceptor (the final place electrons go), oxygen availability is crucial if we want to derive the maximum amount of ATP per molecule of fuel substrate
This list is far from exhaustive, but it’s meant to demonstrate that there is a lot that can go wrong in deriving energy from food.
For more information on oxidative metabolism, I have a thread you can check out here:
x.com/takethiamine/s…
● Inhibition of pyruvate dehydrogenase by PDK (as seen in the Randle cycle), blocking entry into the Krebs cycle
● Low NAD+/NADH ratio causing lactate dehydrogenase to convert pyruvate to lactate
● α-Ketoglutarate dehydrogenase in the Krebs cycle inhibition by excessive NADH in relation to NAD+
● Complex I of the electron transport chain inhibition by prescription drugs such as Metformin, Haloperidol, and Clofibrate
● Complex III of the electron transport chain inhibition by Acetaminophen
● Oxygen availability: as the terminal acceptor (the final place electrons go), oxygen availability is crucial if we want to derive the maximum amount of ATP per molecule of fuel substrate
This list is far from exhaustive, but it’s meant to demonstrate that there is a lot that can go wrong in deriving energy from food.
For more information on oxidative metabolism, I have a thread you can check out here:
x.com/takethiamine/s…
Increasing metabolism
● PUFA intake as close to 0 as possible
● Avoid the “macronutrient swampland” (opt for higher carb than fat but don’t force it)
● Address thyroid health (this does not mean recklessly taking thyroid products without adequate research)[78]
● Fix circadian rhythm
● Strength training (but not intense cardio)
● All 8 B vitamins in the diet, if not, consider improving diet or supplementing
● B1
● B3
● Baking soda
● Caffeine
● Sodium
● Magnesium
● Calcium
● Potassium
● Zinc
● Copper
● Vitamin A* (do not supplement if you have a sluggish liver or are hypothyroid)
● Vitamin D3
● Vitamin E
● Vitamin K2
● Glucose
● Fructose
● Sucrose
● Gelatin
● Restriction of BCAAs (leucine, isoleucine, and valine)
● Restriction of inflammatory amino acids (methionine, cysteine, and tryptophan)
● Saturated fats (coconut oil especially)
● Red light
● CO2
● Aspirin
● Pregnenolone
● Progesterone
● DHEA (no more than 5 mg at a time as DHEA easily aromatizes)
Identifying unique metabolic bottlenecks using tests
● Whole genome sequencing
● Mitoswab Plus test
● Mosaic Diagnostics organic acids test
● Plasma amino acids
Ratios indicative of metabolic rate
● Acetoacetate/beta-hydroxybutyrate
● Lactate/pyruvate
● Oxidized/reduced glutathione
● Cortisol/cortisone
● Estrone/estradiol
● NAD+/NADH
Additional useful biomarkers
● TSH
● Total cholesterol
● Prolactin
● Vitamin D
● PTH
● rT3
● Serum phosphorus
● Pulse (70-85 bpm)
● Underarm temperature (minimum 97.8°F waking, reaching or exceeding 98.6°F midday)
● Achilles reflex test[79]
● Blood sugar (waking and postprandial)
● Lactic acid (you can buy a lactate meter for home use)[80]
● PUFA intake as close to 0 as possible
● Avoid the “macronutrient swampland” (opt for higher carb than fat but don’t force it)
● Address thyroid health (this does not mean recklessly taking thyroid products without adequate research)[78]
● Fix circadian rhythm
● Strength training (but not intense cardio)
● All 8 B vitamins in the diet, if not, consider improving diet or supplementing
● B1
● B3
● Baking soda
● Caffeine
● Sodium
● Magnesium
● Calcium
● Potassium
● Zinc
● Copper
● Vitamin A* (do not supplement if you have a sluggish liver or are hypothyroid)
● Vitamin D3
● Vitamin E
● Vitamin K2
● Glucose
● Fructose
● Sucrose
● Gelatin
● Restriction of BCAAs (leucine, isoleucine, and valine)
● Restriction of inflammatory amino acids (methionine, cysteine, and tryptophan)
● Saturated fats (coconut oil especially)
● Red light
● CO2
● Aspirin
● Pregnenolone
● Progesterone
● DHEA (no more than 5 mg at a time as DHEA easily aromatizes)
Identifying unique metabolic bottlenecks using tests
● Whole genome sequencing
● Mitoswab Plus test
● Mosaic Diagnostics organic acids test
● Plasma amino acids
Ratios indicative of metabolic rate
● Acetoacetate/beta-hydroxybutyrate
● Lactate/pyruvate
● Oxidized/reduced glutathione
● Cortisol/cortisone
● Estrone/estradiol
● NAD+/NADH
Additional useful biomarkers
● TSH
● Total cholesterol
● Prolactin
● Vitamin D
● PTH
● rT3
● Serum phosphorus
● Pulse (70-85 bpm)
● Underarm temperature (minimum 97.8°F waking, reaching or exceeding 98.6°F midday)
● Achilles reflex test[79]
● Blood sugar (waking and postprandial)
● Lactic acid (you can buy a lactate meter for home use)[80]
Special thanks to
@BradCohn
@Peatpill
@ImPeating314
@EndoMedChem
@nobody97799851
@stag________
@lowmegatron
@Glace__
@NangaParbat1618
@bioenergy_space
@Outdoctrination
@dannyroddy
@BradCohn
@Peatpill
@ImPeating314
@EndoMedChem
@nobody97799851
@stag________
@lowmegatron
@Glace__
@NangaParbat1618
@bioenergy_space
@Outdoctrination
@dannyroddy

• • •
Missing some Tweet in this thread? You can try to
force a refresh