COVID VACCINE ELIGIBILITY 🇬🇧,
a thread🧵
JCVI have just advised that, going forwards, eligibility for Covid vaccination will be even more tightly restricted.
But the ‘bespoke cost-effectiveness assessment’ upon which this is based is heavily flawed…
gov.uk/government/pub…
a thread🧵
JCVI have just advised that, going forwards, eligibility for Covid vaccination will be even more tightly restricted.
But the ‘bespoke cost-effectiveness assessment’ upon which this is based is heavily flawed…
gov.uk/government/pub…

Before I dive into the issues, let’s just recap where we are…
In the UK, if you’re under 65 and not ‘at risk’, the last time you were eligible for a Covid vaccination was 2 years ago (Autumn 2022).
For most under 50s, it’s been 3 years since you were eligible (Autumn 2021).
In the UK, if you’re under 65 and not ‘at risk’, the last time you were eligible for a Covid vaccination was 2 years ago (Autumn 2022).
For most under 50s, it’s been 3 years since you were eligible (Autumn 2021).

Meanwhile, in many other countries, the entire population is given A CHOICE.
Their governments recommend that certain risk groups should get vaccinated…
…but even outside these risk groups, ANYONE who wants to get vaccinated, can be as part of their national vax programme.
Their governments recommend that certain risk groups should get vaccinated…
…but even outside these risk groups, ANYONE who wants to get vaccinated, can be as part of their national vax programme.

Ok, now let’s review all the reasons why the cost-effectiveness analysis (which has NOT been peer reviewed) is flawed.
There are 4 main issues:
1️⃣ The analysis *only* considered hospital & ICU admissions and deaths using reported data from 2023/24.
medrxiv.org/content/10.110…
There are 4 main issues:
1️⃣ The analysis *only* considered hospital & ICU admissions and deaths using reported data from 2023/24.
medrxiv.org/content/10.110…

So why is this a problem?
For starters, Covid hospital data is now significantly under-reported.
Since April 2023, most patients with Covid symptoms are no longer tested to confirm if they have Covid, unless they are eligible for antiviral treatment…
gov.uk/guidance/covid…
For starters, Covid hospital data is now significantly under-reported.
Since April 2023, most patients with Covid symptoms are no longer tested to confirm if they have Covid, unless they are eligible for antiviral treatment…
gov.uk/guidance/covid…

…and if they aren’t tested, then the hospital admission is not recorded as being a *Covid* hospitalisation.
Even the experts at UKHSA agree that changes in hospital testing policy in April 2023 had a significant impact on hospitalisation numbers.
Even the experts at UKHSA agree that changes in hospital testing policy in April 2023 had a significant impact on hospitalisation numbers.
https://twitter.com/kallmemeg/status/1709907814573895945

The chart below from @jneill clearly illustrates just how much Covid testing has reduced over the last 2 years.
Hundreds of thousands of PCR tests used to be performed every single day. Now we’re down to a teeny tiny fraction of that.
Hundreds of thousands of PCR tests used to be performed every single day. Now we’re down to a teeny tiny fraction of that.

Of course, this lack of testing impacts the death records too.
Here’s an example of data from just one week in late September.
12.8% of all deaths involved flu or pneumonia…
…but the ARI data shows us there was practically no flu at that time, but a LOT of Covid (in purple).
Here’s an example of data from just one week in late September.
12.8% of all deaths involved flu or pneumonia…
…but the ARI data shows us there was practically no flu at that time, but a LOT of Covid (in purple).

Now let’s look at excess deaths…
Overall excess deaths across ALL age groups are heavily skewed by older ages (who are more likely to die)…
…but when we zoom in on the data for younger (UNVACCINATED) age groups, the mortality rate is HIGHER than any recent pre-pandemic year.
Overall excess deaths across ALL age groups are heavily skewed by older ages (who are more likely to die)…
…but when we zoom in on the data for younger (UNVACCINATED) age groups, the mortality rate is HIGHER than any recent pre-pandemic year.
https://twitter.com/actuarybyday/status/1844277004973244755

It’s clear that Covid hospitalisations and Covid deaths are under-reported since the change in testing protocols…
…so if you’re using these figures to calculate how many hospitalisations & deaths would be averted by vaccination, then these numbers will be under-estimated also.
…so if you’re using these figures to calculate how many hospitalisations & deaths would be averted by vaccination, then these numbers will be under-estimated also.
2️⃣ The next issue is that the cost-effectiveness analysis ignores any deaths linked to post-infection sequelae.
As this article by @BawdenTom explains, the risk of having a heart attack or stroke increases significantly for 3 years after Covid infection.
inews.co.uk/news/science/h…
As this article by @BawdenTom explains, the risk of having a heart attack or stroke increases significantly for 3 years after Covid infection.
inews.co.uk/news/science/h…

Another study examined data from 4.6m adults in England and found that incidence of heart attacks & strokes was LOWER after Covid vaccination compared to those who had not been vaxxed.
This benefit is not included in the cost-effectiveness analysis.
cam.ac.uk/research/news/…
This benefit is not included in the cost-effectiveness analysis.
cam.ac.uk/research/news/…

But this is only the tip of the iceberg...
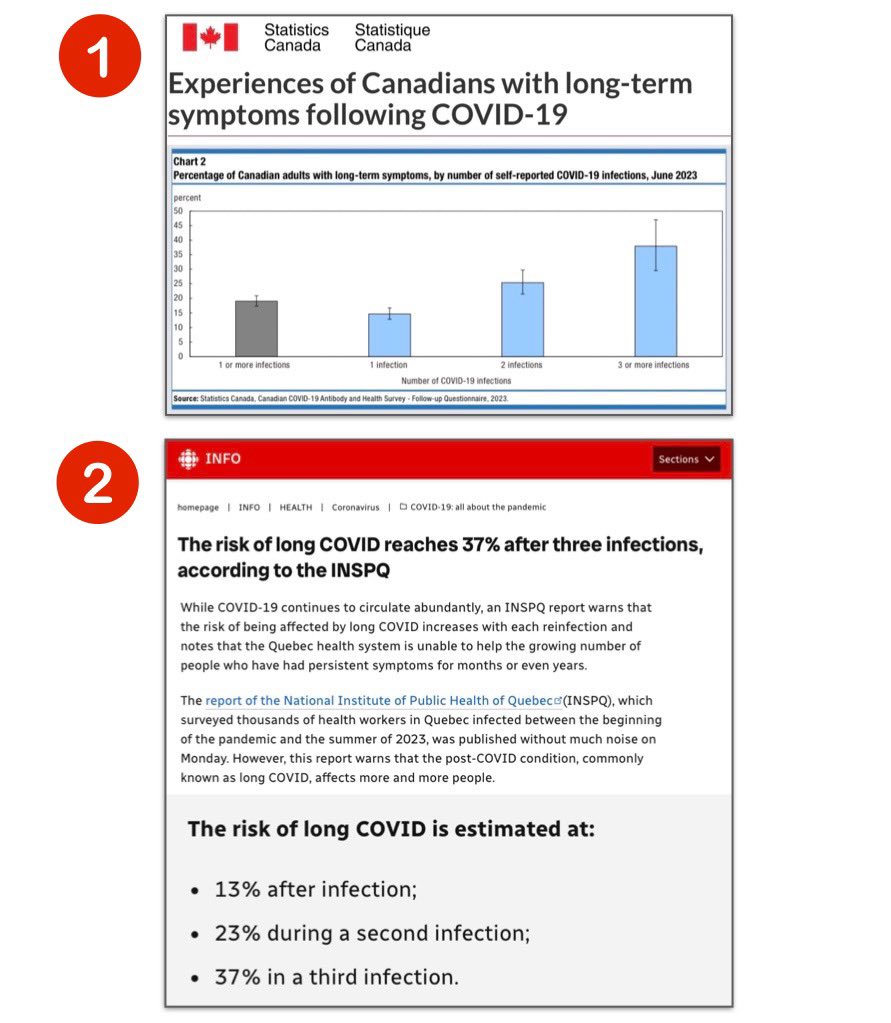
3️⃣ The BIGGEST risk for younger people is long-term chronic illness.
The latest data from the GP-Patient Survey (July 2024) shows that 4.6% of the population now have LONG COVID.
That equates to 3.1 MILLION people across the UK!
3️⃣ The BIGGEST risk for younger people is long-term chronic illness.
The latest data from the GP-Patient Survey (July 2024) shows that 4.6% of the population now have LONG COVID.
That equates to 3.1 MILLION people across the UK!

According to the latest ONS Covid Infection Survey (March 2024), 29% of those currently suffering from Long Covid reported that their symptoms started within the last 12 months.
In other words, nearly A THIRD of people suffering from Long Covid are NEW cases since March 2023.
In other words, nearly A THIRD of people suffering from Long Covid are NEW cases since March 2023.

We also know that incidence of Long Covid is far higher in the middle age groups, particularly 45 to 64 year olds.
This age group are NOT eligible for vaccination.
(Source: ONS Survey, March 2024)
ons.gov.uk/peoplepopulati…
This age group are NOT eligible for vaccination.
(Source: ONS Survey, March 2024)
ons.gov.uk/peoplepopulati…

This high prevalence of Long Covid is having a major impact on the workforce, and in turn, the economy.
The UK LOCOMOTION study revealed that OVER HALF of those with Long Covid had been forced to reduce their working hours or stop working altogether.
evidence.nihr.ac.uk/alert/how-much…
The UK LOCOMOTION study revealed that OVER HALF of those with Long Covid had been forced to reduce their working hours or stop working altogether.
evidence.nihr.ac.uk/alert/how-much…

And this report published by @TheEconomist estimated that 252 MILLION work hours may be lost due to Long Covid in 2024.
The economic cost resulting from this is estimated to be over US$15.5 BILLION, equivalent to 0.5% of UK’s GDP.
impact.economist.com/perspectives/h…
The economic cost resulting from this is estimated to be over US$15.5 BILLION, equivalent to 0.5% of UK’s GDP.
impact.economist.com/perspectives/h…

Many studies have shown that recent vaccination DRAMATICALLY reduces the risk of developing Long Covid.
Given the clear economic impacts of LC, it seems incredible that the vaccine cost-effectiveness analysis doesn’t take this aspect into account at all.
scientificamerican.com/article/vaccin…
Given the clear economic impacts of LC, it seems incredible that the vaccine cost-effectiveness analysis doesn’t take this aspect into account at all.
scientificamerican.com/article/vaccin…

Another recent study revealed that the risk of developing Long Covid is DOUBLED for those who have NOT been vaccinated compared to those who have been vaccinated.
nejm.org/doi/full/10.10… x.com/zalaly/status/…
nejm.org/doi/full/10.10… x.com/zalaly/status/…

4️⃣ But it’s not just chronic illness that’s a problem.
Short-term illness (not severe enough to require hospital) is another important consideration since this can cause significant disruption to workplaces.
Covid is not seasonal. It comes in repeated waves throughout the year.
Short-term illness (not severe enough to require hospital) is another important consideration since this can cause significant disruption to workplaces.
Covid is not seasonal. It comes in repeated waves throughout the year.

This article from @andrewgregory reveals how the cost of workplace illness has risen by 41% to £103 BILLION in 2023 (up from £73bn in 2018), according to the IPPR.
This was largely due to a loss of productivity amid “staggering” levels of presenteeism.
amp.theguardian.com/society/articl…
This was largely due to a loss of productivity amid “staggering” levels of presenteeism.
amp.theguardian.com/society/articl…

You can read the full IPPR report at the link below.
This report clearly shows how the increased level of illness amongst employees is having a HUGE cost to businesses.
And the majority of this cost is caused by employees attempting to work when sick.
ippr-org.files.svdcdn.com/production/Dow…
This report clearly shows how the increased level of illness amongst employees is having a HUGE cost to businesses.
And the majority of this cost is caused by employees attempting to work when sick.
ippr-org.files.svdcdn.com/production/Dow…

As a result of this flawed cost-effectiveness analysis (which excluded many of the primary benefits of vaccination), the numbers are VASTLY under-estimated.
This is why the vaccine eligibility has been so tightly restricted to only those aged 75 and over (or immunocompromised).
This is why the vaccine eligibility has been so tightly restricted to only those aged 75 and over (or immunocompromised).

The really interesting thing is that ANOTHER vaccine cost-effectiveness analysis has recently been performed which DID look at some of these additional factors for the UK.
This study was recently published in the Journal of Medical Economics.
tandfonline.com/doi/full/10.10…
This study was recently published in the Journal of Medical Economics.
tandfonline.com/doi/full/10.10…

Unsurprisingly, this alternative analysis which INCLUDED benefits for averting Long Covid reached a VERY different conclusion:
Expanding vaccine eligibility to all over 50s increases the total cost of vaccination, but REMAINS cost-effective with an ICER of £10,061/QALY gained.
Expanding vaccine eligibility to all over 50s increases the total cost of vaccination, but REMAINS cost-effective with an ICER of £10,061/QALY gained.

Some of my followers may recall that I conducted a detailed forensic analysis of the Covid vaccine ‘bespoke non-standard cost-effectiveness assessment’ methodology when it was first published just over a year ago.
You can have a read of my analysis in the thread below ⬇️
You can have a read of my analysis in the thread below ⬇️
https://twitter.com/_catinthehat/status/1725575757647200639
Finally, I wanted to show a side-by-side analysis of Covid vaccine eligibility in Autumn 2022 vs Autumn 2025…
It seems crazy that even those who are clinically vulnerable will no longer be eligible for protection from a Covid booster, unless they are immunosuppressed.
It seems crazy that even those who are clinically vulnerable will no longer be eligible for protection from a Covid booster, unless they are immunosuppressed.

Here’s a comparison of the vaccine eligibility for Covid vs Flu.
The criteria is vastly different!
Too many differences to list them all, but children, clinically vulnerable people & healthcare workers are all eligible for the flu jab - but won’t be able to get a Covid booster.
The criteria is vastly different!
Too many differences to list them all, but children, clinically vulnerable people & healthcare workers are all eligible for the flu jab - but won’t be able to get a Covid booster.

So what can you do about this?
I would recommend writing to your local MP and ask them to raise concerns with the Minister for Public Health & Prevention who is responsible for vaccine policy (@GwynneMP).
Below is an excellent letter example written by @GillianSmith16 ⬇️
I would recommend writing to your local MP and ask them to raise concerns with the Minister for Public Health & Prevention who is responsible for vaccine policy (@GwynneMP).
Below is an excellent letter example written by @GillianSmith16 ⬇️
https://twitter.com/gilliansmith16/status/1857040216432706014

@GwynneMP @GillianSmith16 You can find details about how to get in touch with your local MP here ⬇️
parliament.uk/get-involved/c…
parliament.uk/get-involved/c…
• • •
Missing some Tweet in this thread? You can try to
force a refresh