My approach to fixing dysautonomia post-COVID/ mRNA shots🧵
Targeting the CHOLINERGIC system with 3 therapeutic agents
Autonomic nervous system dysfunction is extremely common in this cohort - especially after mRNA.
4 years on - A lot of people are still sick, and dysautonomia can can account for many (if not all) of the symptoms
Targeting the CHOLINERGIC system with 3 therapeutic agents
Autonomic nervous system dysfunction is extremely common in this cohort - especially after mRNA.
4 years on - A lot of people are still sick, and dysautonomia can can account for many (if not all) of the symptoms

Spike protein binds nicotinic acetylcholine receptors and triggers degeneration of cholinergic neurons
Spike also impairs the production of acetylcholine in said neurons.
Without acetycholine, the nervous system begins to malfunction
Spike also impairs the production of acetylcholine in said neurons.
Without acetycholine, the nervous system begins to malfunction

This cholinergic deficit is thought to play major roles in the cognitive impairment, memory loss, and widespread symptoms

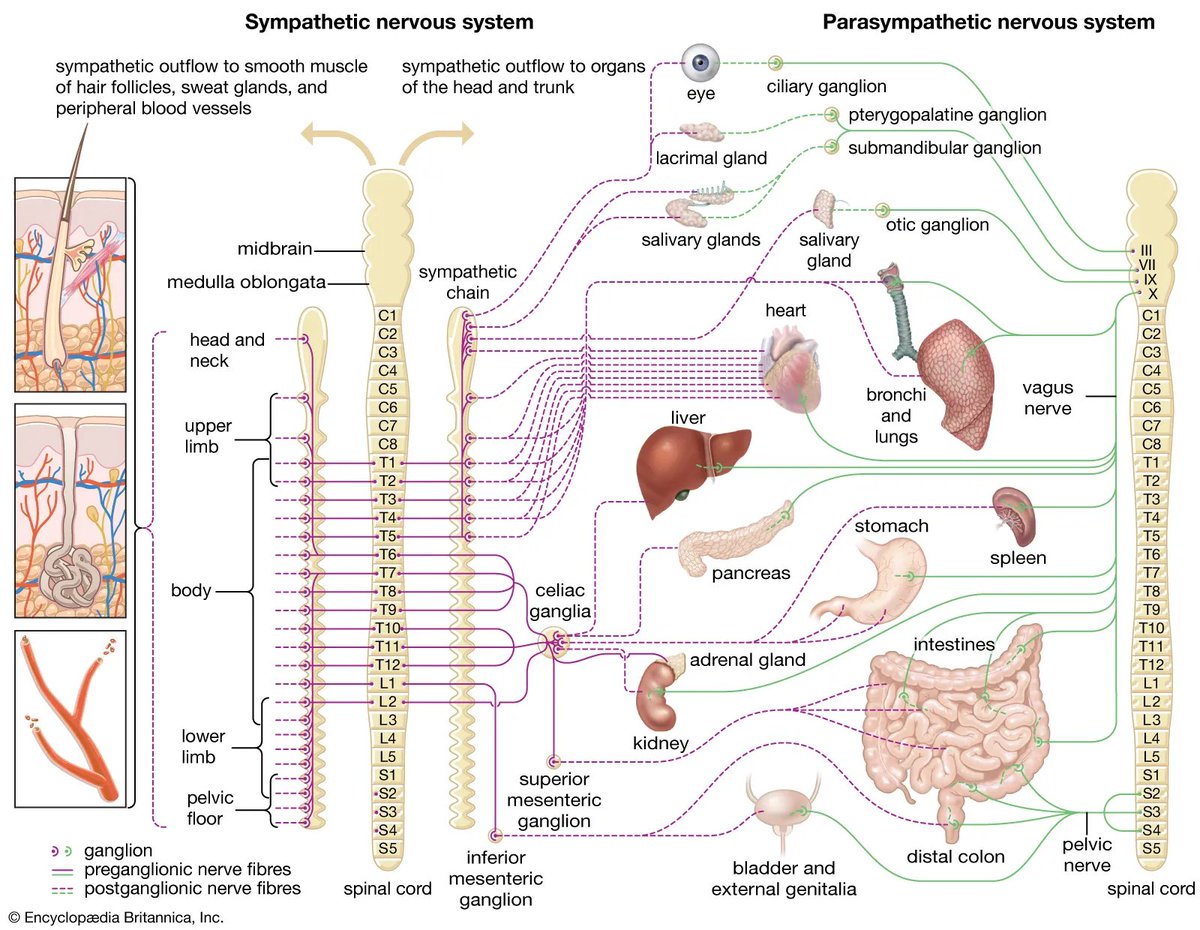
One of the body's main tools for calming inflammation is via the vagus nerve...
Which also requires acetylcholine.
This is called the "cholinergic anti-inflammatory pathway", and when it falters, the body is faced with unrelenting systemic inflammation
Which also requires acetylcholine.
This is called the "cholinergic anti-inflammatory pathway", and when it falters, the body is faced with unrelenting systemic inflammation

Studies have shown substantial overlap in the pathophysiological mechanisms of COVID-19/vaccine injury and...
Alzheimer's Disease & Parkinsons
Both of which involve impairment of the cholinergic system
Take home: spike protein leads to neurodegeneration
Alzheimer's Disease & Parkinsons
Both of which involve impairment of the cholinergic system
Take home: spike protein leads to neurodegeneration
Therapeutic agent #1: NICOTINE
Most probably know of it's use in long COVID. It's old news.
Fortunately, due to high affinity with nicotinic ACh receptors, exogenous nicotine can displace spike protein
Nicotine essentially "mimics" acetylcholine.
In doing so, it restores cholinergic output
Most probably know of it's use in long COVID. It's old news.
Fortunately, due to high affinity with nicotinic ACh receptors, exogenous nicotine can displace spike protein
Nicotine essentially "mimics" acetylcholine.
In doing so, it restores cholinergic output

Just so you know, this is a brief summary of a lecture I am giving in Florida at a conference on December 13-15th
If your in the area, you can check it out here:
qntacademy.com/quantum-leap-1
If your in the area, you can check it out here:
qntacademy.com/quantum-leap-1
It is no coincidence that smoking is considered substantially protective against parkinson's disease.
Nicotine also has great utility in Alzheimer's disease
Nicotine also has great utility in Alzheimer's disease

The second therapeutic agent approaches the problem from a different angle:
Stimulating production of acetylcholine within the neuron itself.
Enter... Thiamine (Vitamin B1)
In many respects, thiamine is THE most important nutrient for the cholinergic system
Stimulating production of acetylcholine within the neuron itself.
Enter... Thiamine (Vitamin B1)
In many respects, thiamine is THE most important nutrient for the cholinergic system

Thiamine availability tracks closely with acetycholine production in neurons
Thiamine is needed to make the raw material
But aside from its metabolic role, thiamine is also involved in the release and utilization of ACh by neurons
Thiamine is needed to make the raw material
But aside from its metabolic role, thiamine is also involved in the release and utilization of ACh by neurons

High dose thiamine has put some patients with Parkinson's Disease into clinical remission, and is currently being trialled in Alzheimer's disease

I run a group on FB with over 11,000 members.
Many of them reversed long-COVID/post vaccine dysautonomia after my protocols which employ thiamine derivatives in high doses
Thiamine is my number 1 go-to therapy for ANY dysautonomia
Many of them reversed long-COVID/post vaccine dysautonomia after my protocols which employ thiamine derivatives in high doses
Thiamine is my number 1 go-to therapy for ANY dysautonomia

The third intervention approaches the problem from yet another angle:
Cleaning up the mess caused by chronic neuroinflammation
Therapeutic agent #3 : Plasmalogens
Cleaning up the mess caused by chronic neuroinflammation
Therapeutic agent #3 : Plasmalogens

In simple terms, plasmalogens are a specific type of lipid found in high concentrations in cell membrane
They can be depleted during states of inflammation.
They are being studied Alzheimer's disease and cognitive impairment
They can be depleted during states of inflammation.
They are being studied Alzheimer's disease and cognitive impairment

One theory states that under conditions of cholinergic impairment, cells may "autocanabilize" their own choline-plasmalogens to replenish choline

One thing is for sure...
Working via several different mechanisms, they can work wonders in any condition characterized by neuroinflammation.
Working via several different mechanisms, they can work wonders in any condition characterized by neuroinflammation.

In conclusion, this was a summary of my presentation on 3 therapeutic agents which can help to restore nervous system function in people suffering from post-COVID/vaccine dysautonomia
Rough dosage:
Thiamine (depending on the form used):
HCL form - 500-2000mg
TTFD - 200-500mg
Benfotiamine - 1,200-2000mg
Nicotine: It varies, but anywhere from 5mg-21mg patches, daily
Plasmalogens: Also varies on the form. Most people I know use marine-derived plasmalogens as low as 1-2mg per day. Other companies advocate for plasmalogen precursors, but have no experience with this so can't comment.
Rough dosage:
Thiamine (depending on the form used):
HCL form - 500-2000mg
TTFD - 200-500mg
Benfotiamine - 1,200-2000mg
Nicotine: It varies, but anywhere from 5mg-21mg patches, daily
Plasmalogens: Also varies on the form. Most people I know use marine-derived plasmalogens as low as 1-2mg per day. Other companies advocate for plasmalogen precursors, but have no experience with this so can't comment.

• • •
Missing some Tweet in this thread? You can try to
force a refresh