A few of the people who were involved in administering the government response to the pandemic really didn't like having to do it.
And they especially didn't like how so many officials would say one thing privately and one thing publicly.
So they kept notes.
And they especially didn't like how so many officials would say one thing privately and one thing publicly.
So they kept notes.
https://twitter.com/_CatintheHat/status/1860072299933892660
I've been sent quite a few of those notes in the last year, and the sad truth is that I just don't have time and energy to work through them all, but having seen those six videos from the UK Covid Inquiry, I feel the need to dig out one transcript that I've had for a while.
It's from a meeting between a load of representatives of healthcare professionals, and policymakers working for various government departments who were making choices about the pandemic response.
As I understand it, the meeting happened somewhere at the start of June 2021.
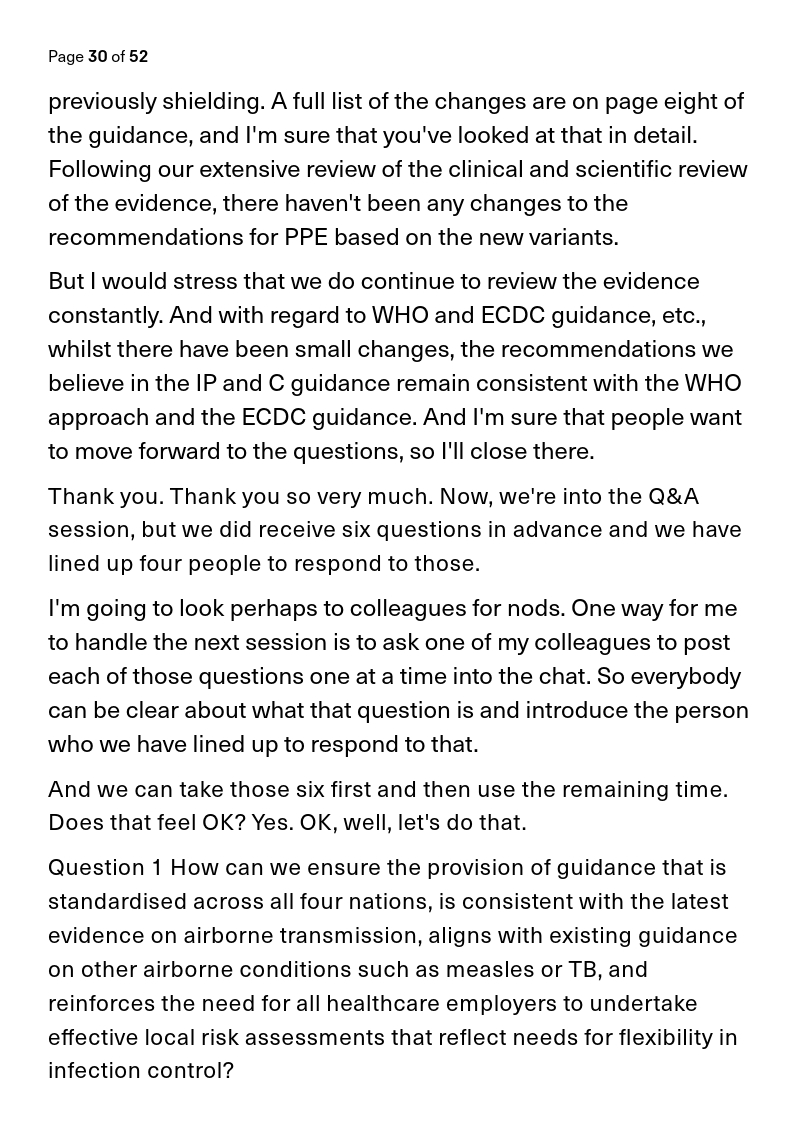
It starts with an appeal by healthcare workers for better practice and guidance on protective equipment based on the airborne nature of Covid.
And then it ends with them getting fobbed off, ignored, belittled, gaslighted, undermined, and dismissed by the people leading the government response.
It's really something.
I don't have time to go into this in depth, I'm in a really busy week, but I'll try to make a few notes as I go.
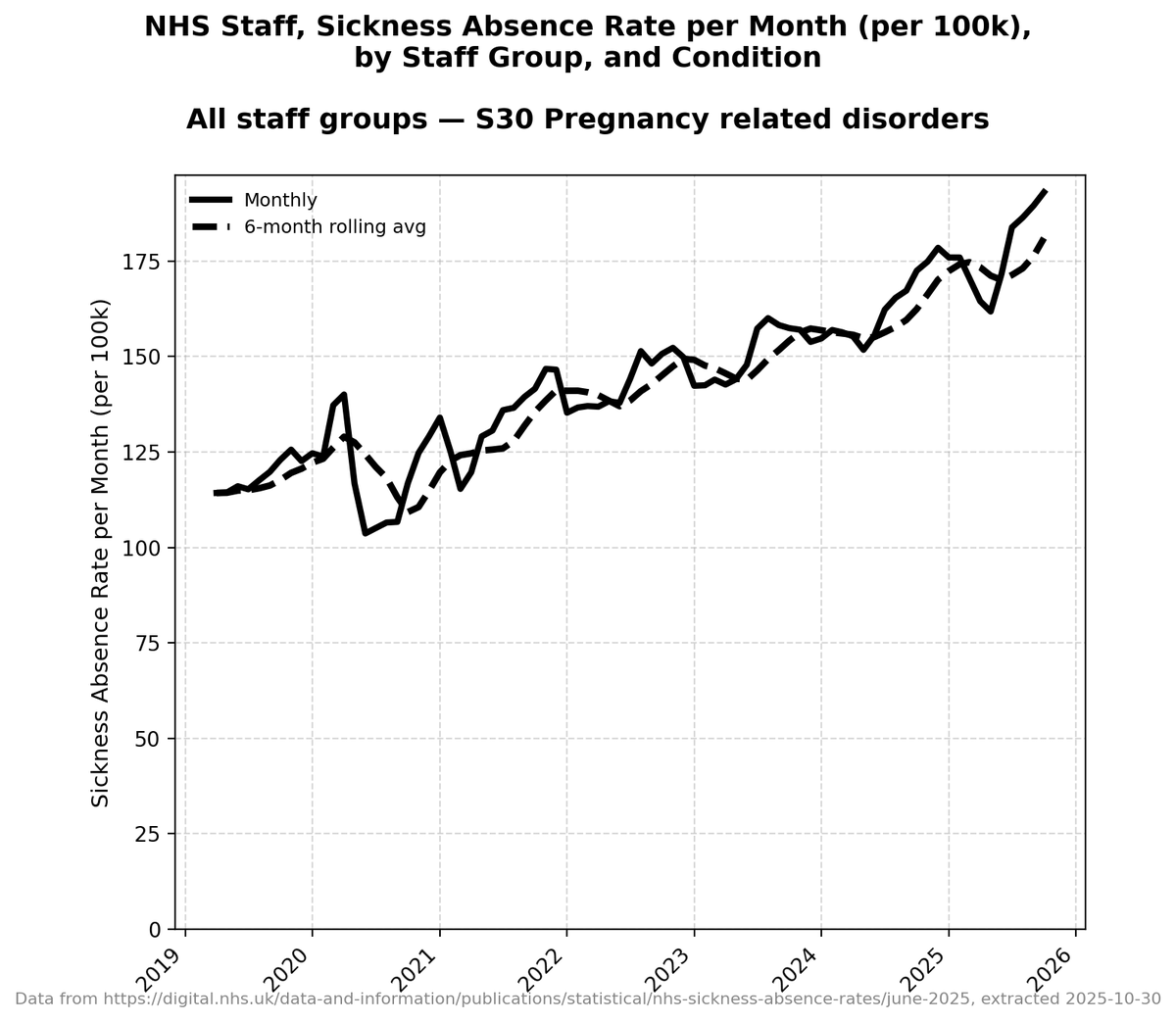
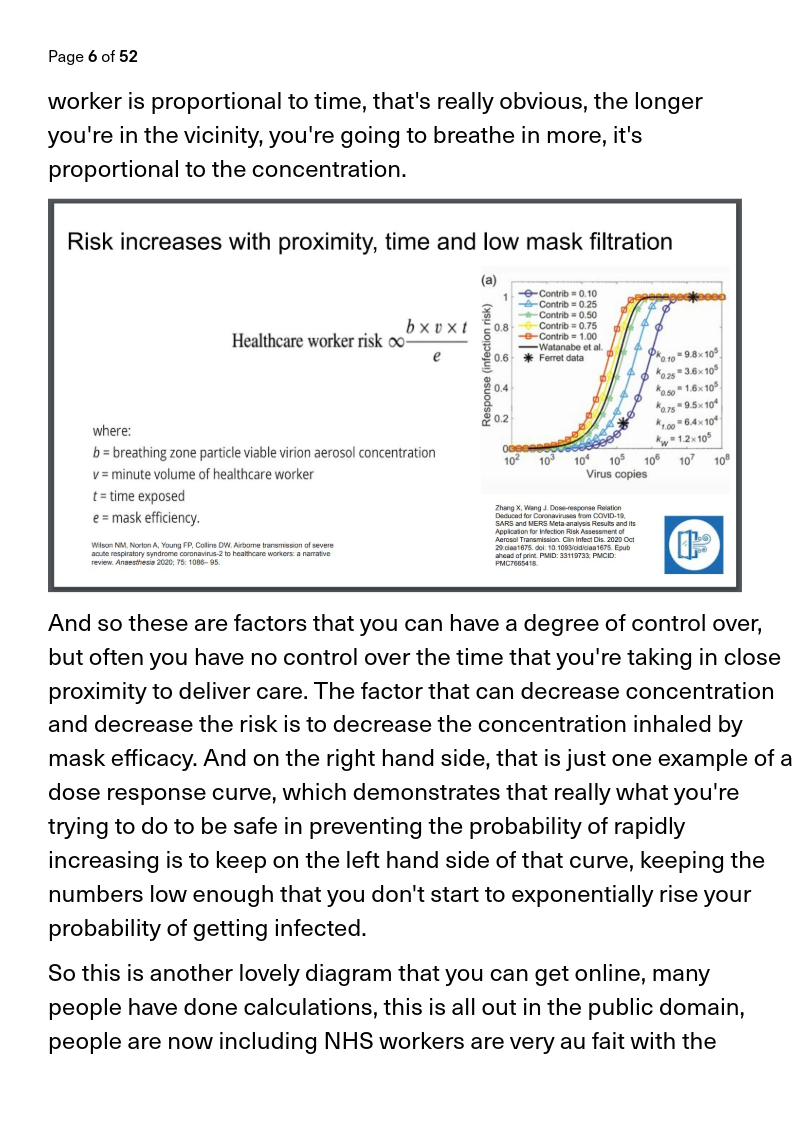
It starts off with the leads of several groups of healthcare professionals laying out the problem, airborne transmission, how it works, and how it is affecting NHS staff. 


They go into a lot of brilliant detail.
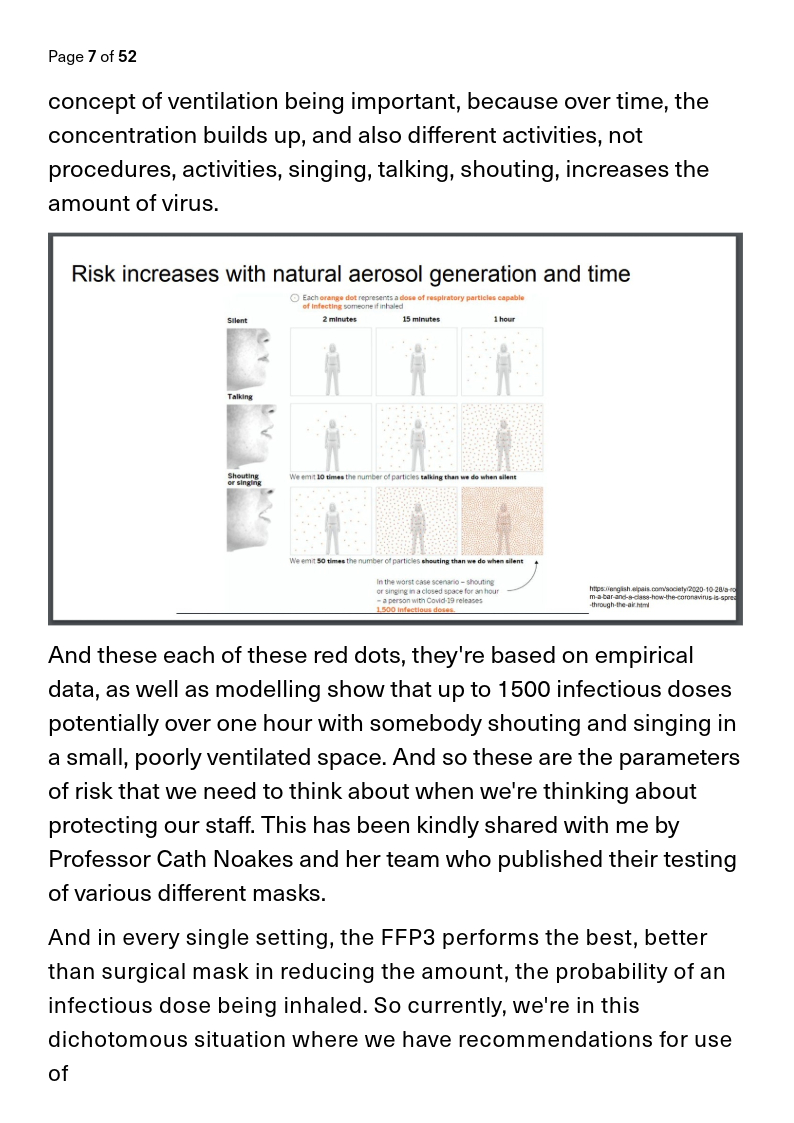
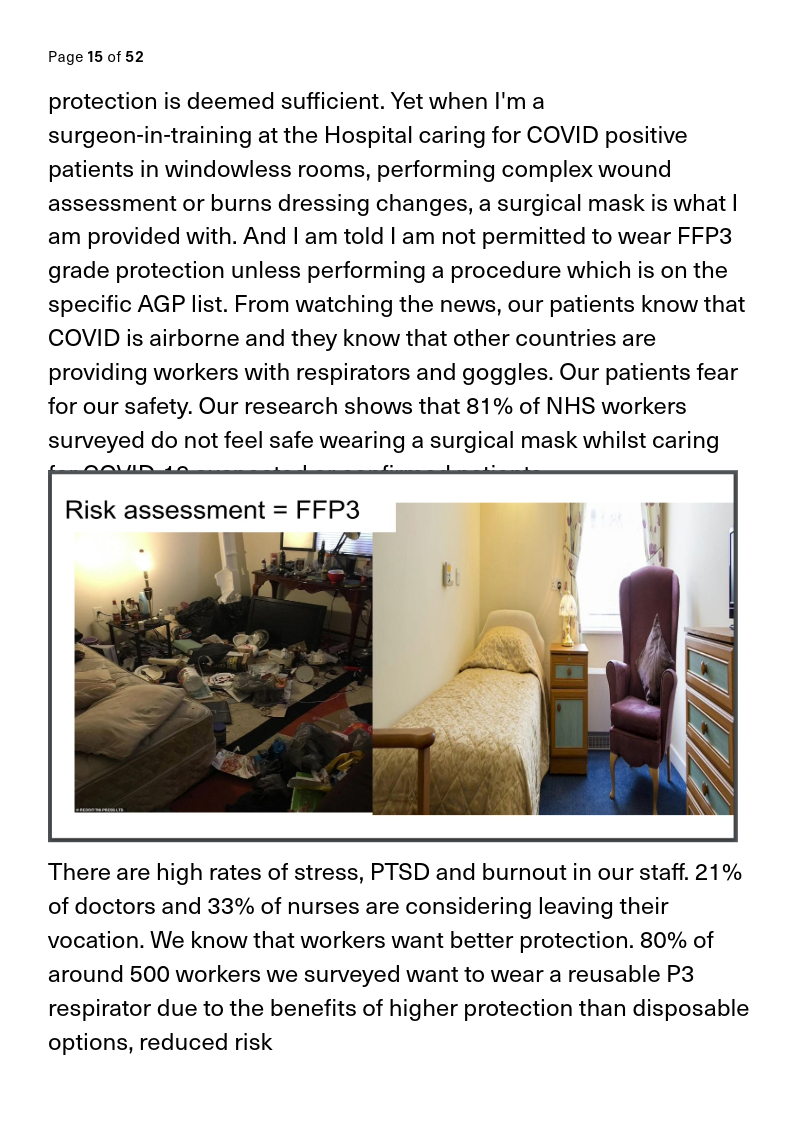
And they explain how it's relevant to people in different situations. Like paramedics going to scary situations.

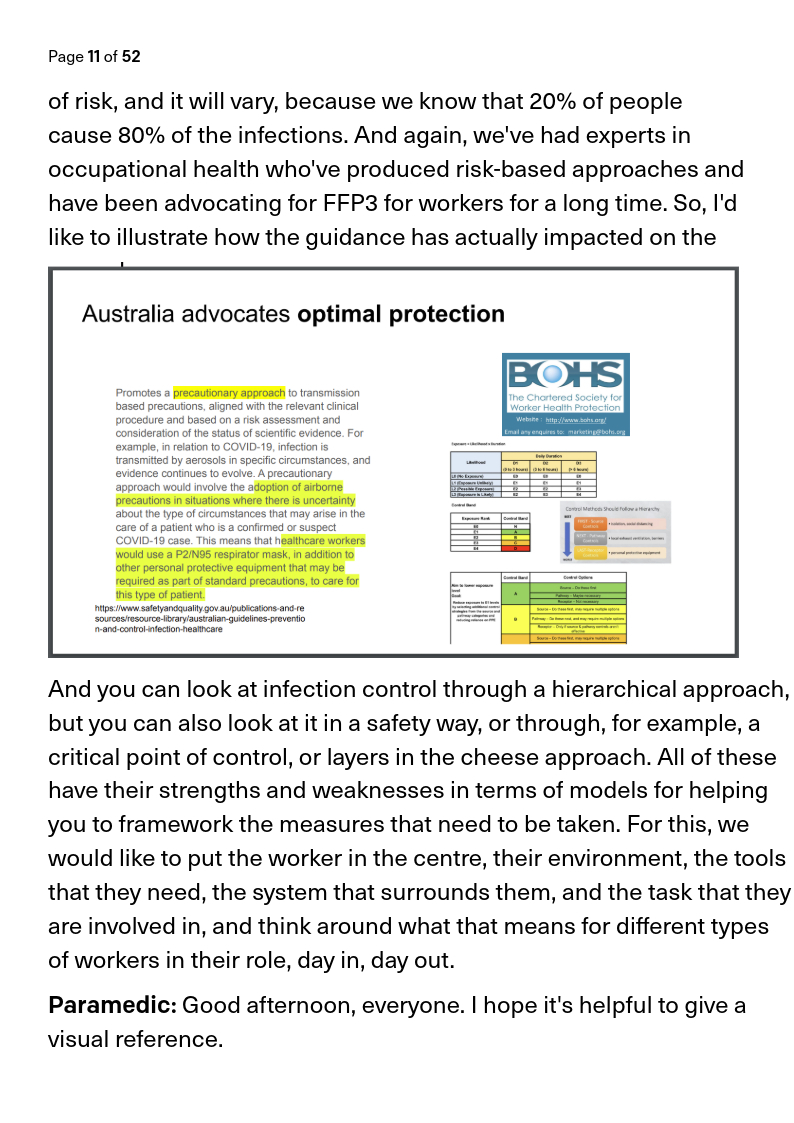

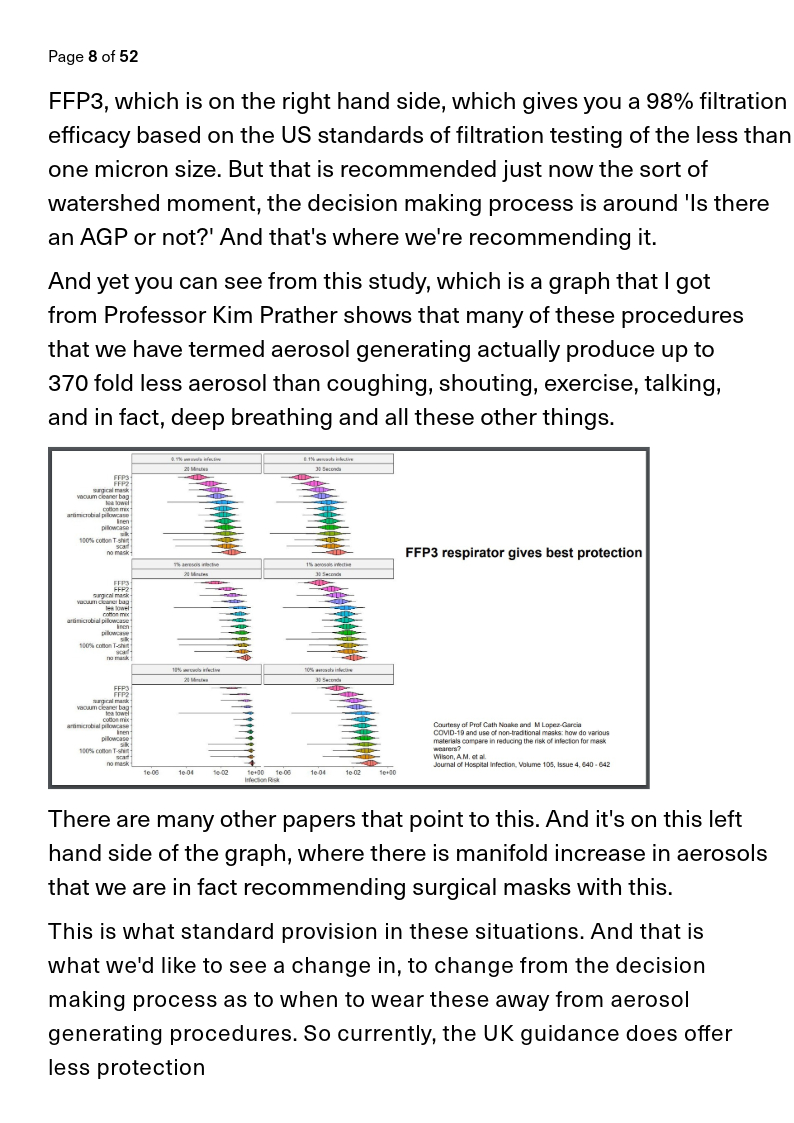
And the level of professionalism and understanding and experience is so clear:

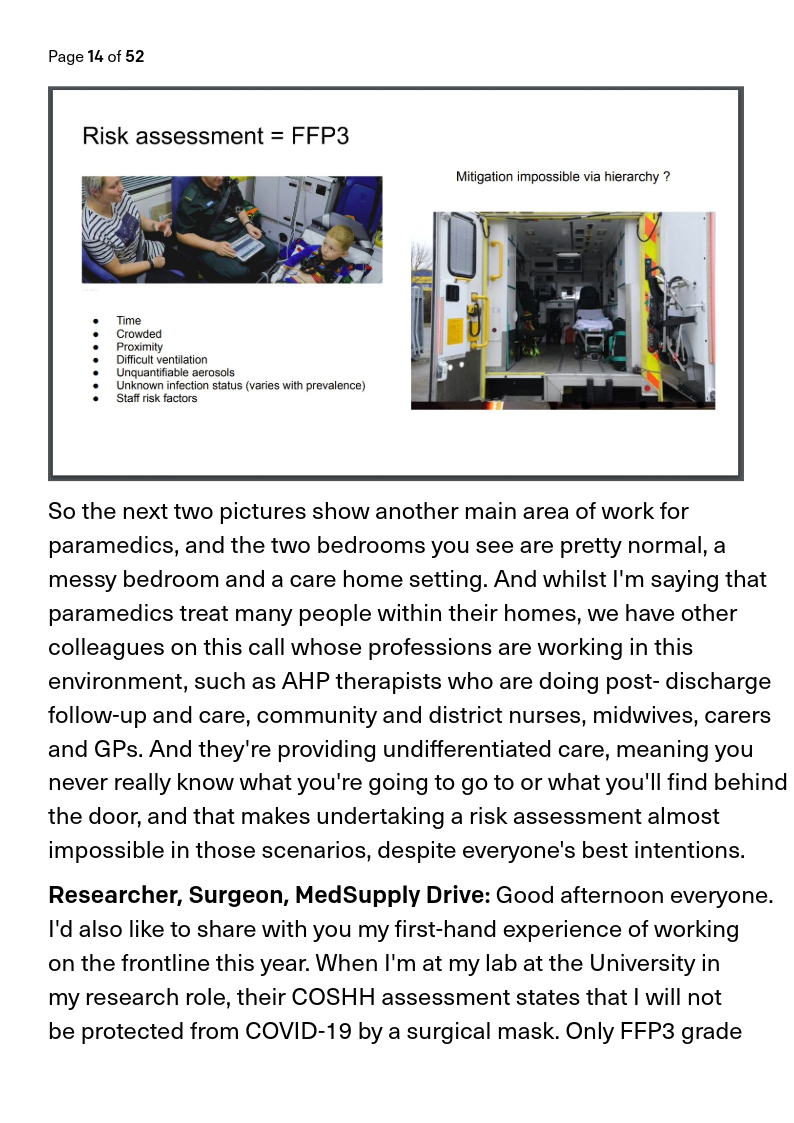

And you get discipline after discipline represented by eloquent, informed, intelligent advocates.


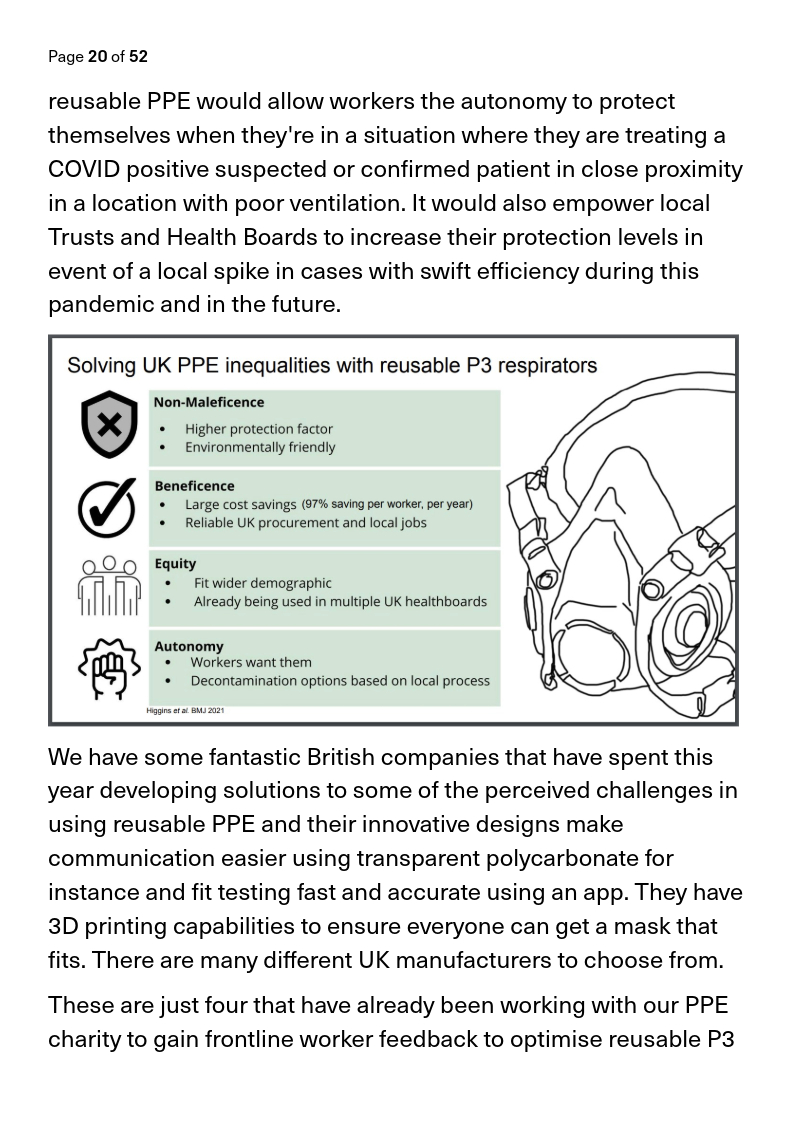
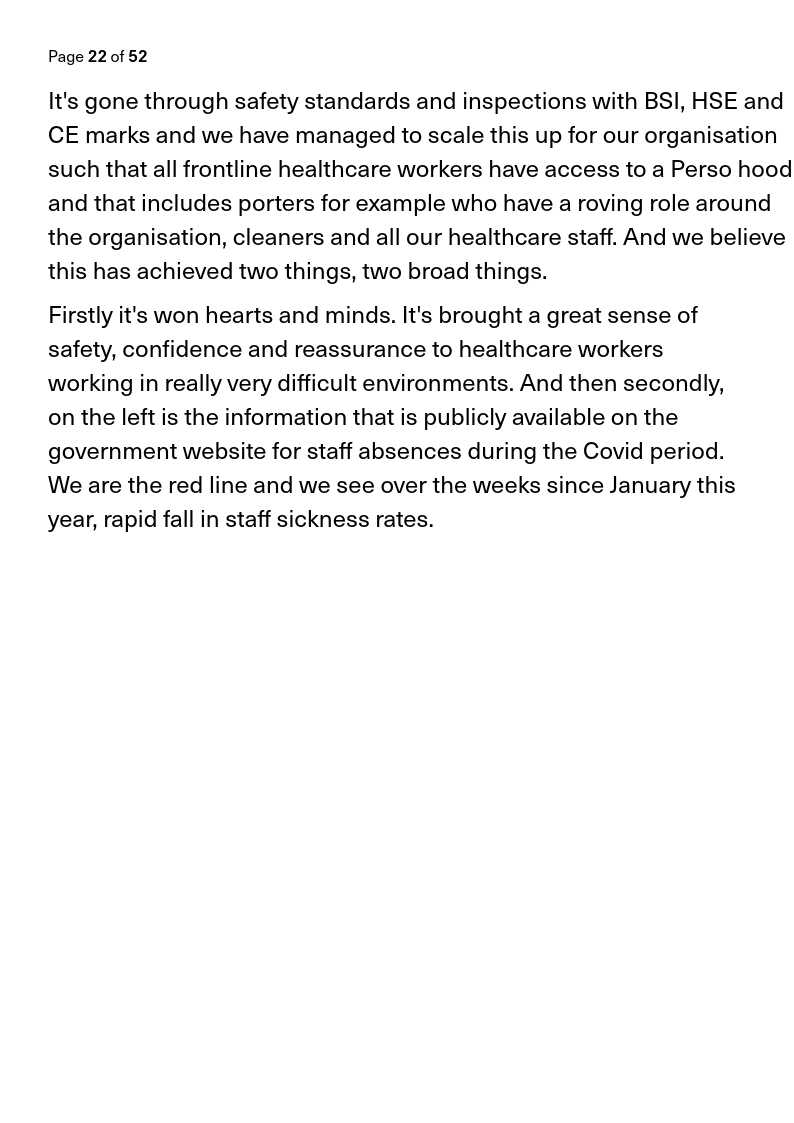
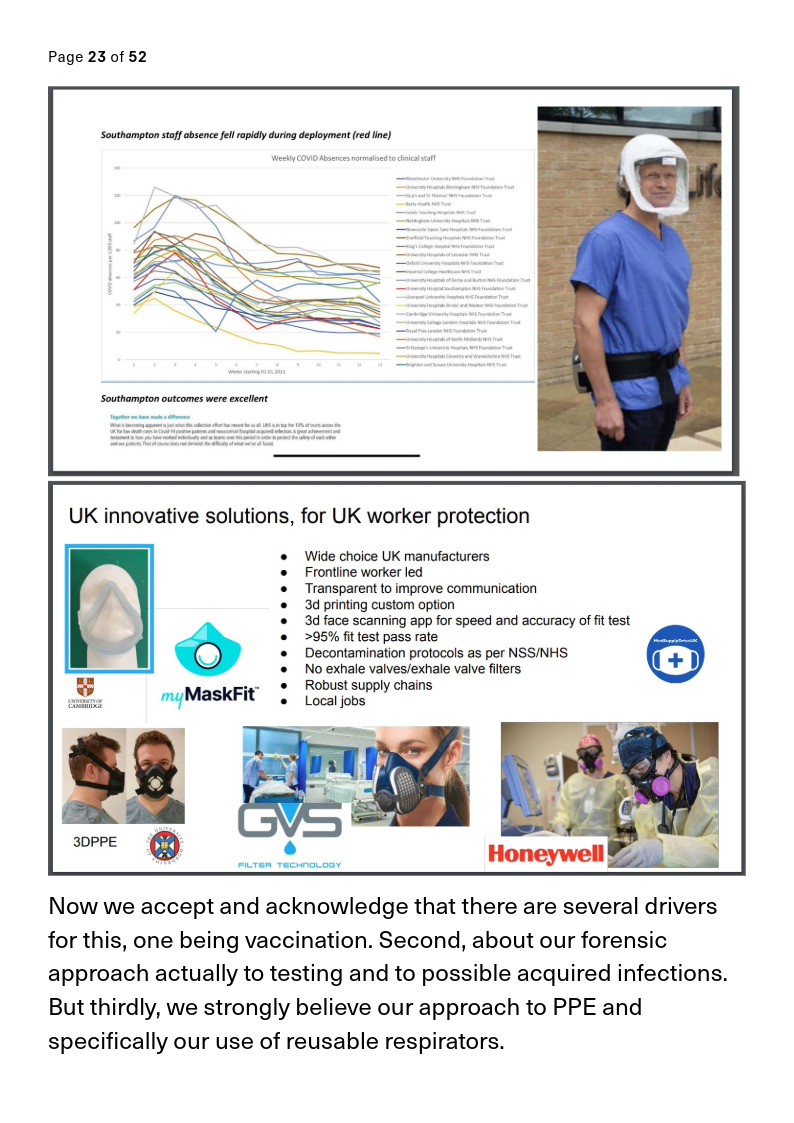
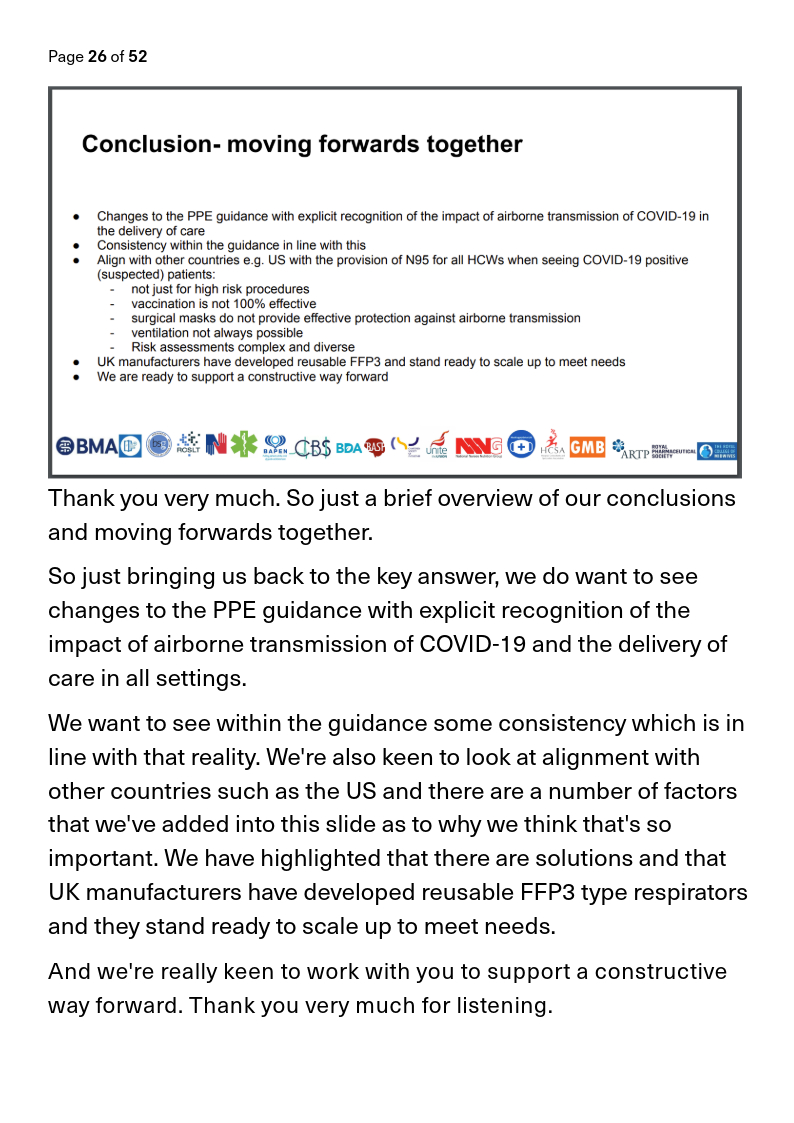
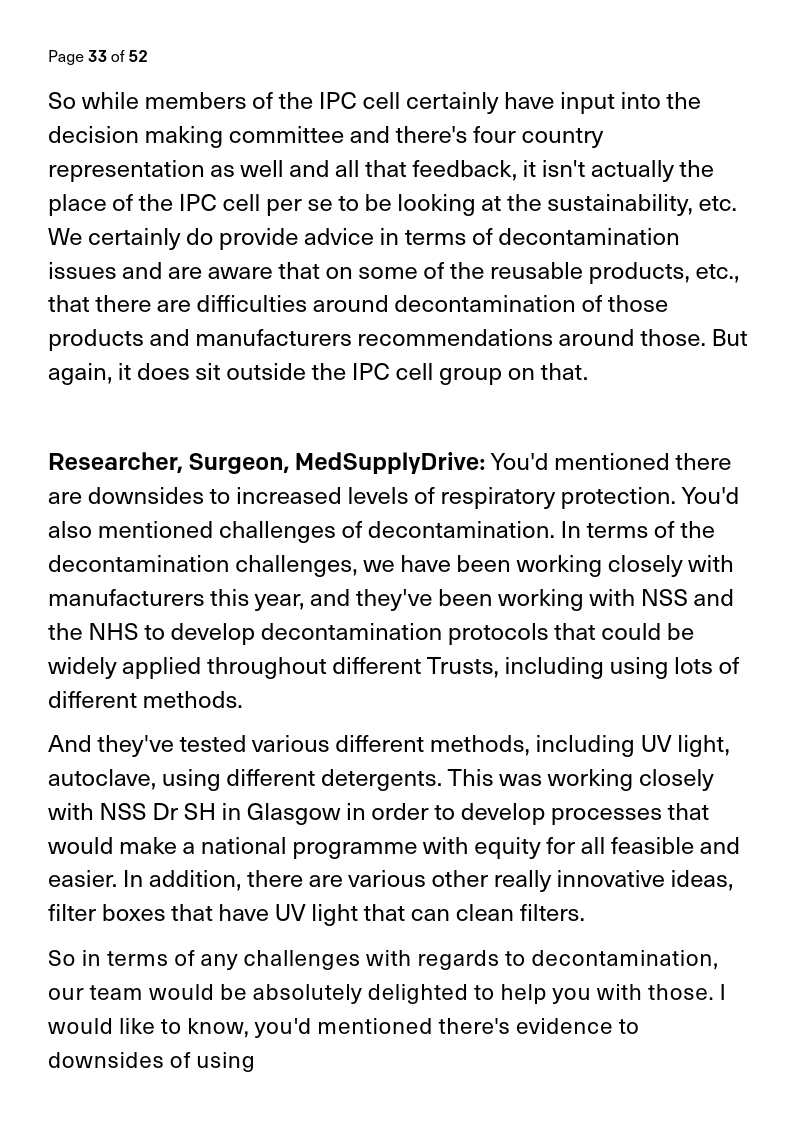
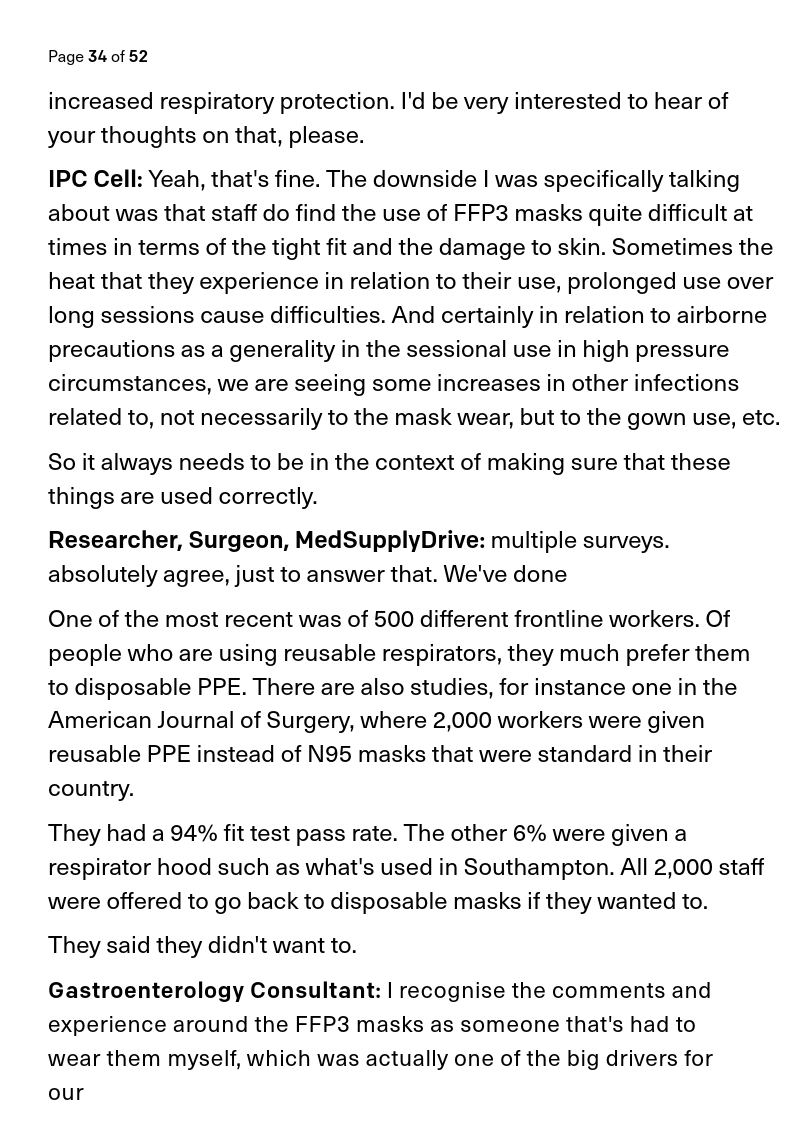
Practical suggestions.
Solutions provided.
Solutions provided.

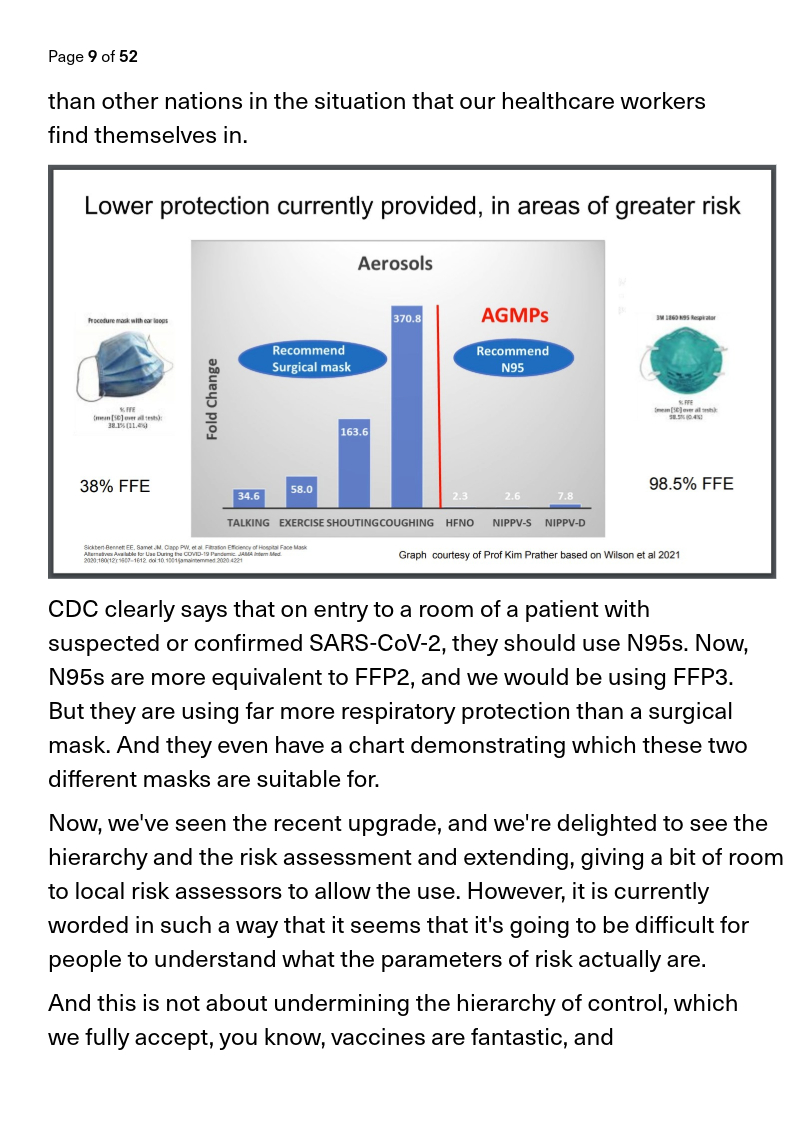
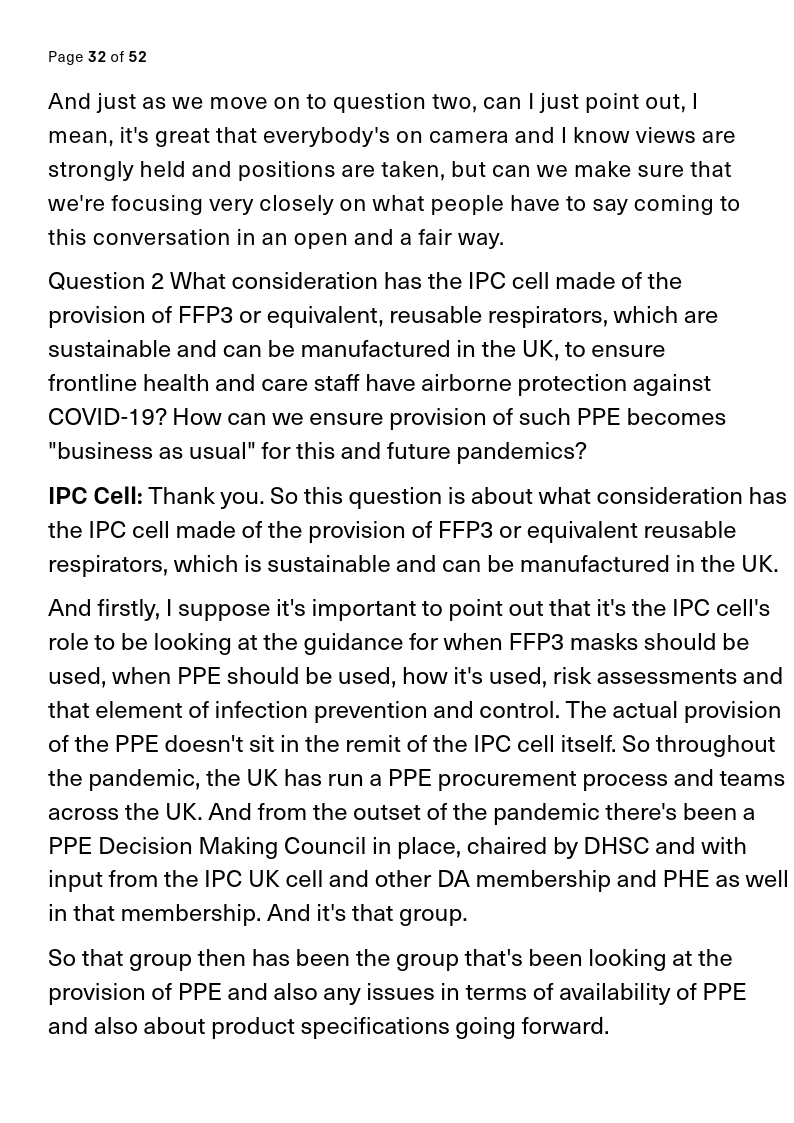
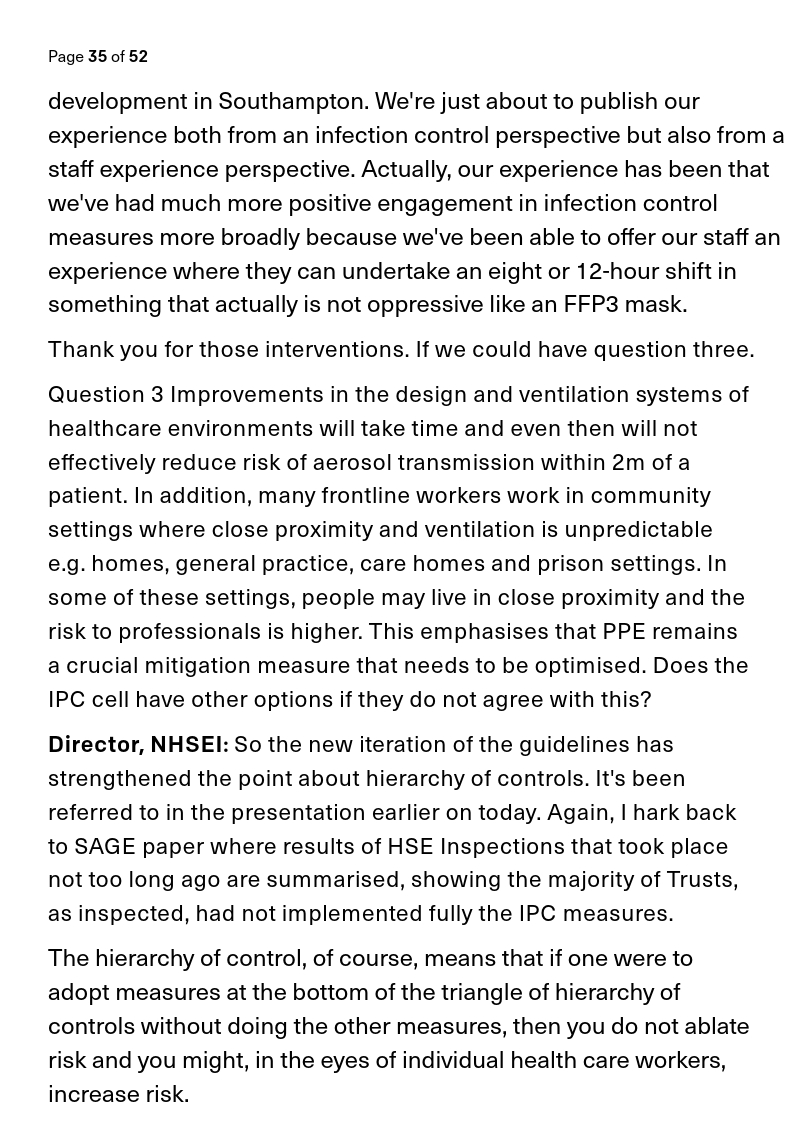
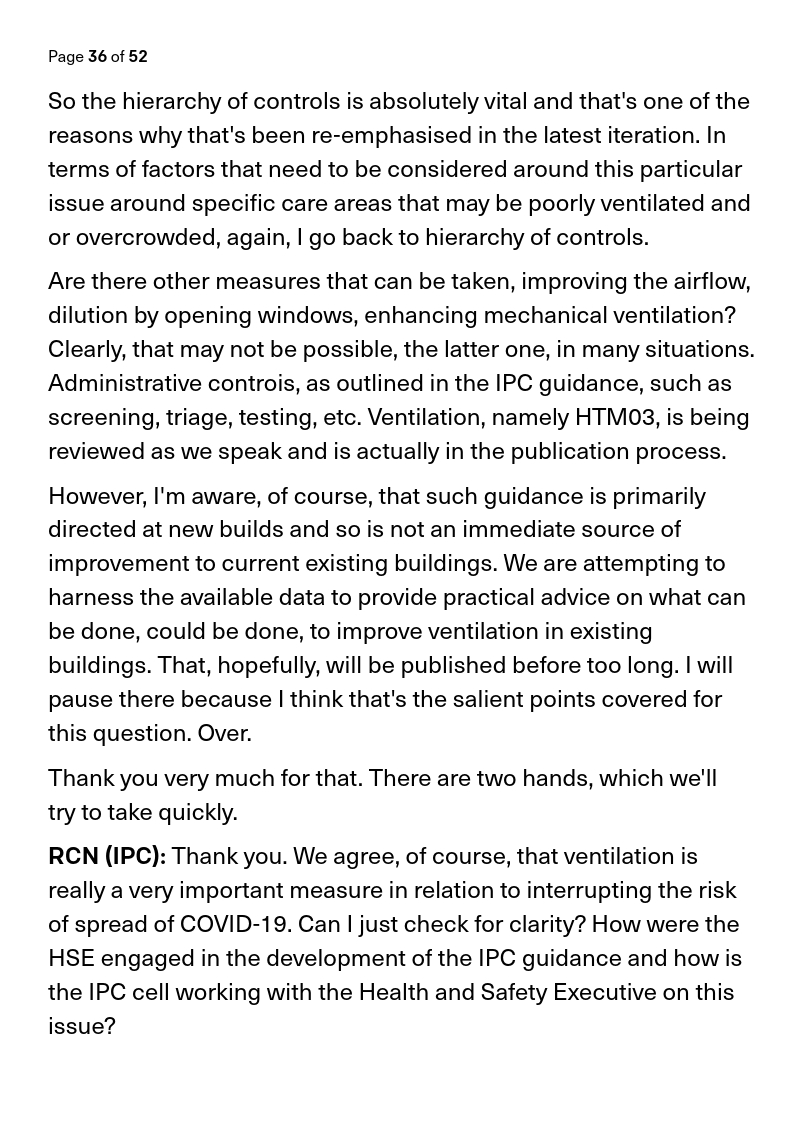
And then comes the government response...

... which just feels like a load of gaslighting, misdirection, avoidance of the question, and you can read the frustration from the people involved in the meeting...

... you ever been in a zoom meeting where you can read the disbelief, anger, and frustration just from the people on camera...
I can't fit all the alt text on the images - I'm going to share it in a single tweet at the end of the image part of the thread...
And you don't need to read the frustration from the faces on camera... because then they start to say it out loud...
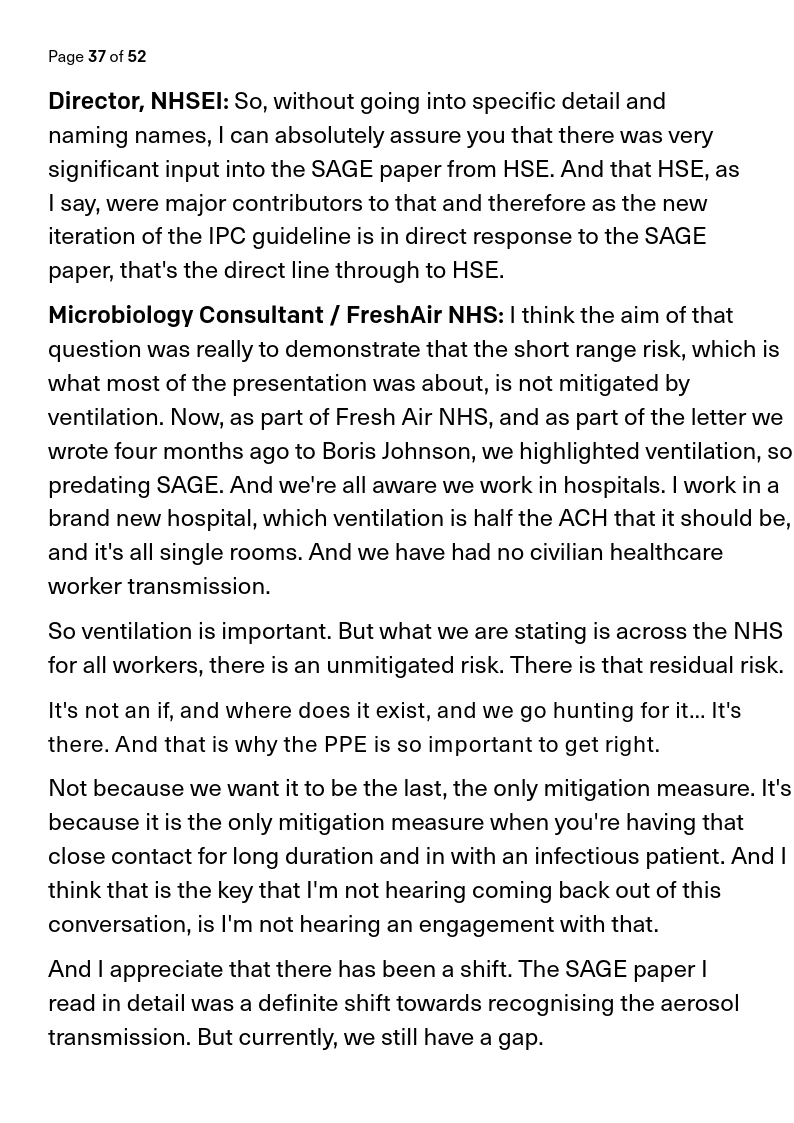



And those evasive answers come back round again.
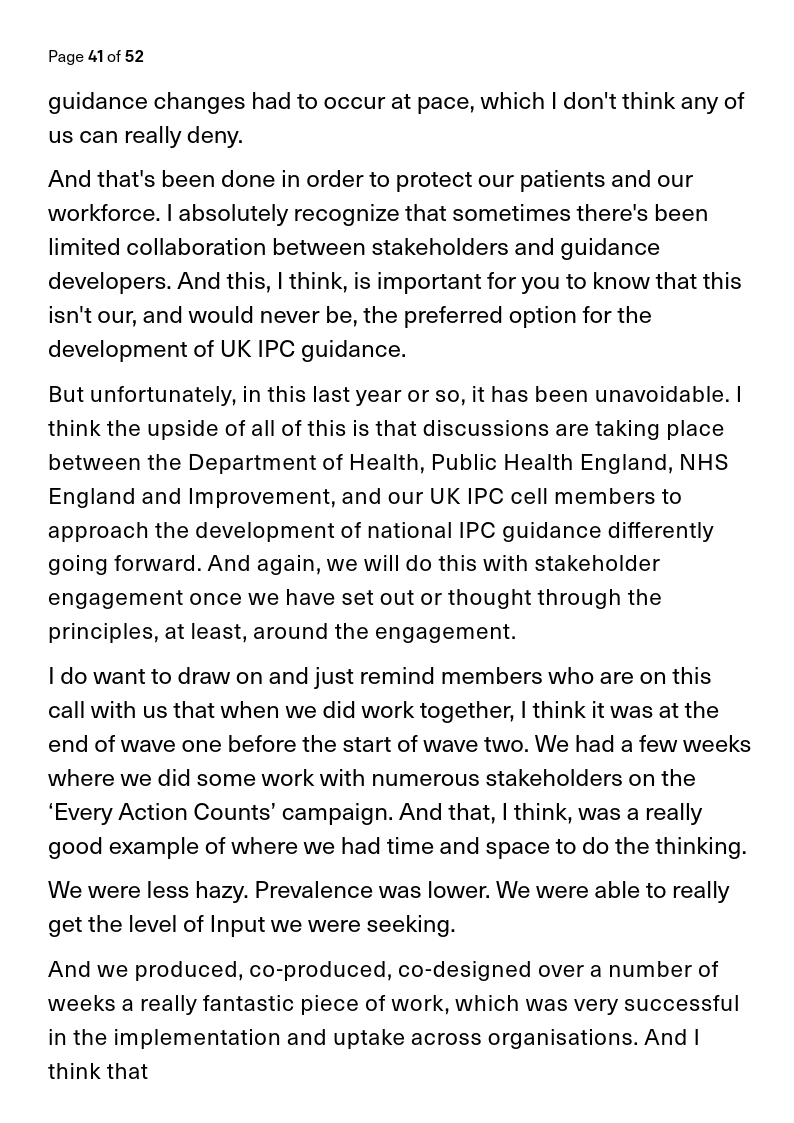


Promises to take action... but none is going to come...



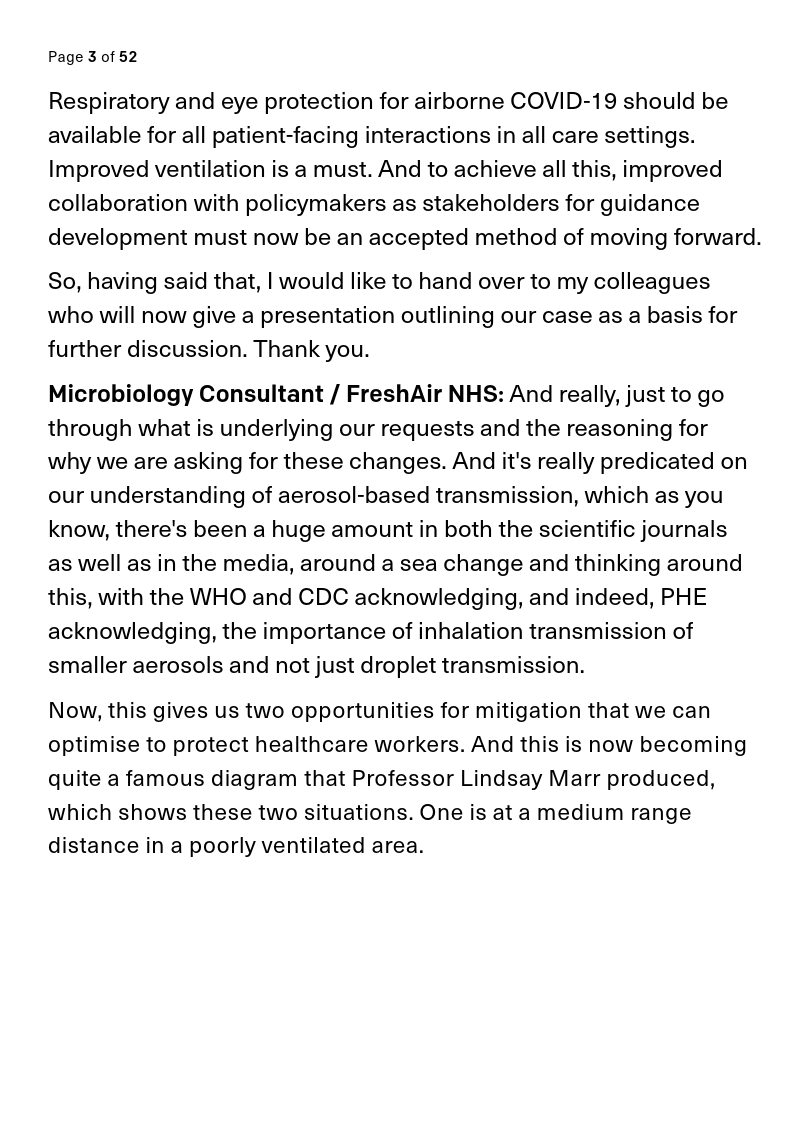
And the meeting ends in government shambles.



So it comes back round to Cat's thread.
I have no idea why the @covidinquiryuk don't have those minutes and didn't confront those IPC leads when they gave their contradictory testimony.
I have no idea why the @covidinquiryuk don't have those minutes and didn't confront those IPC leads when they gave their contradictory testimony.
https://x.com/_CatintheHat/status/1860072299933892660
I didn't get to see much of the inquiry last week, but those videos in that thread contain such an egregious collection of evasions and fabrications to cover their backs for the appalling guidance they provided.
Meeting transcript here:
https://x.com/1goodtern/status/1860781050479136855
• • •
Missing some Tweet in this thread? You can try to
force a refresh