Today the American Society of Anesthesiologists won a fight to continue defrauding Americans by overcharging them for care.
So let's talk anesthesiologists.
They are notorious for "surprise billing", where they charge an out-of-network rate at an in-network facility.
Thread.
So let's talk anesthesiologists.
They are notorious for "surprise billing", where they charge an out-of-network rate at an in-network facility.
Thread.
https://twitter.com/cremieuxrecueil/status/1864532455853547934

Anesthesiology was one of the medical specialties that was the most likely to cause a surprise bill, because patients usually don't select their anesthesiologist.
This meant lots of patients got saddled with out-of-network care, even at an in-network facility.
This meant lots of patients got saddled with out-of-network care, even at an in-network facility.

This has, to some extent, been reduced recently thanks to state-level protective legislation, and also to the federal No Surprises Act that went into effect in January of 2022.
Unfortunately, there are still exceptions aplenty, so surprise bills still exist.
Unfortunately, there are still exceptions aplenty, so surprise bills still exist.

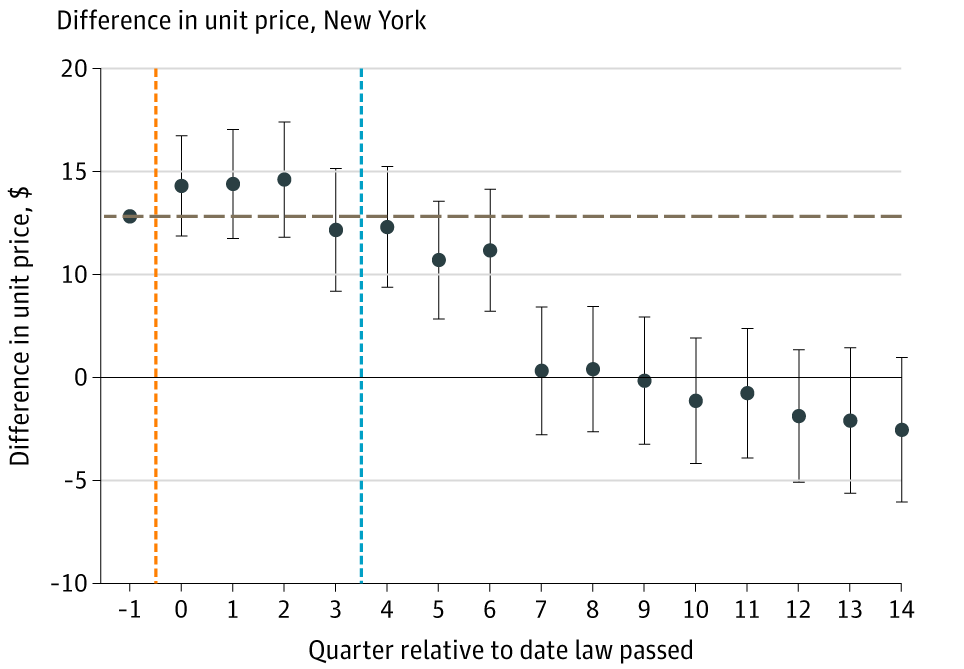
Before the Act, several states passed laws to reduce the amount of surprise billing
When New York did this, prices paid to in-network anesthesiologists were comparable to peer states' between the law passing (orange line) and being implemented (blue), then they abruptly declined
When New York did this, prices paid to in-network anesthesiologists were comparable to peer states' between the law passing (orange line) and being implemented (blue), then they abruptly declined
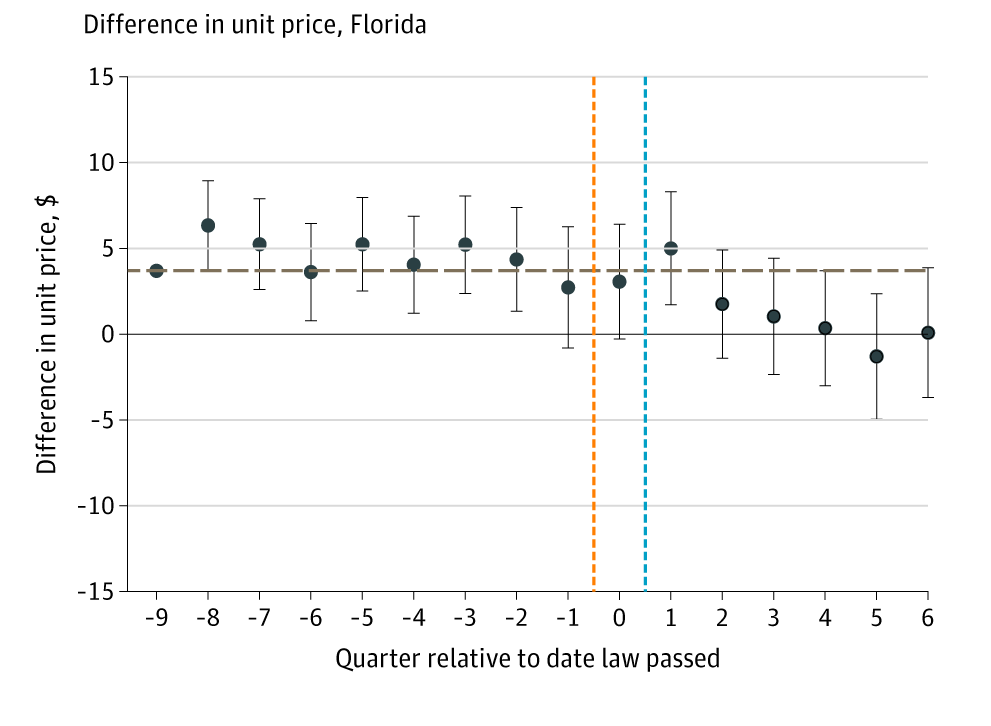
When Florida passed their own surprise ban, prices started falling shortly after the ban went into effect.
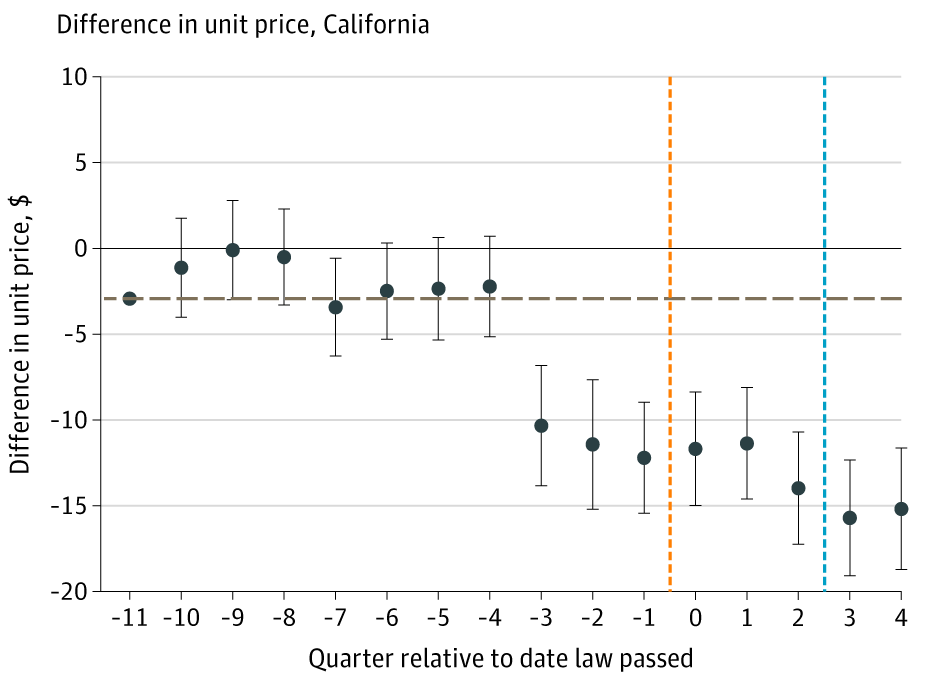
But something much more interesting happened in California.
In California, the legislature had problems getting their ban passed until it was adjusted to become more acceptable.
Because of the knowledge of this legislation appearing and returning, doctors anticipated round 2.
In California, the legislature had problems getting their ban passed until it was adjusted to become more acceptable.
Because of the knowledge of this legislation appearing and returning, doctors anticipated round 2.
In California, prices declined substantially when the bill was reintroduced to the senate, well before it was passed or implemented
It then might've fallen a bit more after implementation
What this makes clear is that anesthesiologists know what they're doing when they surprise
It then might've fallen a bit more after implementation
What this makes clear is that anesthesiologists know what they're doing when they surprise
Anesthesiologists are handsomely paid, and the experience of curbing even one aspect of their misbehavior shows us that at least some of their misbehavior is very likely to be intentional--a choice rather than a mere mistake.
But they get away with it.
But they get away with it.
If you've been online in the past two days, you probably heard about the assassination of the CEO of UnitedHealthcare and an outcry against BCBS shortly thereafter based on statements by the American Society of Anesthesiologists (ASA), supported by progressive groups and journos.
The ASA was protesting Anthem's decision to try to stop anesthesiologists billing them for work they didn't actually do by paying them the same rate that Medicare pays them for the procedures they do.
Medicare's rate is fair, but anesthesiologists hate it.
Medicare's rate is fair, but anesthesiologists hate it.
Paying on a per-procedure basis stops people from misreporting how long they work so they can order insurers (and patients) to pay them for more time.
This is fair, but anesthesiologists were understandably upset because this means their compensation goes down.
This is fair, but anesthesiologists were understandably upset because this means their compensation goes down.
Their compensation goes down even if they're in the majority of anesthesiologists who don't directly commit fraud because Medicare services more than 100 million Americans, and they have the power to dictate prices that are much lower than what private insurers are forced to pay.
This is related to why surprise bills were a thing in the first place.
Surprise bills generally reflected one of either resource unavailability or market power on the part of doctors.
The first one has to do with the AMA.
Surprise bills generally reflected one of either resource unavailability or market power on the part of doctors.
The first one has to do with the AMA.
If you need a certain type of specialist at a given moment in time, they might not be available.
If you're in a small area and your network is adequate outside of that special moment, you're out of luck.
If you're in a well-serviced area with an adequate network, it's different
If you're in a small area and your network is adequate outside of that special moment, you're out of luck.
If you're in a well-serviced area with an adequate network, it's different
If you're in a well-serviced area and you find yourself getting a surprise, it can reflect you making a mistake, or the effect of there not being enough specialists because their supply has been restricted due to legislation that the AMA and other medical associations lobbied for
If it's not those things, it usually ends up being something worse: doctors having market power, so they fail to reach an agreement with insurers who can't come to an agreement to profitably bring them in-network.
This happens all the time in rural areas: the doctors band together and won't contract with insurers unless insurers provide them terms that are extremely favorable.
If you're a doctor in a small specialty in a small area, you're golden, and not harmful enough for govt. to care.
If you're a doctor in a small specialty in a small area, you're golden, and not harmful enough for govt. to care.
Americans put up with this extremely suboptimal system in part because doctors have *amazing* PR.
They're your doctor after all! You go to them. You trust them. They're your friend. Hell, they might've even saved your life!
And they are well-spoken, generally good people.
They're your doctor after all! You go to them. You trust them. They're your friend. Hell, they might've even saved your life!
And they are well-spoken, generally good people.
But they still have bad incentives that cause them to act in ways that are materially harmful, and to misrepresent what they're doing.
That out-of-network surprise anesthesia rate? It's about five-times the Medicare rate the ASA was protesting.
That out-of-network surprise anesthesia rate? It's about five-times the Medicare rate the ASA was protesting.
But the Medicare rate is fair, or at least, doctors have never managed to show it's unfair.
They commonly argue that they have to charge private plans way more in order to subsidize the people paying the Medicare rate, but they've never shown that, even though it should be easy.
They commonly argue that they have to charge private plans way more in order to subsidize the people paying the Medicare rate, but they've never shown that, even though it should be easy.
People accurately say "most doctors are good", they make half-hearted defenses of cartel-like doctors' associations that make it hard to improve America's healthcare situation, and they believe the person denying their claim is the bad guy when that's so rarely true.
The conversation around insurance rejections, fraud, billing, and much else is horrible because of the number of professional constraints, privacy regulations, and the multitude of barriers to transparency.
Get rejected? It's almost always just plan mix and coding stringency.
Get rejected? It's almost always just plan mix and coding stringency.
If you want a better system, you have to understand that doctors aren't free of sin just because the ones you know are good guys and gals who you know and trust.
To reform healthcare in America, you have to deal with the fact that a lot of them have very bad incentives.
To reform healthcare in America, you have to deal with the fact that a lot of them have very bad incentives.
There's so much more left to say, but that's not for a site with a small character limit.
Here's the study I referenced. Make sure you click through to the other one on anesthesiologists' likely-fraudulent rounding too: jamanetwork.com/journals/jamai…
Here's the study I referenced. Make sure you click through to the other one on anesthesiologists' likely-fraudulent rounding too: jamanetwork.com/journals/jamai…
• • •
Missing some Tweet in this thread? You can try to
force a refresh