
Dec 16th update:
Increasing numbers this week as the holiday season kicks in. I believe the prior week was undersampled and this week was oversampled. ED data shows a slower rise over 2 wks (next post)
🔸286,000 new infections/day
🔸1 in every 112 people currently infected
Increasing numbers this week as the holiday season kicks in. I believe the prior week was undersampled and this week was oversampled. ED data shows a slower rise over 2 wks (next post)
🔸286,000 new infections/day
🔸1 in every 112 people currently infected

Emergency department data is currently 5 more days up to date than WW, and the trend looks quite different. Slow, steady increases. The reality may lie somewhere between them. I didn't post a WW update last week because I thought the decrease was a mirage.

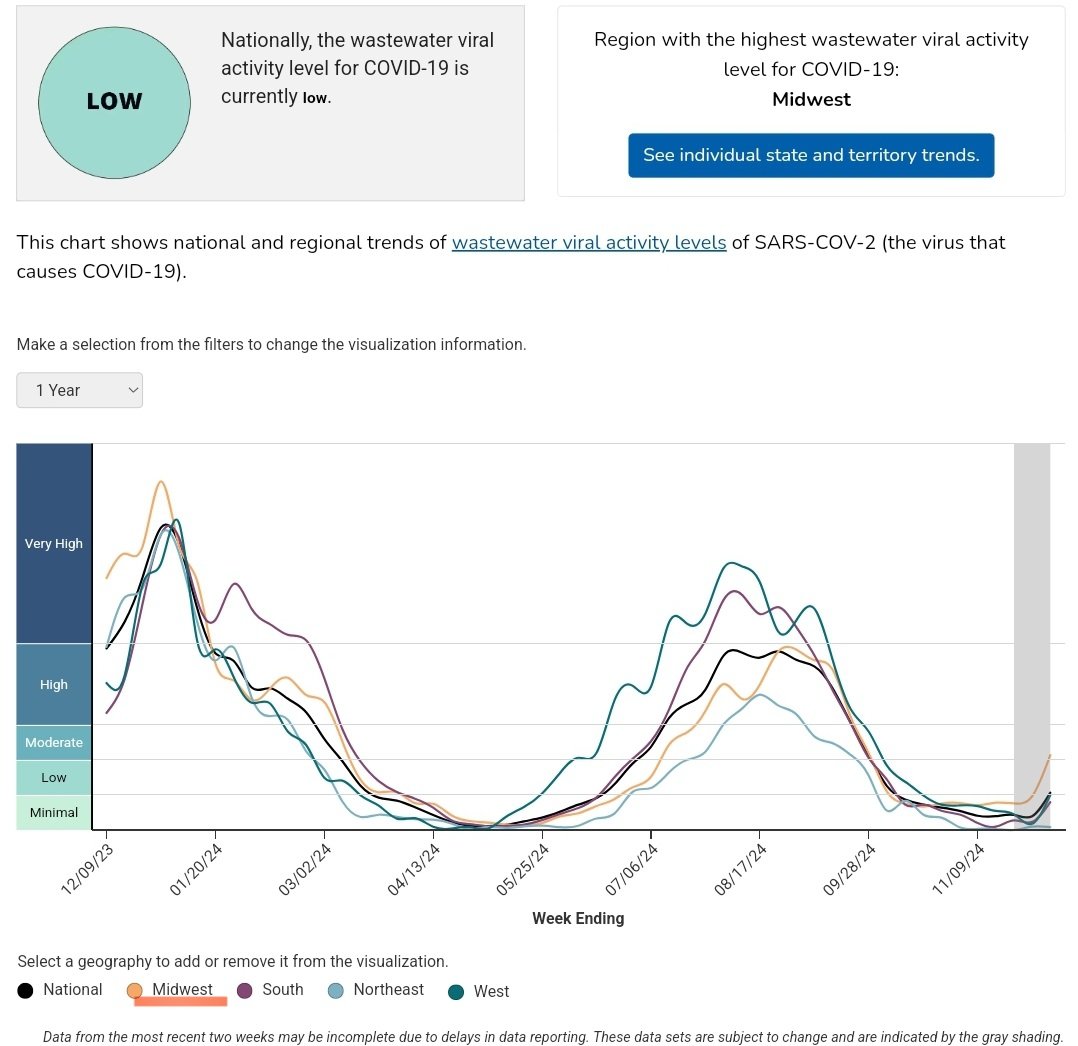
Either way, we are still over 3x lower on case levels than the prior two years at this time. But we are getting back to moderate levels of spread- just not the large surge we are used to at this time.
I have kept my calibration consistent.
I have kept my calibration consistent.
It's worth mentioning that the Midwest is at about double the levels of the other regions. AZ and NM are also elevated.
• • •
Missing some Tweet in this thread? You can try to
force a refresh













