
THE COVID INJECTIONS CAUSE AGGRESSIVE (TURBO) CANCERS EN MASSE: A MEGA-THREAD SHOWCASING THE OVERWHELMING EVIDENCE OF AN UNTHINKABLE HORROR THAT WILL TOUCH US ALL (1/57+)🧵
(Stick this thread on any post with a Community Note saying the injections don’t cause turbo cancers.)
Thread index:
Tweets 1–16: Physicians, Scientists, and Industry Experts—from the U.S., U.K., Canada, Germany, and Sweden—Describe How the COVID Injections Cause Turbo Cancers
The injections—
-Severely degrade the immune system, particularly causing T-cell suppression
-Are adulterated with DNA plasmids, which contain the notorious SV40 promoter sequence, which has not only been associated with oncogenesis, but also binding with P53 a.k.a. “the guardian of the genome”
-Are associated with far more aggressive cancers than what was normal prior to the injections’ rollout
-Are associated with increasing rates of cancers
Tweets 17–23: Anecdotal interviews with people describing aggressive cancers in themselves, their friends, or family members who’ve taken one or more COVID injections.
Tweets 24–39: Evidence in the scientific literature and regulatory documentation that supports the idea that the COVID injections degrade the immune system, are capable of causing aggressive cancers, and contain DNA and SV40 contamination.
Tweets 40–47: A—small—sample of the VAERS reports linking the COVID injections to various types of cancers.
Tweets 48–57: Users on X speak out about themselves, family, or friends who developed an aggressive, often fatal, cancer following receipt of one or more COVID injections.
NOTE: Please add your own COVID injection–related “turbo cancer” story to this thread to bolster the already overwhelming evidence that it is indeed a real phenomenon.
—-----------------------
DR. DAVID RASNICK—“I’m convinced that the true explanation of what’s behind turbo cancer is that these [COVID] injections…are devastating the immune system…[and] now we’re seeing a consequence of that devastated immune system.”
In this first tweet, we start by hearing from cancer and AIDS research titan Dr. David Rasnick, who notes in a 2024 interview with Children’s Health Defense that this phenomenon of “turbo cancers” is new, and is defined by cancers that appear and grow to Stage 3 or Stage 4—i.e. “lethal”—in a matter of months.
Rasnick, who earned a PhD in chemistry from the Georgia Institute of Technology in 1978, has more than 20 years of experience in the pharmaceutical and biotech industries, published numerous scientific papers, and invented novel laboratory techniques, notes that these turbo cancers are also affecting younger people than usual, including people in their 20s.
“When it [the turbo cancer] develops, they get late stage cancer and they’re dead really, really quickly,” Rasnick says. “That is new.”
Furthermore, Rasnick says the only other time these kinds of rapid-growing cancers have been observed was in lab animals that were made to be immune deficient “by design.”
“I’m convinced that the true explanation of what’s behind turbo cancer,” Rasnick says, “is that these [COVID] injections…these mRNA and DNA genetic injections…are devastating the immune system…[and] now we’re seeing a consequence of that devastated immune system.”
Rasnick adds, “Once your immune system is really, really depressed, now these things [cancers] can develop rapidly.” The cancer researcher adds, “We’re basically doing to human beings what we did to laboratory animals: We’re destroying their immune systems to the point where they can’t resist the cancer. And the cancers are now growing like they are in cell culture. They don’t have anything impeding their ability to proliferate.”
(Stick this thread on any post with a Community Note saying the injections don’t cause turbo cancers.)
Thread index:
Tweets 1–16: Physicians, Scientists, and Industry Experts—from the U.S., U.K., Canada, Germany, and Sweden—Describe How the COVID Injections Cause Turbo Cancers
The injections—
-Severely degrade the immune system, particularly causing T-cell suppression
-Are adulterated with DNA plasmids, which contain the notorious SV40 promoter sequence, which has not only been associated with oncogenesis, but also binding with P53 a.k.a. “the guardian of the genome”
-Are associated with far more aggressive cancers than what was normal prior to the injections’ rollout
-Are associated with increasing rates of cancers
Tweets 17–23: Anecdotal interviews with people describing aggressive cancers in themselves, their friends, or family members who’ve taken one or more COVID injections.
Tweets 24–39: Evidence in the scientific literature and regulatory documentation that supports the idea that the COVID injections degrade the immune system, are capable of causing aggressive cancers, and contain DNA and SV40 contamination.
Tweets 40–47: A—small—sample of the VAERS reports linking the COVID injections to various types of cancers.
Tweets 48–57: Users on X speak out about themselves, family, or friends who developed an aggressive, often fatal, cancer following receipt of one or more COVID injections.
NOTE: Please add your own COVID injection–related “turbo cancer” story to this thread to bolster the already overwhelming evidence that it is indeed a real phenomenon.
—-----------------------
DR. DAVID RASNICK—“I’m convinced that the true explanation of what’s behind turbo cancer is that these [COVID] injections…are devastating the immune system…[and] now we’re seeing a consequence of that devastated immune system.”
In this first tweet, we start by hearing from cancer and AIDS research titan Dr. David Rasnick, who notes in a 2024 interview with Children’s Health Defense that this phenomenon of “turbo cancers” is new, and is defined by cancers that appear and grow to Stage 3 or Stage 4—i.e. “lethal”—in a matter of months.
Rasnick, who earned a PhD in chemistry from the Georgia Institute of Technology in 1978, has more than 20 years of experience in the pharmaceutical and biotech industries, published numerous scientific papers, and invented novel laboratory techniques, notes that these turbo cancers are also affecting younger people than usual, including people in their 20s.
“When it [the turbo cancer] develops, they get late stage cancer and they’re dead really, really quickly,” Rasnick says. “That is new.”
Furthermore, Rasnick says the only other time these kinds of rapid-growing cancers have been observed was in lab animals that were made to be immune deficient “by design.”
“I’m convinced that the true explanation of what’s behind turbo cancer,” Rasnick says, “is that these [COVID] injections…these mRNA and DNA genetic injections…are devastating the immune system…[and] now we’re seeing a consequence of that devastated immune system.”
Rasnick adds, “Once your immune system is really, really depressed, now these things [cancers] can develop rapidly.” The cancer researcher adds, “We’re basically doing to human beings what we did to laboratory animals: We’re destroying their immune systems to the point where they can’t resist the cancer. And the cancers are now growing like they are in cell culture. They don’t have anything impeding their ability to proliferate.”
(2/57) DR. RYAN COLE — “[These shots]...cause immune suppression. They cause a disruption and dysregulation of your immune system that normally is what would fight cancer.”
In this clip from a 2023 interview with Greg Hunter, Dr. Ryan Cole, a board-certified pathologist and founder of Cole Diagnostics Inc. in Boise, Idaho, says that he saw early warning signs of immune system suppression following the rollout of the COVID injections and warned people that they “suppress the immune system.”
Cole notes that the injections “alter the way your immune system works.” He adds that they “[put] your T cells to sleep” in such a way that they can’t perform their “surveillance” duties “to fight cancer.”
The veteran pathologist adds that he has traveled the world, talking to oncologists, pathologists, family doctors, et al., who say that they’re “seeing cancers…in age groups…never seen before, and it happened after the rollout of the shots.”
Cole adds that insurance datasets and some countries’ disability data confirms the huge uptick in cancers. In the U.K., for example, Cole says that in 2021, there was a 6–7% rise in cancers; in 2022, there was a staggering 35% increase.
“Those are the types of data that we’re seeing that [are] really concerning,” Cole adds.
In this clip from a 2023 interview with Greg Hunter, Dr. Ryan Cole, a board-certified pathologist and founder of Cole Diagnostics Inc. in Boise, Idaho, says that he saw early warning signs of immune system suppression following the rollout of the COVID injections and warned people that they “suppress the immune system.”
Cole notes that the injections “alter the way your immune system works.” He adds that they “[put] your T cells to sleep” in such a way that they can’t perform their “surveillance” duties “to fight cancer.”
The veteran pathologist adds that he has traveled the world, talking to oncologists, pathologists, family doctors, et al., who say that they’re “seeing cancers…in age groups…never seen before, and it happened after the rollout of the shots.”
Cole adds that insurance datasets and some countries’ disability data confirms the huge uptick in cancers. In the U.K., for example, Cole says that in 2021, there was a 6–7% rise in cancers; in 2022, there was a staggering 35% increase.
“Those are the types of data that we’re seeing that [are] really concerning,” Cole adds.
(3/57) DR. ROGER HODKINSON— “The immune system has been taken off its watch…[there could be] a tsunami of…cancer and other conditions that have been brought on…by this vaccination program.”
In this clip from a 2022 interview with the RAIR Foundation, Dr. Roger Hodkinson, a medical specialist in pathology, a graduate of Cambridge University, and a Fellow at the Royal College of Physicians and Surgeons of Canada (FRCPC), echoes Dr. Ryan Cole’s concerns regarding the COVID injections’ deleterious effects on the immune system.
“One of the primary functions of the immune system is to surveil the entire body, looking for little, tiny cancers that can be knocked off before they get to a size when they produce a lump or a syndrome that kills you…[And] with the [COVID] vaccination, having a profound impact on the vitality of our immune system, the deep concern is that some of these cancers that are being reported, or maybe all of them, are due to immune escape,” Hodkinson says. The pathologist adds, “the immune system has been…taken off its watch…and the cancer has been allowed to proliferate in a way that it would not normally have done.”
Hodkinson goes on to note: “[This] could result in a tsunami of…cancer and other conditions that have been brought on…by this vaccination program.” He adds, “When…something of this magnitude…is not studied, that is cause for enormous concern. Because that is not the way medicine works.”
In this clip from a 2022 interview with the RAIR Foundation, Dr. Roger Hodkinson, a medical specialist in pathology, a graduate of Cambridge University, and a Fellow at the Royal College of Physicians and Surgeons of Canada (FRCPC), echoes Dr. Ryan Cole’s concerns regarding the COVID injections’ deleterious effects on the immune system.
“One of the primary functions of the immune system is to surveil the entire body, looking for little, tiny cancers that can be knocked off before they get to a size when they produce a lump or a syndrome that kills you…[And] with the [COVID] vaccination, having a profound impact on the vitality of our immune system, the deep concern is that some of these cancers that are being reported, or maybe all of them, are due to immune escape,” Hodkinson says. The pathologist adds, “the immune system has been…taken off its watch…and the cancer has been allowed to proliferate in a way that it would not normally have done.”
Hodkinson goes on to note: “[This] could result in a tsunami of…cancer and other conditions that have been brought on…by this vaccination program.” He adds, “When…something of this magnitude…is not studied, that is cause for enormous concern. Because that is not the way medicine works.”
(4/57) SCIENTIST KEVIN MCKERNAN—”The EMA…has documents that have leaked showing a one to 815-fold variance in the amount of DNA contamination that are in these vaccines.”
In this clip from a presentation given to the International COVID Summit in 2024, Kevin McKernan, Founder and Chief Scientific Officer of Medicinal Genomics, as well as former R&D lead of the Human Genome Project, describes how there is “DNA contamination” in the mRNA COVID injections from both Pfizer and Moderna. McKernan notes that there is DNA plasmid contamination of between one and 815-fold from injection lot to injection lot (i.e. batch to batch) and that the contamination has been found by scientists in multiple states in the U.S. and in Germany. (The one to 815-fold figure means that the amount of DNA plasmids present in a given injection is up to 815 times the allowable amount set by regulatory agencies.)
McKernan notes that regulators have, in turn, been forced to respond to the contamination and that the FDA in the U.S., the European Medicines Agency (EMA), and Health Canada have all confirmed that there is indeed DNA plasmids in the COVID mRNA injections. McKernan notes that the regulators have also confirmed that this DNA contamination includes the so-called “SV40 promoter,” which is a DNA sequence derived from the Simian Virus 40 that enhances gene expression. I.e. the SV40 promoter helps to import the contaminating DNA plasmids into the nucleus of the cell.
Furthermore, McKernan notes that the inclusion of the SV40 in the contaminating DNA plasmids was originally withheld from the regulators by Pfizer.
Note that, as outlined in the documentation in tweet 39 in this mega-thread, an FDA guidance document published back in 2010 states the following:
“Residual DNA might be a risk to your final product because of oncogenic [i.e. cancer causing] and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration.”
In this clip from a presentation given to the International COVID Summit in 2024, Kevin McKernan, Founder and Chief Scientific Officer of Medicinal Genomics, as well as former R&D lead of the Human Genome Project, describes how there is “DNA contamination” in the mRNA COVID injections from both Pfizer and Moderna. McKernan notes that there is DNA plasmid contamination of between one and 815-fold from injection lot to injection lot (i.e. batch to batch) and that the contamination has been found by scientists in multiple states in the U.S. and in Germany. (The one to 815-fold figure means that the amount of DNA plasmids present in a given injection is up to 815 times the allowable amount set by regulatory agencies.)
McKernan notes that regulators have, in turn, been forced to respond to the contamination and that the FDA in the U.S., the European Medicines Agency (EMA), and Health Canada have all confirmed that there is indeed DNA plasmids in the COVID mRNA injections. McKernan notes that the regulators have also confirmed that this DNA contamination includes the so-called “SV40 promoter,” which is a DNA sequence derived from the Simian Virus 40 that enhances gene expression. I.e. the SV40 promoter helps to import the contaminating DNA plasmids into the nucleus of the cell.
Furthermore, McKernan notes that the inclusion of the SV40 in the contaminating DNA plasmids was originally withheld from the regulators by Pfizer.
Note that, as outlined in the documentation in tweet 39 in this mega-thread, an FDA guidance document published back in 2010 states the following:
“Residual DNA might be a risk to your final product because of oncogenic [i.e. cancer causing] and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration.”
(5/57) PROF. ANGUS DALGLEISH—“[The] synthetic DNA contamination…in…vials of the Pfizer and Moderna COVID-19 vaccines…presents risks of genomic instability, which can manifest as cancers…”
Professor Angus Dalgleish, a professor of oncology at St. George’s, University of London, describes in a presentation given to the Special Council at Port Hedland Town in Western Australia in 2024 how the DNA contamination found in the COVID mRNA injections by McKernan, et al. “can manifest as cancers, immune disorders, and hereditary diseases.”
“Synthetic DNA contamination as detected in Australian vials of the Pfizer and Moderna COVID-19 vaccines by David Speicher presents risks of genomic instability, which can manifest as cancers, immune disorders, and hereditary diseases,” Dalgleish says. “The vaccines contain lipid nanoparticles, which encapsulate synthetic DNA fragments. These nanoparticles deliver this DNA into various organs throughout the body, where the DNA has the potential to integrate into our own genetic material. As such these vaccines are not ‘vaccines,’ they are, in fact, gene therapy based. This genomic integration, as the scientific literature makes clear, can lead to cancer development, immune system disruption, and more. The sheer levels of contamination detected…in some cases are extraordinary, and far beyond what should be allowed in any medicinal product.”
Dalgleish goes on to note: “While this may sound like a remote possibility…we are already seeing evidence of these effects in real patients. In my work as an oncologist in the U.K., I started to see a disturbing trend as early as February 2022. Patients who had been cancer free for many years were suddenly relapsing with aggressive, explosive cancers shortly after receiving booster doses of the COVID-19 vaccine. I personally counted six cases in as many weeks in patients who developed a rapid progression, having been completely stable, with zero disease, having been on an immunotherapy I had given them 5, 8, 10, 15, 18 years ago.”
Dalgleish adds: “All these patients only had one thing in common, and that was they had all been forced to have a [COVID-injection] booster by their GPs on the grounds they were at risk. One of the most unsettling aspects of the nature of these cancers is that they are not slow progressing…they are aggressive, often presenting at advanced stages, affecting multiple organs by the time they are diagnosed. Colorectal cancer has specifically shown explosive growth—something we’ve never seen before. These cancers are emerging faster and more virulent than we would expect in patients who otherwise have been stable.”
Dalgleish also notes a rise in blood cancers, such as leukemias and lymphomas, which have “appeared shortly after vaccinations.”
“I have had many colleagues and patients express concerns about the timing of these cancers following what I believe are totally unnecessary boosters, which is not an isolated issue,” the oncologist goes on to say. “My own research has shown that the boosters suppress the T cell response and switch[es] the antibody response to tolerizing. That means this is the perfect example where you have switched off the policing of foreign invaders, viruses, etc. and cancer, allowing it to grow uncontrolled.”
Professor Angus Dalgleish, a professor of oncology at St. George’s, University of London, describes in a presentation given to the Special Council at Port Hedland Town in Western Australia in 2024 how the DNA contamination found in the COVID mRNA injections by McKernan, et al. “can manifest as cancers, immune disorders, and hereditary diseases.”
“Synthetic DNA contamination as detected in Australian vials of the Pfizer and Moderna COVID-19 vaccines by David Speicher presents risks of genomic instability, which can manifest as cancers, immune disorders, and hereditary diseases,” Dalgleish says. “The vaccines contain lipid nanoparticles, which encapsulate synthetic DNA fragments. These nanoparticles deliver this DNA into various organs throughout the body, where the DNA has the potential to integrate into our own genetic material. As such these vaccines are not ‘vaccines,’ they are, in fact, gene therapy based. This genomic integration, as the scientific literature makes clear, can lead to cancer development, immune system disruption, and more. The sheer levels of contamination detected…in some cases are extraordinary, and far beyond what should be allowed in any medicinal product.”
Dalgleish goes on to note: “While this may sound like a remote possibility…we are already seeing evidence of these effects in real patients. In my work as an oncologist in the U.K., I started to see a disturbing trend as early as February 2022. Patients who had been cancer free for many years were suddenly relapsing with aggressive, explosive cancers shortly after receiving booster doses of the COVID-19 vaccine. I personally counted six cases in as many weeks in patients who developed a rapid progression, having been completely stable, with zero disease, having been on an immunotherapy I had given them 5, 8, 10, 15, 18 years ago.”
Dalgleish adds: “All these patients only had one thing in common, and that was they had all been forced to have a [COVID-injection] booster by their GPs on the grounds they were at risk. One of the most unsettling aspects of the nature of these cancers is that they are not slow progressing…they are aggressive, often presenting at advanced stages, affecting multiple organs by the time they are diagnosed. Colorectal cancer has specifically shown explosive growth—something we’ve never seen before. These cancers are emerging faster and more virulent than we would expect in patients who otherwise have been stable.”
Dalgleish also notes a rise in blood cancers, such as leukemias and lymphomas, which have “appeared shortly after vaccinations.”
“I have had many colleagues and patients express concerns about the timing of these cancers following what I believe are totally unnecessary boosters, which is not an isolated issue,” the oncologist goes on to say. “My own research has shown that the boosters suppress the T cell response and switch[es] the antibody response to tolerizing. That means this is the perfect example where you have switched off the policing of foreign invaders, viruses, etc. and cancer, allowing it to grow uncontrolled.”
(6/57) DR. UTE KRÜGER—“Ultimately, I saw a correlation that the tumors appeared on average three [3] months after these so-called ‘vaccinations.’”
In this clip from an interview with klaTVEnglish from 2024, Dr. Ute Krüger, a pathologist and breast cancer researcher in Sweden, describes her experience witnessing the exact same phenomenon Dr. Angus Dalgleish did in the previous tweet: explosive, aggressive cancers that appeared in cancer patients who were previously stable prior to receiving one or more COVID injections.
Krüger describes how, following the rollout of the COVID injections, she began to see the largest tumors she had ever seen in her career. “And the tumors simply grew more aggressively, and there were more frequent occurrences, [meaning] relapses,” Krüger adds.
The pathologist and breast cancer researcher notes: “Patients may have been tumor free for 20 years, and then a few months after these injections against corona, the tumor suddenly came back. And with such aggressiveness that the patients often died as a result.”
In this clip from an interview with klaTVEnglish from 2024, Dr. Ute Krüger, a pathologist and breast cancer researcher in Sweden, describes her experience witnessing the exact same phenomenon Dr. Angus Dalgleish did in the previous tweet: explosive, aggressive cancers that appeared in cancer patients who were previously stable prior to receiving one or more COVID injections.
Krüger describes how, following the rollout of the COVID injections, she began to see the largest tumors she had ever seen in her career. “And the tumors simply grew more aggressively, and there were more frequent occurrences, [meaning] relapses,” Krüger adds.
The pathologist and breast cancer researcher notes: “Patients may have been tumor free for 20 years, and then a few months after these injections against corona, the tumor suddenly came back. And with such aggressiveness that the patients often died as a result.”
(7/57) DR. JOHN CAMPBELL, describing the work of DR. DAVID SPEICHER—“The Moderna [injection] can contain up to 10 [trillion] copies of DNA fragments per dose.”
In this clip from a video posted in October 2024, Dr. John Campbell, a semi-retired nurse lecturer, describes work performed by molecular virologist Dr. David Speicher, which found that in some of the COVID injection vials, there are 10 TRILLION copies of the DNA plasmids. Campbell notes that 3 to 10 copies is “enough to cause incorporation of SV40 DNA contamination into the nuclear genome of the cell, thereby causing a mutation, which has been identified in cell cultures in chromosomes 9 and 12, including an oncogene that can potentially cause cancer.”
In this clip from a video posted in October 2024, Dr. John Campbell, a semi-retired nurse lecturer, describes work performed by molecular virologist Dr. David Speicher, which found that in some of the COVID injection vials, there are 10 TRILLION copies of the DNA plasmids. Campbell notes that 3 to 10 copies is “enough to cause incorporation of SV40 DNA contamination into the nuclear genome of the cell, thereby causing a mutation, which has been identified in cell cultures in chromosomes 9 and 12, including an oncogene that can potentially cause cancer.”
(8/57) DR. ANGUS DALGLEISH (PT. 2)—“The Pfizer [injections] are all full of SV40 [and] SV40 was what, in my day, we put into mice to make them grow tumors…”
Here is Professor Angus Dalgleish once again, this time in a clip taken from a discussion with Charles Kovess et al. from December of 2024.
Dalgleish notes the following:
"It's obvious talking to everybody and all the presentations I've been to....[that] they're [the COVID injections] all completely contaminated. They're just not fit for purpose," Dalgleish says. "The Pfizer [injections] are all full of SV40 [and] SV40 was what, in my day, we put into mice to make them grow tumors so we could pour chemotherapy into them to see if it worked for the tumors. And we are putting this into humans for a disease that hasn't killed anybody for at least two years. It is beyond belief, and that's really what I cannot understand."
Here is Professor Angus Dalgleish once again, this time in a clip taken from a discussion with Charles Kovess et al. from December of 2024.
Dalgleish notes the following:
"It's obvious talking to everybody and all the presentations I've been to....[that] they're [the COVID injections] all completely contaminated. They're just not fit for purpose," Dalgleish says. "The Pfizer [injections] are all full of SV40 [and] SV40 was what, in my day, we put into mice to make them grow tumors so we could pour chemotherapy into them to see if it worked for the tumors. And we are putting this into humans for a disease that hasn't killed anybody for at least two years. It is beyond belief, and that's really what I cannot understand."
(9/57) DR. SUCHARIT BHAKDI—“The integration of any foreign gene into your chromosome can cause cancer immediately.”
Sucharit Bhakdi, a retired Professor Emeritus of Medical Microbiology and Immunology and former Chair of the Institute of Medical Microbiology and Hygiene at Johannes Gutenberg University of Mainz, describes in this clip taken from a conversation with Children’s Health Defense from May 2023 how the integration of foreign genes into a person’s genome can lead to cancer.
Bhakdi notes that mRNA injections cause this type of damage because “the [DNA] plasmids, these foreign genes derived from bacteria, stolen from bacteria, enter the human cells, and…every cell that is genetically altered is doomed.”
Sucharit Bhakdi, a retired Professor Emeritus of Medical Microbiology and Immunology and former Chair of the Institute of Medical Microbiology and Hygiene at Johannes Gutenberg University of Mainz, describes in this clip taken from a conversation with Children’s Health Defense from May 2023 how the integration of foreign genes into a person’s genome can lead to cancer.
Bhakdi notes that mRNA injections cause this type of damage because “the [DNA] plasmids, these foreign genes derived from bacteria, stolen from bacteria, enter the human cells, and…every cell that is genetically altered is doomed.”
(10/57) KEVIN MCKERNAN (Pt. 2)—“This SV40 component…it interacts with P53 [which] is [the] guardian of the genome that’s supposed to keep our genome intact…[and] it’s the most cited gene in cancer.”
In this clip from an interview Kevin McKernan did with Bret Weinstein, he notes that the SV40—which has been firmly established as being present in the DNA plasmid contamination in the COVID injections—interacts with P53, a gene that is commonly referred to as “the guardian of the genome.”
“This SV40 component…it interacts with P53 [which] is [the] guardian of the genome that’s supposed to keep our genome intact,” McKernan says. “And now we have billions of these molecules being injected that we know interact with that.”
Furthermore, McKernan adds that P53 is “the most cited gene in cancer,” and “if you mess with P53, you’re inviting cancer, particularly if you shut it down.”
The scientist also notes that simply having fragmented DNA inside the cytosol of cells—that is, the liquid portion of the cytoplasm within a cell, where many biochemical reactions occur—is enough to cause cancer; meaning the DNA doesn’t even need to be imported into the nucleus of the cell.
“It [the plasmids] doesn’t have to get into the nucleus to cause cancer. Just cytosolic presence of DNA like this can trigger this cGAS STING pathway,” McKernan notes. (The cGAS-STING pathway is an innate immune signaling route that detects cytosolic DNA to trigger an immune response, including inflammation and an antiviral defense.)
In this clip from an interview Kevin McKernan did with Bret Weinstein, he notes that the SV40—which has been firmly established as being present in the DNA plasmid contamination in the COVID injections—interacts with P53, a gene that is commonly referred to as “the guardian of the genome.”
“This SV40 component…it interacts with P53 [which] is [the] guardian of the genome that’s supposed to keep our genome intact,” McKernan says. “And now we have billions of these molecules being injected that we know interact with that.”
Furthermore, McKernan adds that P53 is “the most cited gene in cancer,” and “if you mess with P53, you’re inviting cancer, particularly if you shut it down.”
The scientist also notes that simply having fragmented DNA inside the cytosol of cells—that is, the liquid portion of the cytoplasm within a cell, where many biochemical reactions occur—is enough to cause cancer; meaning the DNA doesn’t even need to be imported into the nucleus of the cell.
“It [the plasmids] doesn’t have to get into the nucleus to cause cancer. Just cytosolic presence of DNA like this can trigger this cGAS STING pathway,” McKernan notes. (The cGAS-STING pathway is an innate immune signaling route that detects cytosolic DNA to trigger an immune response, including inflammation and an antiviral defense.)
(11/57) DR. JANCI LINDSAY— “LNPs have been found to cause cancer cells that are already present to more readily spread by inducing endothelial leakiness.”
In this clip from a presentation given for the World Council for Health, posted in 2023, toxicologist and molecular biologist Dr. Janci Linsday describes the nine (or more) ways the mRNA COVID injections can cause cancer. In her presentation, Lindsay notes that:
–the injections use lipid nanoparticles (LNPs), which have been found to cause cancer cells that are already present to spread more readily
–the LNPs may be oncogenic by themselves
–the SV40 is a “super promoter” that is “great at driving gene expression,” and should it sit above an oncogene, you could have “an amplification of a cancer gene.”
–the spike protein can interact with, and suppress, P53, the aforementioned “guardian of the genome.”
–the injections can produce “frame shifted” proteins, which are aberrant and can themselves cause cancer
–the mRNA in the injections itself can reverse transcribe into the genome, in turn causing insertional mutagenesis and cancer
–the injections cause immunosuppression of T cells, which, in turn, can damage the immune system and lead to cancer (as previously mentioned in the thread)
In this clip from a presentation given for the World Council for Health, posted in 2023, toxicologist and molecular biologist Dr. Janci Linsday describes the nine (or more) ways the mRNA COVID injections can cause cancer. In her presentation, Lindsay notes that:
–the injections use lipid nanoparticles (LNPs), which have been found to cause cancer cells that are already present to spread more readily
–the LNPs may be oncogenic by themselves
–the SV40 is a “super promoter” that is “great at driving gene expression,” and should it sit above an oncogene, you could have “an amplification of a cancer gene.”
–the spike protein can interact with, and suppress, P53, the aforementioned “guardian of the genome.”
–the injections can produce “frame shifted” proteins, which are aberrant and can themselves cause cancer
–the mRNA in the injections itself can reverse transcribe into the genome, in turn causing insertional mutagenesis and cancer
–the injections cause immunosuppression of T cells, which, in turn, can damage the immune system and lead to cancer (as previously mentioned in the thread)
(12/57) KEVIN MCKERNAN (Pt. 3)—“We have sequencing from a colon [tumor] biopsy from a patient who was four [4] times vaccinated…we can find [Pfizer-injection DNA] plasmids in there at a hundred copies per cell.”
In this clip from a 2024 Mind & Matter podcast, we hear again from scientist Kevin McKernan, who describes finding the DNA plasmids from Pfizer’s mRNA COVID injection in a colon tumor from a—now deceased—individual who received four injections.
”We have sequencing from a colon biopsy from a patient who was four [4] times vaccinated. A year after vaccination, they had a colon cancer. They biopsied it that day, and then 30 days later, they died, and then they biopsied after, and we have sequencing on both the pre-mortem and post-mortem samples," McKernan says. The scientist and entrepreneur, often cited as the first person to find DNA contamination in the mRNA COVID injections, adds, "we can find plasmids in there a hundred copies per cell. They're not exactly the same as Pfizer's, which is a real head-scratcher, but they're in there."
McKernan goes on to say: “The copy number alone suggests that these things aren't fully fragmented. Right? These plasmids really shouldn't be replicating to a hundred copies per cell." McKernan adds, "They shouldn't be in there at that level because if you just do the math on how much is in the vaccine, when you do an injection of this, this person has four vaccines...1.2 ml of Pfizer...went into about 87,000 mls [of] body volume. So you should have a massive dilution into your body. Yet when we're sequencing this and doing qPCR off the tumor, the CTs coming back off the tumor are almost as high as they are straight out of the vial."
In this clip from a 2024 Mind & Matter podcast, we hear again from scientist Kevin McKernan, who describes finding the DNA plasmids from Pfizer’s mRNA COVID injection in a colon tumor from a—now deceased—individual who received four injections.
”We have sequencing from a colon biopsy from a patient who was four [4] times vaccinated. A year after vaccination, they had a colon cancer. They biopsied it that day, and then 30 days later, they died, and then they biopsied after, and we have sequencing on both the pre-mortem and post-mortem samples," McKernan says. The scientist and entrepreneur, often cited as the first person to find DNA contamination in the mRNA COVID injections, adds, "we can find plasmids in there a hundred copies per cell. They're not exactly the same as Pfizer's, which is a real head-scratcher, but they're in there."
McKernan goes on to say: “The copy number alone suggests that these things aren't fully fragmented. Right? These plasmids really shouldn't be replicating to a hundred copies per cell." McKernan adds, "They shouldn't be in there at that level because if you just do the math on how much is in the vaccine, when you do an injection of this, this person has four vaccines...1.2 ml of Pfizer...went into about 87,000 mls [of] body volume. So you should have a massive dilution into your body. Yet when we're sequencing this and doing qPCR off the tumor, the CTs coming back off the tumor are almost as high as they are straight out of the vial."
(13/57) RETIRED PHARMA R&D EXECUTIVE SASHA LATYPOVA— “The FDA was fully aware that these things would cause cancer because they’ve written numerous guidance documents [saying so]; that’s how they regulate industry.”
In this clip from an interview with Dr. Drew from 2024, retired pharma R&D executive Sasha Latypova describes how the "FDA was fully aware that these things [the COVID injections] would cause cancer, because they've written numerous guidance documents [saying so]; that's how they regulate industry.” Latypova notes that in “2015, 2013, even more recently than that, they wrote extensive guidance documents explaining to manufacturers who wanted to develop mRNA products that they need to study...cancer..."
"They had this knowledge and they told manufacturers you have to study these risks and you have to exclude them and they were also not allowed to even study it in healthy volunteers because it was considered unethical," Latypova adds. "It was considered too dangerous. So then we come to 2020 [and] all of the sudden all of this is solved—this is a joke. To me, that's where I became extremely suspicious..."
One such FDA guidance document referenced by Latypova is linked in tweet 39 of this mega-thread.
In this clip from an interview with Dr. Drew from 2024, retired pharma R&D executive Sasha Latypova describes how the "FDA was fully aware that these things [the COVID injections] would cause cancer, because they've written numerous guidance documents [saying so]; that's how they regulate industry.” Latypova notes that in “2015, 2013, even more recently than that, they wrote extensive guidance documents explaining to manufacturers who wanted to develop mRNA products that they need to study...cancer..."
"They had this knowledge and they told manufacturers you have to study these risks and you have to exclude them and they were also not allowed to even study it in healthy volunteers because it was considered unethical," Latypova adds. "It was considered too dangerous. So then we come to 2020 [and] all of the sudden all of this is solved—this is a joke. To me, that's where I became extremely suspicious..."
One such FDA guidance document referenced by Latypova is linked in tweet 39 of this mega-thread.
(14/57) DR. JAMES ROYLE— “In addition to the increase in all-cause excess deaths in highly vaccinated countries since the gene based–injectable rollout, there has been observed an alarming and significant increase in cancers.”
In this 2024 presentation for the Stone Summit, U.K.-based surgeon Dr. James Royle describes seeing the same kinds of phenomena regarding turbo cancers as described by Professor Angus Dalgleish, Dr. Ryan Cole, Dr. Ute Krüger, et al. He also notes that the excuses for these cancers that have been used to deflect away from the COVID injections as the cause don’t make any logical sense.
“In addition to the increase in all-cause excess deaths in highly vaccinated countries since the
gene-based injectable rollout, there has been observed an alarming and significant increase in cancers,” Royle says. “These cancers have been termed colloquially ‘turbo cancers.’ Obviously, this is not a scientific term, but reflects the different aggressive biological nature that seems to be being observed by the public as well as clinicians…There was [also] a clear, dramatic increase [in cancer rates] that occurred in 2021 shortly after the rollout.”
Royle goes on to note the following: “A robust study recently published from Japan now [retracted] by the journal after significant pressure showed cancer-related excess mortality in vaccinated populations. Cancer is being observed within all ages. It is my assertion shared by many experts oncologists and clinical colleagues around the world that the cancers we are seeing are extremely aggressive and are of a different biology. One study showed this dramatic increase, particularly in younger ages through 2021, [and in] 2022, [a] 7.9% increase.” The surgeon adds: “I've noticed aggressive widespread recurrences in previously successfully treated bowel cancer cases that I'd considered cured. Many metastases in these cases are unusual or atypical. Middle aged and elderly people are presenting with out-of-the-blue aggressive stage IV colorectal cancer who are incurable and die within weeks or months. In many of these cases, the entire liver appears to be filled with large, round tumor masses.”
The prominent surgeon notes that “many of [his] multidisciplinary team colleagues, fellow surgeons, oncologists, pathologists, radiologists and specialist nurses have all acknowledged… [a] sudden change in patterns and [a] dramatic increase in these aggressive incurable advanced cancers…observed in these past two years. However, none of them can offer an explanation.”
“This post-2021 increase cannot be explained by a sudden population-wide change in environmental toxins,” Royle notes. “Ultra-processed foods are not new. We already had an obesity epidemic prior to COVID-19,” the surgeon adds. “In any case, there is no valid argument that the increase is due to stopping [cancer] screening given we are seeing a particular increase in cancers in much younger people, 20 to 45 years of age. Screening services for colorectal cancer and breast and others typically start at 60 years [of age].”
In this 2024 presentation for the Stone Summit, U.K.-based surgeon Dr. James Royle describes seeing the same kinds of phenomena regarding turbo cancers as described by Professor Angus Dalgleish, Dr. Ryan Cole, Dr. Ute Krüger, et al. He also notes that the excuses for these cancers that have been used to deflect away from the COVID injections as the cause don’t make any logical sense.
“In addition to the increase in all-cause excess deaths in highly vaccinated countries since the
gene-based injectable rollout, there has been observed an alarming and significant increase in cancers,” Royle says. “These cancers have been termed colloquially ‘turbo cancers.’ Obviously, this is not a scientific term, but reflects the different aggressive biological nature that seems to be being observed by the public as well as clinicians…There was [also] a clear, dramatic increase [in cancer rates] that occurred in 2021 shortly after the rollout.”
Royle goes on to note the following: “A robust study recently published from Japan now [retracted] by the journal after significant pressure showed cancer-related excess mortality in vaccinated populations. Cancer is being observed within all ages. It is my assertion shared by many experts oncologists and clinical colleagues around the world that the cancers we are seeing are extremely aggressive and are of a different biology. One study showed this dramatic increase, particularly in younger ages through 2021, [and in] 2022, [a] 7.9% increase.” The surgeon adds: “I've noticed aggressive widespread recurrences in previously successfully treated bowel cancer cases that I'd considered cured. Many metastases in these cases are unusual or atypical. Middle aged and elderly people are presenting with out-of-the-blue aggressive stage IV colorectal cancer who are incurable and die within weeks or months. In many of these cases, the entire liver appears to be filled with large, round tumor masses.”
The prominent surgeon notes that “many of [his] multidisciplinary team colleagues, fellow surgeons, oncologists, pathologists, radiologists and specialist nurses have all acknowledged… [a] sudden change in patterns and [a] dramatic increase in these aggressive incurable advanced cancers…observed in these past two years. However, none of them can offer an explanation.”
“This post-2021 increase cannot be explained by a sudden population-wide change in environmental toxins,” Royle notes. “Ultra-processed foods are not new. We already had an obesity epidemic prior to COVID-19,” the surgeon adds. “In any case, there is no valid argument that the increase is due to stopping [cancer] screening given we are seeing a particular increase in cancers in much younger people, 20 to 45 years of age. Screening services for colorectal cancer and breast and others typically start at 60 years [of age].”
(15/57) DR. WILLIAM MAKIS— “Once the vaccines roll out in 2021, you see a statistically significant rise in cancer, and it rises every single year since then…there’s some kind of damage that…can manifest years after you’ve had your last COVID vaccines.”
In this clip from a discussion with pediatrician Dr. Paul Thomas, oncologist, radiologist, and cancer researcher Dr. William Makis describes some of the work that’s been done by The Ethical Skeptic on cancer trends following the rollout of the COVID injections. Makis notes that there was a “statistically significant rise in cancer” in the U.S. following the rollout of the COVID injections. Furthermore, he says that the injections cause “some kind of damage that…can manifest years after you’ve had your last COVID vaccines.”
"I love the work of Ethical Skeptic, and this is his work," Makis says of the graph he presents for Thomas. "This is a data analyst on X...and he looks at CDC data, and he finds these trends that are really fascinating."
"These are deaths from malignant neoplasms in...a younger cohort, ages 0 to 54," Makis says. "And you see that really, in 2020, you don't see much in terms of a [rise in] cancer. There seems to be a slight blip above trend line, but it's sort of still hovering around a long-term trend line. And then once the vaccines roll out in 2021, then you see a statistically significant rise in cancer, and it rises every single year since then."
Ethical Skeptic "calls it a 12-sigma event, which is...I'm not even gonna try to describe what that means, how astronomically unlikely this is to be a sort of a random thing or a coincidence," Makis says. "This is a very real trend. I'm seeing it in thousands and thousands of young people," the cancer researcher adds. "And what's shocking and what's particularly concerning about this graph—and I really want people to pay attention to this—is that people stopped taking booster shots. People have, by and large, stopped taking booster shots. But the trend continues. And it's a very steady upward trend. There's no sign of it leveling off or stopping, or reversing. And this has me really, really concerned for the long term."
Makis goes on to say:
"Initially, I started seeing these patterns...Someone would take a COVID vaccine and then they would be diagnosed with a stage 4 cancer out of the blue four months later, six months later. And I thought, 'Okay. Well, maybe there's a pattern here. Maybe there's a sort of a certain time that's required for cancer to develop.' And through my research, I found, for example, that there is a shift in the type of antibodies that we produce. It's called the IgG4 shift. And IgG4 antibodies start being produced once you've been exposed to multiple shots, once you've had at least two COVID vaccines. And these are called tolerance antibodies. This is where your...immune system starts tolerating the antigen, which is the spike protein; but it also starts tolerating cancer and cancer cells. And that takes a few months. That whole shift takes several months to happen.
"But then I start[ed] seeing cases where the young person hasn't taken a shot in the last two years, then they're just suddenly diagnosed with an aggressive stage 4 cancer that behaves the way these mRNA vaccine–induced turbo cancers are behaving, and they [the patients] have a very, very poor prognosis. They don't respond to chemotherapy or radiation therapy or even immunotherapy, and then they die approximately six to 12 months after diagnosis. So there is a long-term effect, and that is the one thing that really has me concerned...that there is something that happens to people who've had the vaccines that is permanent. There's some kind of damage that appears to be permanent, and it can manifest years after you've had your last COVID vaccines. And this is really, really, concerning for me."
In this clip from a discussion with pediatrician Dr. Paul Thomas, oncologist, radiologist, and cancer researcher Dr. William Makis describes some of the work that’s been done by The Ethical Skeptic on cancer trends following the rollout of the COVID injections. Makis notes that there was a “statistically significant rise in cancer” in the U.S. following the rollout of the COVID injections. Furthermore, he says that the injections cause “some kind of damage that…can manifest years after you’ve had your last COVID vaccines.”
"I love the work of Ethical Skeptic, and this is his work," Makis says of the graph he presents for Thomas. "This is a data analyst on X...and he looks at CDC data, and he finds these trends that are really fascinating."
"These are deaths from malignant neoplasms in...a younger cohort, ages 0 to 54," Makis says. "And you see that really, in 2020, you don't see much in terms of a [rise in] cancer. There seems to be a slight blip above trend line, but it's sort of still hovering around a long-term trend line. And then once the vaccines roll out in 2021, then you see a statistically significant rise in cancer, and it rises every single year since then."
Ethical Skeptic "calls it a 12-sigma event, which is...I'm not even gonna try to describe what that means, how astronomically unlikely this is to be a sort of a random thing or a coincidence," Makis says. "This is a very real trend. I'm seeing it in thousands and thousands of young people," the cancer researcher adds. "And what's shocking and what's particularly concerning about this graph—and I really want people to pay attention to this—is that people stopped taking booster shots. People have, by and large, stopped taking booster shots. But the trend continues. And it's a very steady upward trend. There's no sign of it leveling off or stopping, or reversing. And this has me really, really concerned for the long term."
Makis goes on to say:
"Initially, I started seeing these patterns...Someone would take a COVID vaccine and then they would be diagnosed with a stage 4 cancer out of the blue four months later, six months later. And I thought, 'Okay. Well, maybe there's a pattern here. Maybe there's a sort of a certain time that's required for cancer to develop.' And through my research, I found, for example, that there is a shift in the type of antibodies that we produce. It's called the IgG4 shift. And IgG4 antibodies start being produced once you've been exposed to multiple shots, once you've had at least two COVID vaccines. And these are called tolerance antibodies. This is where your...immune system starts tolerating the antigen, which is the spike protein; but it also starts tolerating cancer and cancer cells. And that takes a few months. That whole shift takes several months to happen.
"But then I start[ed] seeing cases where the young person hasn't taken a shot in the last two years, then they're just suddenly diagnosed with an aggressive stage 4 cancer that behaves the way these mRNA vaccine–induced turbo cancers are behaving, and they [the patients] have a very, very poor prognosis. They don't respond to chemotherapy or radiation therapy or even immunotherapy, and then they die approximately six to 12 months after diagnosis. So there is a long-term effect, and that is the one thing that really has me concerned...that there is something that happens to people who've had the vaccines that is permanent. There's some kind of damage that appears to be permanent, and it can manifest years after you've had your last COVID vaccines. And this is really, really, concerning for me."
(16/57) DR. CHARLES HOFFE—“In my practice now…approximately two-thirds of all cancer diagnoses—since the vax rollout—are stage 4.”
Topping off the first section of this turbo cancer mega-thread, which features expert testimonials from around the Western world, we have a clip of family physician Dr. Charles Hoffe speaking on turbo cancers during a 2022 Children’s Health Defense virtual roundtable. Hoffe, who has more than 30 years of experience as a family physician, notes that “as a family doctor, over the years, a small percentage of the new cancer diagnoses would unfortunately be stage 4 at first diagnosis. But in [his] practice now…approximately two-thirds of all cancer diagnoses since the vax rollout are stage 4.”
Hoffe notes, “pathologists around the world have noticed this—that, unfortunately, now people who had previous cancers, which were in remission, are flaring up since their shots because of the damage to their immune system by the COVID shots. [And with] new cancers being diagnosed, the tumors are bigger than ever. They seem to grow very aggressively, spread very aggressively, and be very resistant to treatment. So this has been nicknamed turbo cancer.”
The veteran family physician goes on to describe one such case of turbo cancer he’s seen in a man who was mandated to get a COVID injection in order to keep his job. Hoffe shows how the man, a 61-year-old machine operator, developed a grapefruit-sized tumor in his lungs within months of getting his COVID injection. He also developed other tumors, including ones that grew along the vertebrae of his spine. Hoffe notes that the prognosis at the time was that the man would almost certainly die due to the aggressive cancers.
Topping off the first section of this turbo cancer mega-thread, which features expert testimonials from around the Western world, we have a clip of family physician Dr. Charles Hoffe speaking on turbo cancers during a 2022 Children’s Health Defense virtual roundtable. Hoffe, who has more than 30 years of experience as a family physician, notes that “as a family doctor, over the years, a small percentage of the new cancer diagnoses would unfortunately be stage 4 at first diagnosis. But in [his] practice now…approximately two-thirds of all cancer diagnoses since the vax rollout are stage 4.”
Hoffe notes, “pathologists around the world have noticed this—that, unfortunately, now people who had previous cancers, which were in remission, are flaring up since their shots because of the damage to their immune system by the COVID shots. [And with] new cancers being diagnosed, the tumors are bigger than ever. They seem to grow very aggressively, spread very aggressively, and be very resistant to treatment. So this has been nicknamed turbo cancer.”
The veteran family physician goes on to describe one such case of turbo cancer he’s seen in a man who was mandated to get a COVID injection in order to keep his job. Hoffe shows how the man, a 61-year-old machine operator, developed a grapefruit-sized tumor in his lungs within months of getting his COVID injection. He also developed other tumors, including ones that grew along the vertebrae of his spine. Hoffe notes that the prognosis at the time was that the man would almost certainly die due to the aggressive cancers.
(17/57) DR. MICHAEL HUANG—“The clinic I work at, it's about 30 physicians…in the past year, I've learned that two out of the 30 physicians I work with were diagnosed with aggressive advanced cancer, and one of them died because of that.”
Starting off our testimonies portion of this turbo-cancer mega-thread, we have Dr. Michael Huang, a family medicine physician in California, describing during a 2024 conversation with Charles Kovess, et al. how he started to see aggressive cancers crop up in his colleagues following the rollout of the COVID injections.
Huang tells Kovess, et al.:
“I have seen what has happened when my friends have taken the shots. I used to work at Kaiser. It's a large management group. And the clinic I work at, it's about 30 physicians. And, you know, physicians, we are usually trying to stay healthy, trying to avoid harms. We don't smoke. We don't drink. And, unfortunately, in the past year, I've learned that two out of the 30 physicians I work with were diagnosed with aggressive advanced cancer, and one of them died because of that. Almost monthly, I will hear about one or two physicians [who] die suddenly. And most recently, we know this family practice resident who's in his thirties. We have seen him about a month ago, healthy, vibrant, and he suddenly died of advanced gastric cancer and left an unborn child as a result. So we start to see the results of healthcare providers playing Russian Roulette, getting the shots as they're…leading their patients, setting examples, getting their booster shots and getting injured from these experimental vaccines.”
Starting off our testimonies portion of this turbo-cancer mega-thread, we have Dr. Michael Huang, a family medicine physician in California, describing during a 2024 conversation with Charles Kovess, et al. how he started to see aggressive cancers crop up in his colleagues following the rollout of the COVID injections.
Huang tells Kovess, et al.:
“I have seen what has happened when my friends have taken the shots. I used to work at Kaiser. It's a large management group. And the clinic I work at, it's about 30 physicians. And, you know, physicians, we are usually trying to stay healthy, trying to avoid harms. We don't smoke. We don't drink. And, unfortunately, in the past year, I've learned that two out of the 30 physicians I work with were diagnosed with aggressive advanced cancer, and one of them died because of that. Almost monthly, I will hear about one or two physicians [who] die suddenly. And most recently, we know this family practice resident who's in his thirties. We have seen him about a month ago, healthy, vibrant, and he suddenly died of advanced gastric cancer and left an unborn child as a result. So we start to see the results of healthcare providers playing Russian Roulette, getting the shots as they're…leading their patients, setting examples, getting their booster shots and getting injured from these experimental vaccines.”
(18/57) NURSE DAWN—“This is a huge tumor about the size of a softball behind my eye. And I had [metastases] to the back of my skull and 12 different areas of my bones.”
In this clip taken from a 2023 interview with Children’s Health Defense, Dawn, a nurse, describes how she developed cancers throughout her body after receiving two Moderna COVID injections. Dawn describes how the cancer is “muscle-loving,” appearing throughout her body, and did not respond to treatment.
Dawn also shows how she developed a “huge tumor about the size of a softball” behind her eye” and had “[metastases] to the back of [her] skull and 12 different areas of [her] bones.”
In this clip taken from a 2023 interview with Children’s Health Defense, Dawn, a nurse, describes how she developed cancers throughout her body after receiving two Moderna COVID injections. Dawn describes how the cancer is “muscle-loving,” appearing throughout her body, and did not respond to treatment.
Dawn also shows how she developed a “huge tumor about the size of a softball” behind her eye” and had “[metastases] to the back of [her] skull and 12 different areas of [her] bones.”
(19/57) MODERNA COVID INJECTION–TRIAL PARTICIPANT—“I know I got this vaccine that's caused me to have a rare cancer that has progressed way faster than it was supposed to.”
In this clip from a HighWire segment, we hear from a participant of Moderna’s COVID-injection “clinical trial” describe how she developed T-cell lymphoma—a type of cancer that originates from T cells, a type of white blood cell in the immune system—following receipt of her injection.
Since being diagnosed, the trial participant notes that she’s been to the doctor approximately 200 times and has had four surgeries. Despite the doctors’ visits and surgeries, however, the participant notes her cancer has only become “worse.”
In this clip from a HighWire segment, we hear from a participant of Moderna’s COVID-injection “clinical trial” describe how she developed T-cell lymphoma—a type of cancer that originates from T cells, a type of white blood cell in the immune system—following receipt of her injection.
Since being diagnosed, the trial participant notes that she’s been to the doctor approximately 200 times and has had four surgeries. Despite the doctors’ visits and surgeries, however, the participant notes her cancer has only become “worse.”
(20/57) JILL KLEISS— “Shortly after I had my vaccine, two weeks later, I went to have my routine mammogram…[months later] I insisted on a biopsy…[and was told I] have the same breast cancer again [that I had prior to the ‘vaccine’] on the other side.”
In this clip we hear from Jill Kleiss, also known as the Chemo Dancer on YouTube, who describes how she developed breast cancer following her COVID injection. Kleiss, who had had breast cancer prior to receiving the injection, developed cancer in the breast that had previously been healthy and cancer-free.
In this clip we hear from Jill Kleiss, also known as the Chemo Dancer on YouTube, who describes how she developed breast cancer following her COVID injection. Kleiss, who had had breast cancer prior to receiving the injection, developed cancer in the breast that had previously been healthy and cancer-free.
(21/57) CHILDREN’S HEALTH DEFENSE BUS STORY—“[After receiving his COVID injection], all of the sudden he had multiple cancers, fluid buildup around the heart, [and] pneumonia.”
In this clip from a Children’s Health Defense bus story, we hear from a gentleman who describes a cousin of his who developed brain and lung cancer following receipt of his COVID injection. The gentleman notes that his cousin subsequently died—the time between the development of the cancers and death was less than a year.
In this clip from a Children’s Health Defense bus story, we hear from a gentleman who describes a cousin of his who developed brain and lung cancer following receipt of his COVID injection. The gentleman notes that his cousin subsequently died—the time between the development of the cancers and death was less than a year.
(22/57) CHILDREN’S HEALTH DEFENSE BUS STORY—”I…have three aunts that had turbo cancer from the COVID shot. They all died last year. Within months of each other.”
A woman describes for Children’s Health Defense how three of her aunts all developed turbo cancer following their receipt of one or more COVID injections. She notes they all died within months of each other.
A woman describes for Children’s Health Defense how three of her aunts all developed turbo cancer following their receipt of one or more COVID injections. She notes they all died within months of each other.
(23/57) JEREMIAH’S AUNT, NANCY ARCHER—“I think [it] took, from her last shot, approximately, 12 months to get to that point where medicine didn’t even think they had an answer [for her cancer].”
In this Children’s Health Defense bus interview, we hear from Jeremiah, who describes how his aunt, Nancy Archer, died of turbo cancer following receipt of a Pfizer COVID injection.
“It was heartbreaking to watch her succumb to turbo cancer from the effects of the shot,” Jeremiah says. He notes that she only took the injection because she wanted to ensure that she could travel freely between her homes in the U.S. and Guatemala. The timespan between Nancy’s receipt of her final Pfizer injection and her turbo cancer–caused death was approximately one year according to Jeremiah.
In this Children’s Health Defense bus interview, we hear from Jeremiah, who describes how his aunt, Nancy Archer, died of turbo cancer following receipt of a Pfizer COVID injection.
“It was heartbreaking to watch her succumb to turbo cancer from the effects of the shot,” Jeremiah says. He notes that she only took the injection because she wanted to ensure that she could travel freely between her homes in the U.S. and Guatemala. The timespan between Nancy’s receipt of her final Pfizer injection and her turbo cancer–caused death was approximately one year according to Jeremiah.
(24/57) 2024 Study Published in Cureus Shows Significant Cancer Increase in Japan Following the Rollout of the COVID Injections in the Country
Title: Increased Age-Adjusted Cancer Mortality After the Third mRNA-Lipid Nanoparticle Vaccine Dose During the COVID-19 Pandemic in Japan
Authors: Miki Gibo, et al.
Published: April 8, 2024
Journal: Cureus
Key excerpts: “No significant excess mortality was observed during the first year of the pandemic (2020). However, some excess cancer mortalities were observed in 2021 after mass vaccination with the first and second vaccine doses, and significant excess mortalities were observed for all cancers and some specific types of cancer (including ovarian cancer, leukemia, prostate cancer, lip/oral/pharyngeal cancer, pancreatic cancer, and breast cancer) after mass vaccination with the third dose in 2022.”
“In 2020, the first year of the pandemic, there was significant deficit mortality for all causes (< 99% lower PI) and no excess mortality for all cancers. However, in 2021, there was significant excess mortality of 2.1% (>99% upper PI) for all causes and 1.1% (>95% upper PI) for all cancers. In 2022, the excesses increased to 9.6% (>99% upper PI) for all causes and 2.1% (>99% upper PI) for all cancers. In 2022, the number of excess deaths was 115,799 (95%CI: 106,018, 125,501) for all causes and 7,162 (95%CI: 4,786, 9,522) for all cancers.”
Link: proquest.com/openview/45137…
Title: Increased Age-Adjusted Cancer Mortality After the Third mRNA-Lipid Nanoparticle Vaccine Dose During the COVID-19 Pandemic in Japan
Authors: Miki Gibo, et al.
Published: April 8, 2024
Journal: Cureus
Key excerpts: “No significant excess mortality was observed during the first year of the pandemic (2020). However, some excess cancer mortalities were observed in 2021 after mass vaccination with the first and second vaccine doses, and significant excess mortalities were observed for all cancers and some specific types of cancer (including ovarian cancer, leukemia, prostate cancer, lip/oral/pharyngeal cancer, pancreatic cancer, and breast cancer) after mass vaccination with the third dose in 2022.”
“In 2020, the first year of the pandemic, there was significant deficit mortality for all causes (< 99% lower PI) and no excess mortality for all cancers. However, in 2021, there was significant excess mortality of 2.1% (>99% upper PI) for all causes and 1.1% (>95% upper PI) for all cancers. In 2022, the excesses increased to 9.6% (>99% upper PI) for all causes and 2.1% (>99% upper PI) for all cancers. In 2022, the number of excess deaths was 115,799 (95%CI: 106,018, 125,501) for all causes and 7,162 (95%CI: 4,786, 9,522) for all cancers.”
Link: proquest.com/openview/45137…


(25/57) “Five case reports of 71, 40, 76, 55, and 75 years old with diagnoses of colon cancer, breast cancer, skin cancer, and gastric cancer in the last two patients respectively days and months after receiving the second, third and fourth doses of the COVID-19 vaccine.”
Title: Which Could Be the Risk Factors for Developing Cancer After Receiving The COVID-19 Vaccine?
Authors: Huang, W. L
Published: January 28, 2023
Journal: International Journal of Cancer Research & Therapy
Key Excerpts: “There are several articles in the literature after the COVID-19 pandemic showing the necessity of vaccinating people who have a cancer diagnosis to prevent this disease in this group of patients. But what I want to report in this article is that I am facing an increasing number of cases of patients with cancer after receiving COVID-19 vaccines and this is what I want to describe in this study, using the thoughts of Hippocrates (460 bce - 375 bce), the father of medicine, that said that ‘it is more important to consider other ancient medical traditions prior to the knowledge we have nowadays.’”
“Five case reports of 71, 40, 76, 55, and 75 years old with diagnoses of colon cancer, breast cancer, skin cancer, and gastric cancer in the last two patients respectively days and months after receiving the second, third and fourth doses of the COVID-19 vaccine.”
“The conclusion of this study is that patients that are developing cancer after receiving the COVID-19 vaccine have in common, energy deficiency inside the five internal massive organs (and these alterations are the factors to induce cancer formation according to traditional Chinese medicine) and the use of this kind of vaccine has the potential to reduce even more the vital energy of the patient which is already very low and leading to a weakness state of the immune system and increasing the chance to have any kind of chronic diseases, in this case, cancer.”
Link: opastpublishers.com/open-access-ar…
Title: Which Could Be the Risk Factors for Developing Cancer After Receiving The COVID-19 Vaccine?
Authors: Huang, W. L
Published: January 28, 2023
Journal: International Journal of Cancer Research & Therapy
Key Excerpts: “There are several articles in the literature after the COVID-19 pandemic showing the necessity of vaccinating people who have a cancer diagnosis to prevent this disease in this group of patients. But what I want to report in this article is that I am facing an increasing number of cases of patients with cancer after receiving COVID-19 vaccines and this is what I want to describe in this study, using the thoughts of Hippocrates (460 bce - 375 bce), the father of medicine, that said that ‘it is more important to consider other ancient medical traditions prior to the knowledge we have nowadays.’”
“Five case reports of 71, 40, 76, 55, and 75 years old with diagnoses of colon cancer, breast cancer, skin cancer, and gastric cancer in the last two patients respectively days and months after receiving the second, third and fourth doses of the COVID-19 vaccine.”
“The conclusion of this study is that patients that are developing cancer after receiving the COVID-19 vaccine have in common, energy deficiency inside the five internal massive organs (and these alterations are the factors to induce cancer formation according to traditional Chinese medicine) and the use of this kind of vaccine has the potential to reduce even more the vital energy of the patient which is already very low and leading to a weakness state of the immune system and increasing the chance to have any kind of chronic diseases, in this case, cancer.”
Link: opastpublishers.com/open-access-ar…
(26/57) “We report on an aggressive, infiltrating, metastatic, and ultimately lethal basaloid type of carcinoma arising shortly after an mRNA vaccination for COVID-19…We propose that the vaccine can cause suppression of the immune system, which leads to accelerated cancer progression.”
Title: Bell’s palsy or an aggressive infiltrating basaloid carcinoma post-mRNA vaccination for COVID-19? A case report and review of the literature
Authors: Anthony M Kyriakopoulos, et al.
Published: September 15, 2023
Journal: Journal of Experimental and Clinical Sciences
Key Excerpts: “We report on an aggressive, infiltrating, metastatic, and ultimately lethal basaloid type of carcinoma arising shortly after an mRNA vaccination for COVID-19…We propose that the vaccine can cause suppression of the immune system, which leads to accelerated cancer progression.”
“In this study we describe all aspects of this case and discuss possible causal links between the rapid emergence of this metastatic cancer and mRNA vaccination. We place this within the context of multiple immune impairments potentially related to the mRNA injections that would be expected to potentiate more aggressive presentation and progression of cancer. The type of malignancy we describe suggests a population risk for occurrence of a large variety of relatively common basaloid phenotype cancer cells, which may have the potential for metastatic disease.”
Link: pmc.ncbi.nlm.nih.gov/articles/PMC10…
Title: Bell’s palsy or an aggressive infiltrating basaloid carcinoma post-mRNA vaccination for COVID-19? A case report and review of the literature
Authors: Anthony M Kyriakopoulos, et al.
Published: September 15, 2023
Journal: Journal of Experimental and Clinical Sciences
Key Excerpts: “We report on an aggressive, infiltrating, metastatic, and ultimately lethal basaloid type of carcinoma arising shortly after an mRNA vaccination for COVID-19…We propose that the vaccine can cause suppression of the immune system, which leads to accelerated cancer progression.”
“In this study we describe all aspects of this case and discuss possible causal links between the rapid emergence of this metastatic cancer and mRNA vaccination. We place this within the context of multiple immune impairments potentially related to the mRNA injections that would be expected to potentiate more aggressive presentation and progression of cancer. The type of malignancy we describe suggests a population risk for occurrence of a large variety of relatively common basaloid phenotype cancer cells, which may have the potential for metastatic disease.”
Link: pmc.ncbi.nlm.nih.gov/articles/PMC10…



(27/57) “Evidence is provided that adding 100 % of N1-methyl-pseudouridine (m1Ψ) to the mRNA vaccine in a melanoma model stimulated cancer growth and metastasis…Based on this compelling evidence, we suggest that future clinical trials for cancers or infectious diseases should not use mRNA vaccines with a 100 % m1Ψ modification, but rather ones with the lower percentage of m1Ψ modification to avoid immune suppression.”
Title: Review: N1-methyl-pseudouridine (m1Ψ): Friend or foe of cancer?
Authors: Alberto Rubio-Casillas, et al.
Published: May 2024
Journal: International Journal of Biological Macromolecules
Key Excerpts: “Evidence is provided that adding 100 % of N1-methyl-pseudouridine (m1Ψ) to the mRNA vaccine in a melanoma model stimulated cancer growth and metastasis…Based on this compelling evidence, we suggest that future clinical trials for cancers or infectious diseases should not use mRNA vaccines with a 100 % m1Ψ modification, but rather ones with the lower percentage of m1Ψ modification to avoid immune suppression.”
Link: sciencedirect.com/science/articl…
Title: Review: N1-methyl-pseudouridine (m1Ψ): Friend or foe of cancer?
Authors: Alberto Rubio-Casillas, et al.
Published: May 2024
Journal: International Journal of Biological Macromolecules
Key Excerpts: “Evidence is provided that adding 100 % of N1-methyl-pseudouridine (m1Ψ) to the mRNA vaccine in a melanoma model stimulated cancer growth and metastasis…Based on this compelling evidence, we suggest that future clinical trials for cancers or infectious diseases should not use mRNA vaccines with a 100 % m1Ψ modification, but rather ones with the lower percentage of m1Ψ modification to avoid immune suppression.”
Link: sciencedirect.com/science/articl…

(28/57) “Treg responses produced after mRNA vaccination and the subsequent mRNA-encoded SARS-CoV-2 spike protein expression may lead to a harmful influence on the immune system of vaccinees, and subsequent accelerated development of cancer and autoimmune disease.”
Title: Oncogenesis and autoimmunity as a result of mRNA COVID-19 vaccination
Authors: Anthony M Kyriakopoulos, et al.
Published: April 23, 2024
Journal: TechRxiv PREPRINT
Key Excerpts: “In summary, the Treg responses produced after mRNA vaccination and the subsequent mRNA-encoded SARS-CoV-2 spike protein expression may lead to a harmful influence on the immune system of vaccinees, and subsequent accelerated development of cancer and autoimmune disease. These mechanisms are consistent with both epidemiological findings and case reports.”
Link: techrxiv.org/doi/full/10.22…
Title: Oncogenesis and autoimmunity as a result of mRNA COVID-19 vaccination
Authors: Anthony M Kyriakopoulos, et al.
Published: April 23, 2024
Journal: TechRxiv PREPRINT
Key Excerpts: “In summary, the Treg responses produced after mRNA vaccination and the subsequent mRNA-encoded SARS-CoV-2 spike protein expression may lead to a harmful influence on the immune system of vaccinees, and subsequent accelerated development of cancer and autoimmune disease. These mechanisms are consistent with both epidemiological findings and case reports.”
Link: techrxiv.org/doi/full/10.22…

(29/57) “In this report, a rare case of primary cutaneous adenoid cystic carcinoma (PCACC) localized in the subcutaneous tissue of the scapular region that grew after BNT162b2 corona virus disease of 2019 (COVID-19) vaccination…The BNT162b2 mRNA vaccine has been associated with a multisystem inflammatory syndrome (MIS-V). A comparable immune reaction could potentially enhance tumor growth rate.”
Title: Primary Cutaneous Adenoid Cystic Carcinoma in a Rare Location With an Immune Response to a BNT162b2 Vaccine
Authors: Yilmaz, Abdurrahman, et al.
Published: April–June 2024
Journal: JBJS Case Connector
Key Excerpts: “In this report, a rare case of primary cutaneous adenoid cystic carcinoma (PCACC) localized in the subcutaneous tissue of the scapular region that grew after BNT162b2 corona virus disease of 2019 (COVID-19) vaccination is presented and may be explained by CD4 and CD8 cell infiltration. The BNT162b2 mRNA vaccine has been associated with a multisystem inflammatory syndrome (MIS-V). A comparable immune reaction could potentially enhance tumor growth rate.”
Link: journals.lww.com/jbjscc/abstrac…
Title: Primary Cutaneous Adenoid Cystic Carcinoma in a Rare Location With an Immune Response to a BNT162b2 Vaccine
Authors: Yilmaz, Abdurrahman, et al.
Published: April–June 2024
Journal: JBJS Case Connector
Key Excerpts: “In this report, a rare case of primary cutaneous adenoid cystic carcinoma (PCACC) localized in the subcutaneous tissue of the scapular region that grew after BNT162b2 corona virus disease of 2019 (COVID-19) vaccination is presented and may be explained by CD4 and CD8 cell infiltration. The BNT162b2 mRNA vaccine has been associated with a multisystem inflammatory syndrome (MIS-V). A comparable immune reaction could potentially enhance tumor growth rate.”
Link: journals.lww.com/jbjscc/abstrac…

(30/57) “mRNA vaccine boosters may impair immune system response in immune compromised individuals. Multiple doses of the mRNA COVID-19 vaccines may result in much higher levels of IgG 4 antibodies, or also impaired activation of CD4 + and CD8 + T cells.”
Title: mRNA vaccine boosters and impaired immune system response in immune compromised individuals: a narrative review
Authors: Alberto Boretti
Published: January 27, 2024
Journal: Clinical and Experimental Medicine
Key Excerpts: “mRNA vaccine boosters may impair immune system response in immune compromised individuals. Multiple doses of the mRNA COVID-19 vaccines may result in much higher levels of IgG 4 antibodies, or also impaired activation of CD4 + and CD8 + T cells.”
Link: link.springer.com/article/10.100…
Title: mRNA vaccine boosters and impaired immune system response in immune compromised individuals: a narrative review
Authors: Alberto Boretti
Published: January 27, 2024
Journal: Clinical and Experimental Medicine
Key Excerpts: “mRNA vaccine boosters may impair immune system response in immune compromised individuals. Multiple doses of the mRNA COVID-19 vaccines may result in much higher levels of IgG 4 antibodies, or also impaired activation of CD4 + and CD8 + T cells.”
Link: link.springer.com/article/10.100…

(31/57) “The mRNA vaccines potentially cause increased risk to infectious diseases and cancer.”
Title: Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs
Authors: Stephanie Seneff, et al.
Published: June 2022
Journal: Food and Chemical Toxicology
Key Excerpts: “The mRNA vaccines potentially cause increased risk to infectious diseases and cancer.”
“In this paper, we present evidence that vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance.”
“These vaccinations have now been shown to downregulate critical pathways related to cancer surveillance, infection control, and cellular homeostasis.”
Link: sciencedirect.com/science/articl…
Title: Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs
Authors: Stephanie Seneff, et al.
Published: June 2022
Journal: Food and Chemical Toxicology
Key Excerpts: “The mRNA vaccines potentially cause increased risk to infectious diseases and cancer.”
“In this paper, we present evidence that vaccination induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health. Immune cells that have taken up the vaccine nanoparticles release into circulation large numbers of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites. We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance.”
“These vaccinations have now been shown to downregulate critical pathways related to cancer surveillance, infection control, and cellular homeostasis.”
Link: sciencedirect.com/science/articl…



(32/57) “In this report we describe the case of a healthy, young, athletic woman who developed acute lymphoblastic leukaemia (ALL)/lymphoblastic lymphoma (LBL) after receiving the second dose of the Pfizer/BioNTech modified mRNA (modRNA) COVID-19 genetic vaccine (marketed as Comirnaty)”
Title: A Case Report of Acute Lymphoblastic Leukaemia (ALL)/Lymphoblastic Lymphoma (LBL) Following the Second Dose of Comirnaty: An Analysis of the Potential Pathogenic Mechanism Based on of the Existing Literature
Authors: Patrizia Gentilini, et al.
Published: Posted April 1, 2024
Journal: PREPRINT
Key Excerpts: “In this report we describe the case of a healthy, young, athletic woman who developed acute lymphoblastic leukaemia (ALL)/lymphoblastic lymphoma (LBL) after receiving the second dose of the Pfizer/BioNTech modified mRNA (modRNA) COVID-19 genetic vaccine (marketed as Comirnaty)”
“A time interval of 16 weeks from the second vaccination to the diagnosis of cancer was noted.”
Link: researchgate.net/profile/Panagi…
Title: A Case Report of Acute Lymphoblastic Leukaemia (ALL)/Lymphoblastic Lymphoma (LBL) Following the Second Dose of Comirnaty: An Analysis of the Potential Pathogenic Mechanism Based on of the Existing Literature
Authors: Patrizia Gentilini, et al.
Published: Posted April 1, 2024
Journal: PREPRINT
Key Excerpts: “In this report we describe the case of a healthy, young, athletic woman who developed acute lymphoblastic leukaemia (ALL)/lymphoblastic lymphoma (LBL) after receiving the second dose of the Pfizer/BioNTech modified mRNA (modRNA) COVID-19 genetic vaccine (marketed as Comirnaty)”
“A time interval of 16 weeks from the second vaccination to the diagnosis of cancer was noted.”
Link: researchgate.net/profile/Panagi…


(33/57) “We report a case of neuropsychiatric symptoms and refractory HLH in a woman with systemic lupus erythematosus (SLE) after receiving her COVID-19 vaccine treated with belimumab, later found to have intravascular large B-cell lymphoma (IVLBCL) at autopsy.”
Title: Fatal hemophagocytic lymphohistiocytosis with intravascular large B-cell lymphoma following coronavirus disease 2019 vaccination in a patient with systemic lupus erythematosus: an intertwined case
Authors: Yusuke Ueda, et al.
Published: November 6, 2023
Journal: Immunological Medicine
Key Excerpts: “We report a case of neuropsychiatric symptoms and refractory HLH in a woman with systemic lupus erythematosus (SLE) after receiving her COVID-19 vaccine treated with belimumab, later found to have intravascular large B-cell lymphoma (IVLBCL) at autopsy.”
Link: tandfonline.com/doi/full/10.10…
Title: Fatal hemophagocytic lymphohistiocytosis with intravascular large B-cell lymphoma following coronavirus disease 2019 vaccination in a patient with systemic lupus erythematosus: an intertwined case
Authors: Yusuke Ueda, et al.
Published: November 6, 2023
Journal: Immunological Medicine
Key Excerpts: “We report a case of neuropsychiatric symptoms and refractory HLH in a woman with systemic lupus erythematosus (SLE) after receiving her COVID-19 vaccine treated with belimumab, later found to have intravascular large B-cell lymphoma (IVLBCL) at autopsy.”
Link: tandfonline.com/doi/full/10.10…

(34/57) “After reviewing the available literature, we are particularly concerned that certain COVID-19 vaccines may generate a pro-tumorigenic milieu (i.e., a specific environment that could lead to neoplastic transformation) that predisposes some (stable) oncologic patients and survivors to cancer progression, recurrence, and/or metastasis.”
Title: SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis
Authors: Raquel Valdes Angues, et al.
Published: December 17, 2023
Journal: Cureus
Key Excerpts: “After reviewing the available literature, we are particularly concerned that certain COVID-19 vaccines may generate a pro-tumorigenic milieu (i.e., a specific environment that could lead to neoplastic transformation) that predisposes some (stable) oncologic patients and survivors to cancer progression, recurrence, and/or metastasis.”
Link: pmc.ncbi.nlm.nih.gov/articles/PMC10…
Title: SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis
Authors: Raquel Valdes Angues, et al.
Published: December 17, 2023
Journal: Cureus
Key Excerpts: “After reviewing the available literature, we are particularly concerned that certain COVID-19 vaccines may generate a pro-tumorigenic milieu (i.e., a specific environment that could lead to neoplastic transformation) that predisposes some (stable) oncologic patients and survivors to cancer progression, recurrence, and/or metastasis.”
Link: pmc.ncbi.nlm.nih.gov/articles/PMC10…


(35/57) “We present a rare case of metastatic prostate cancer diagnosed after initially presenting as generalized lymphadenopathy following a coronavirus disease 2019 (COVID) booster vaccination.”
Title: Metastatic prostatic adenocarcinoma presenting as generalized lymphadenopathy unmasked by a COVID booster vaccine
Authors: Kavya Bharathidasan, et al.
Published: November 28, 2023
Journal: Clinical Case Reports
Key Excerpts: “We present a rare case of metastatic prostate cancer diagnosed after initially presenting as generalized lymphadenopathy following a coronavirus disease 2019 (COVID) booster vaccination.”
Link: onlinelibrary.wiley.com/doi/full/10.10…
Title: Metastatic prostatic adenocarcinoma presenting as generalized lymphadenopathy unmasked by a COVID booster vaccine
Authors: Kavya Bharathidasan, et al.
Published: November 28, 2023
Journal: Clinical Case Reports
Key Excerpts: “We present a rare case of metastatic prostate cancer diagnosed after initially presenting as generalized lymphadenopathy following a coronavirus disease 2019 (COVID) booster vaccination.”
Link: onlinelibrary.wiley.com/doi/full/10.10…

(36/57) “Our results raise grave concerns regarding the safety of the BNT162b2 vaccine and call for an immediate halt of all RNA biologicals unless these concerns can be dispelled.”
Title: BioNTech RNA-Based COVID-19 Injections Contain Large Amounts Of Residual DNA Including An SV40 Promoter/Enhancer Sequence
Authors: Ulrike Kämmerer, et al.
Published: December 3, 2024
Journal: Science, Public Health Policy and the Law
Key Excerpts: “We further analyzed RNA and DNA contents of these vials and identified large amounts of DNA after RNase A digestion in all lots with concentrations ranging from 32.7 ng to 43.4 ng per clinical dose. This far exceeds the maximal acceptable concentration of 10 ng per clinical dose that has been set by international regulatory authorities.”
“Our results raise grave concerns regarding the safety of the BNT162b2 vaccine and call for an immediate halt of all RNA biologicals unless these concerns can be dispelled.”
Link: publichealthpolicyjournal.com/biontech-rna-b…
Title: BioNTech RNA-Based COVID-19 Injections Contain Large Amounts Of Residual DNA Including An SV40 Promoter/Enhancer Sequence
Authors: Ulrike Kämmerer, et al.
Published: December 3, 2024
Journal: Science, Public Health Policy and the Law
Key Excerpts: “We further analyzed RNA and DNA contents of these vials and identified large amounts of DNA after RNase A digestion in all lots with concentrations ranging from 32.7 ng to 43.4 ng per clinical dose. This far exceeds the maximal acceptable concentration of 10 ng per clinical dose that has been set by international regulatory authorities.”
“Our results raise grave concerns regarding the safety of the BNT162b2 vaccine and call for an immediate halt of all RNA biologicals unless these concerns can be dispelled.”
Link: publichealthpolicyjournal.com/biontech-rna-b…
(37/57) “These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold.”
Title: DNA fragments detected in monovalent and bivalent 2 Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events
Authors: David J. Speicher, et al.
Journal: PREPRINT
Key Excerpts: “These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold…Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs.”
Link: osf.io/preprints/osf/…
Title: DNA fragments detected in monovalent and bivalent 2 Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events
Authors: David J. Speicher, et al.
Journal: PREPRINT
Key Excerpts: “These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold…Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs.”
Link: osf.io/preprints/osf/…
(38/57) “We conclude that the SV40 origin of replication and early control region are sufficient viral components for the genomic instability at sites of SV40 integration and that SV40 T Ag is not required.”
Title: The genomic instability associated with integrated simian virus 40 DNA is dependent on the origin of replication and early control region
Authors: D J Hunter, et al.
Published: February 1, 1994
Journal: Journal of Virology
Key Excerpts: “We conclude that the SV40 origin of replication and early control region are sufficient viral components for the genomic instability at sites of SV40 integration and that SV40 T Ag is not required.”
Link: journals.asm.org/doi/10.1128/jv…
Title: The genomic instability associated with integrated simian virus 40 DNA is dependent on the origin of replication and early control region
Authors: D J Hunter, et al.
Published: February 1, 1994
Journal: Journal of Virology
Key Excerpts: “We conclude that the SV40 origin of replication and early control region are sufficient viral components for the genomic instability at sites of SV40 integration and that SV40 T Ag is not required.”
Link: journals.asm.org/doi/10.1128/jv…

(39/57) “Residual DNA might be a risk to your final product because of oncogenic and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration.”
Title: Guidance for Industry Characterization and Qualification of Cell Substrates and Other Biological Materials Used in the Production of Viral Vaccines for Infectious Disease Indications
Authors: The Food and Drug Administration (FDA)
Key Excerpts: “Residual DNA might be a risk to your final product because of oncogenic and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration.”
Link: fda.gov/media/78428/do…
Title: Guidance for Industry Characterization and Qualification of Cell Substrates and Other Biological Materials Used in the Production of Viral Vaccines for Infectious Disease Indications
Authors: The Food and Drug Administration (FDA)
Key Excerpts: “Residual DNA might be a risk to your final product because of oncogenic and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration.”
Link: fda.gov/media/78428/do…


(40/57) SENIOR RESEARCH SCIENTIST STEPHANIE SENEFF—"Ninety-eight percent [98%] of the mentions of cancer [in VAERS in 2021] were COVID vaccines...This is just very striking to me that cancer is something that these vaccines cause that other vaccines don't cause..."
To start the VAERS portion of this turbo-cancer mega thread, we have senior research scientist at MIT Stephanie Seneff describing for Dr. William Makis, Zen Honeycutt, et al. how the COVID injections are heavily associated with various cancers according to numerous reports in VAERS.
"Ninety-eight percent [98%] of the mentions of cancer [in VAERS in 2021] were COVID vaccines," Seneff says. "It's hugely more highly represented than the number of COVID vaccines that were received in that year, so it's way out of line with the other [non-COVID] vaccines."
"This is just very striking to me that cancer is something that these vaccines cause that other vaccines don't cause," Seneff adds. She notes that for VAERS reports of cancer regarding flu jabs, there are "practically none," which means the ratio of how often the COVID injections cause cancer versus flu jabs is "infinity."
As for mechanism of action, Seneff highlights one paper describing PD-L1 overexpression as a result of the COVID injections, which, in turn, can increase one's odds of developing cancer. (PD-L1, Seneff notes, is a "molecule that's produced by both cancer cells and immune cells" that "prevents... immune cells from responding to both the... COVID virus, but also to cancer.")
Seneff notes that the paper shows a "dramatic difference" in overexpression of PD-L1 in the control group versus the group recently injected with the COVID jabs, with the latter group showing far more of it.
To start the VAERS portion of this turbo-cancer mega thread, we have senior research scientist at MIT Stephanie Seneff describing for Dr. William Makis, Zen Honeycutt, et al. how the COVID injections are heavily associated with various cancers according to numerous reports in VAERS.
"Ninety-eight percent [98%] of the mentions of cancer [in VAERS in 2021] were COVID vaccines," Seneff says. "It's hugely more highly represented than the number of COVID vaccines that were received in that year, so it's way out of line with the other [non-COVID] vaccines."
"This is just very striking to me that cancer is something that these vaccines cause that other vaccines don't cause," Seneff adds. She notes that for VAERS reports of cancer regarding flu jabs, there are "practically none," which means the ratio of how often the COVID injections cause cancer versus flu jabs is "infinity."
As for mechanism of action, Seneff highlights one paper describing PD-L1 overexpression as a result of the COVID injections, which, in turn, can increase one's odds of developing cancer. (PD-L1, Seneff notes, is a "molecule that's produced by both cancer cells and immune cells" that "prevents... immune cells from responding to both the... COVID virus, but also to cancer.")
Seneff notes that the paper shows a "dramatic difference" in overexpression of PD-L1 in the control group versus the group recently injected with the COVID jabs, with the latter group showing far more of it.
(41/57) VAERS ID 1220913: “HUSBAND DIED BECAUSE OF TERMINAL PANCREATIC CANCER.” (One dose of Moderna’s COVID injection.)
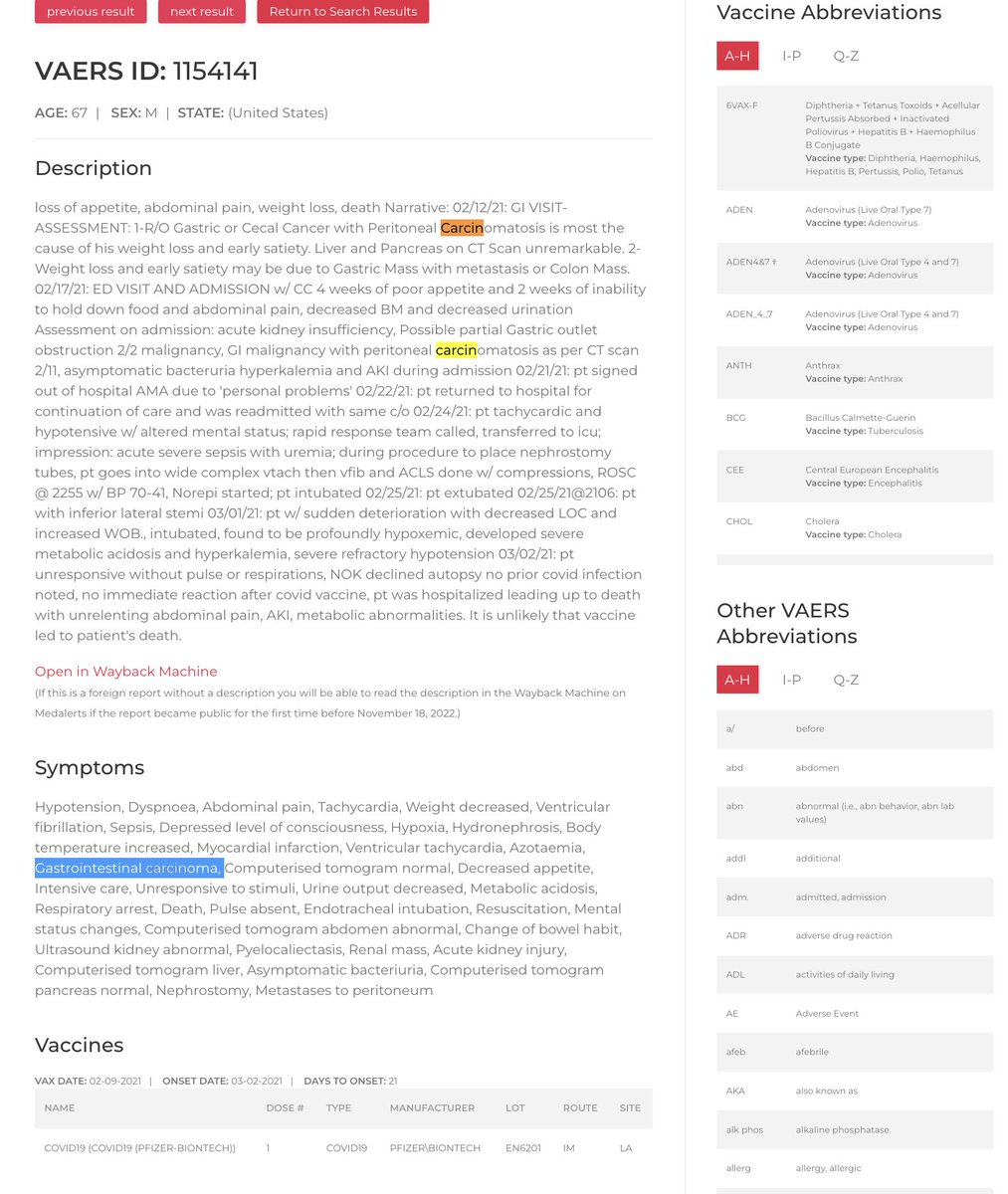

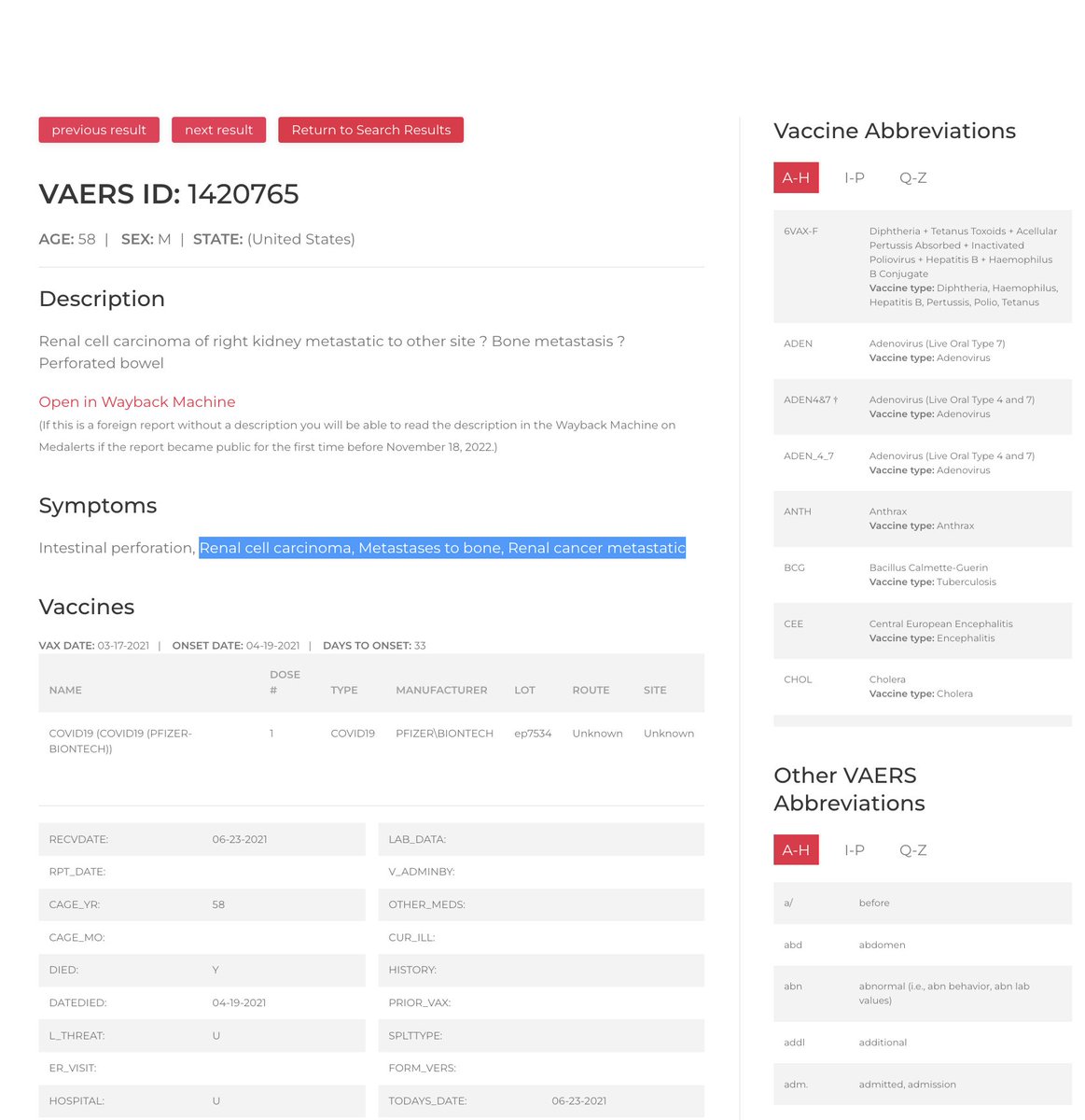

(42/57) VAERS ID 2184304: “HE HAD 2 LUMBAR SPINE X-RAYS ON OR ABOUT JULY 16, 2021, WHICH SHOWED LESIONS ON HIS SPINE…FROM THAT POINT ON I WATCHED THE TUMORS APPEAR ON HIS BODY AND HEAD. HE DIED 9/7/2021.” (Two doses of Moderna’s COVID injection.)
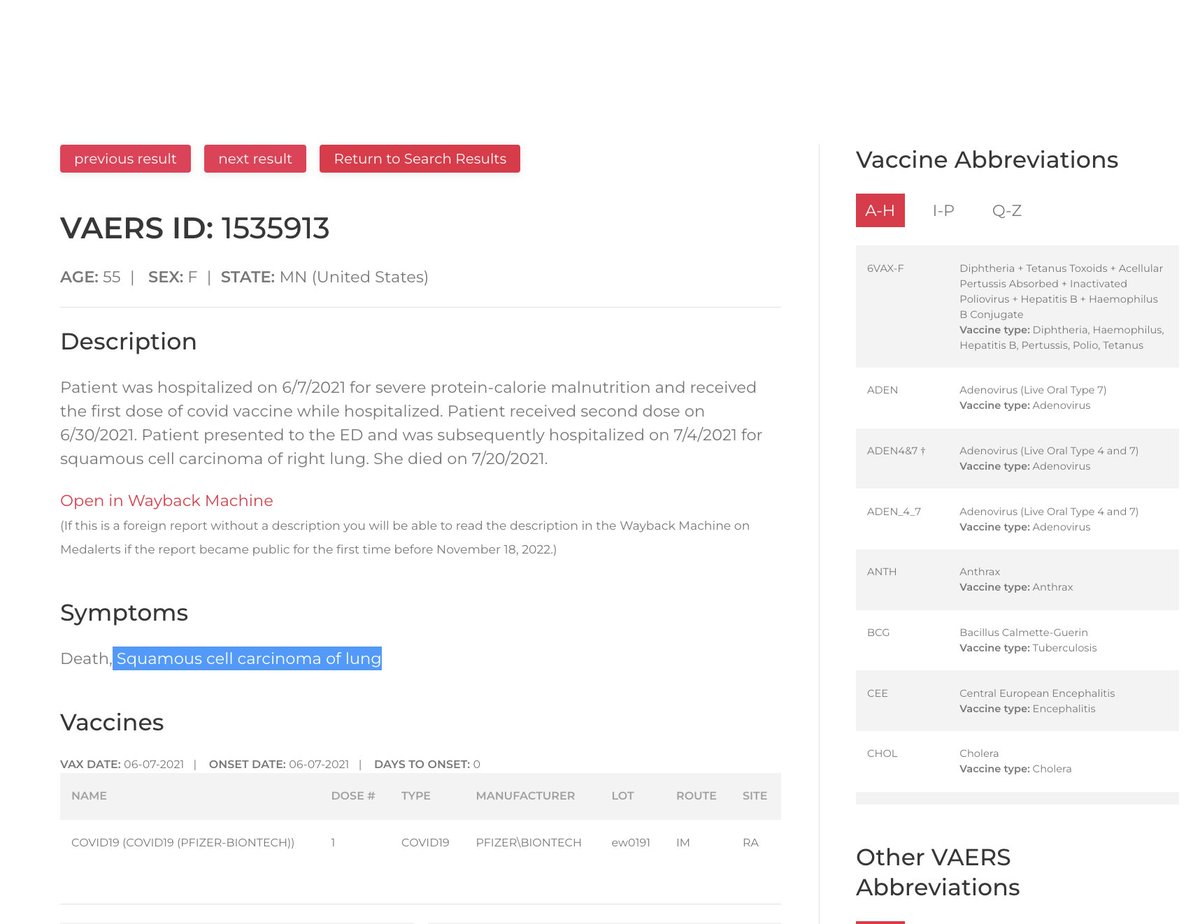

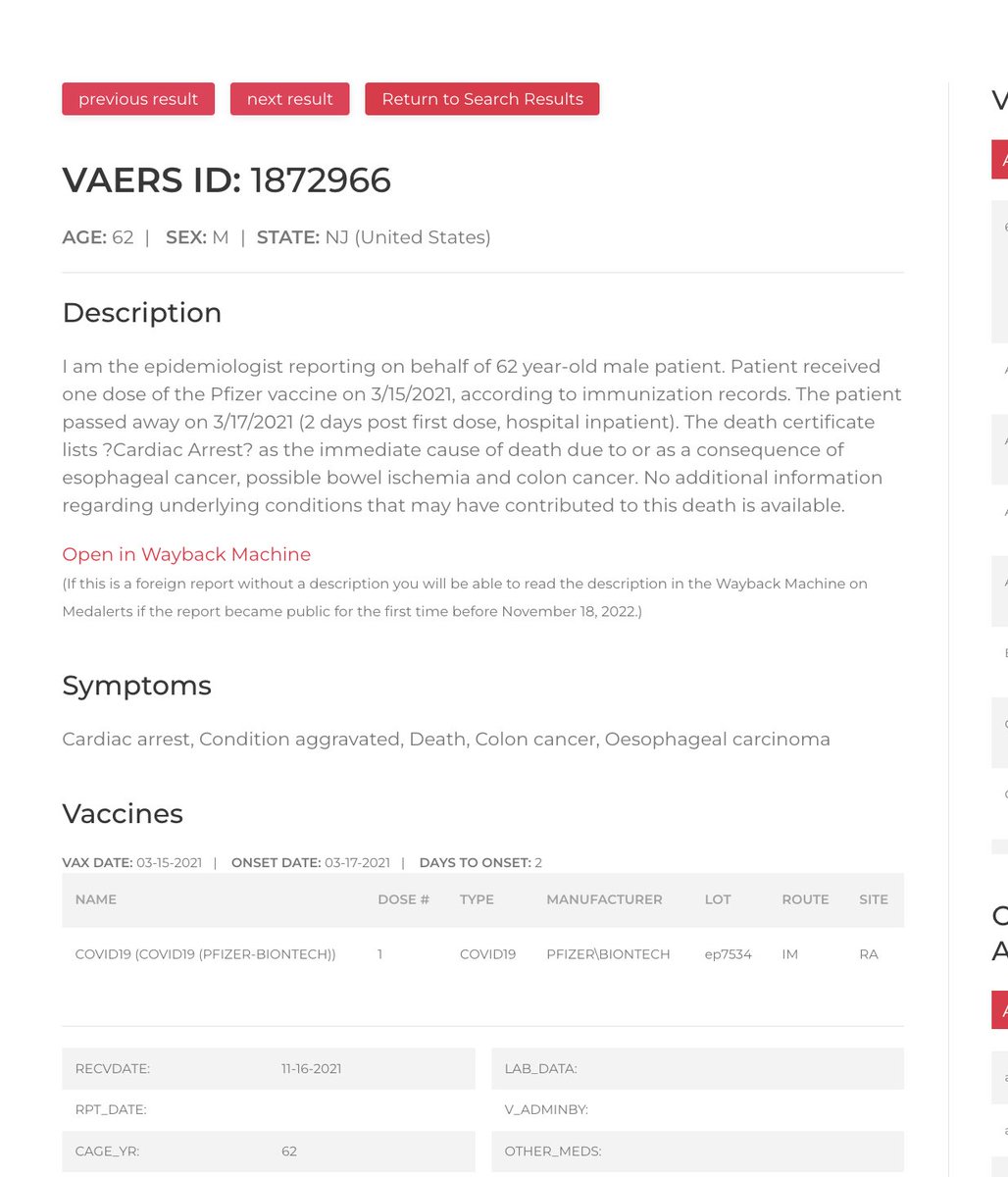

(43/57) VAERS ID 2785362: “TURBO CANCER RAPIDLY SPREAD THROUGHOUT HER BODY, EVENTUALLY WINDING UP IN HER SPINE AND BRAIN…TAKING HER LIFE.” (Three doses of Moderna’s COVID injection.)
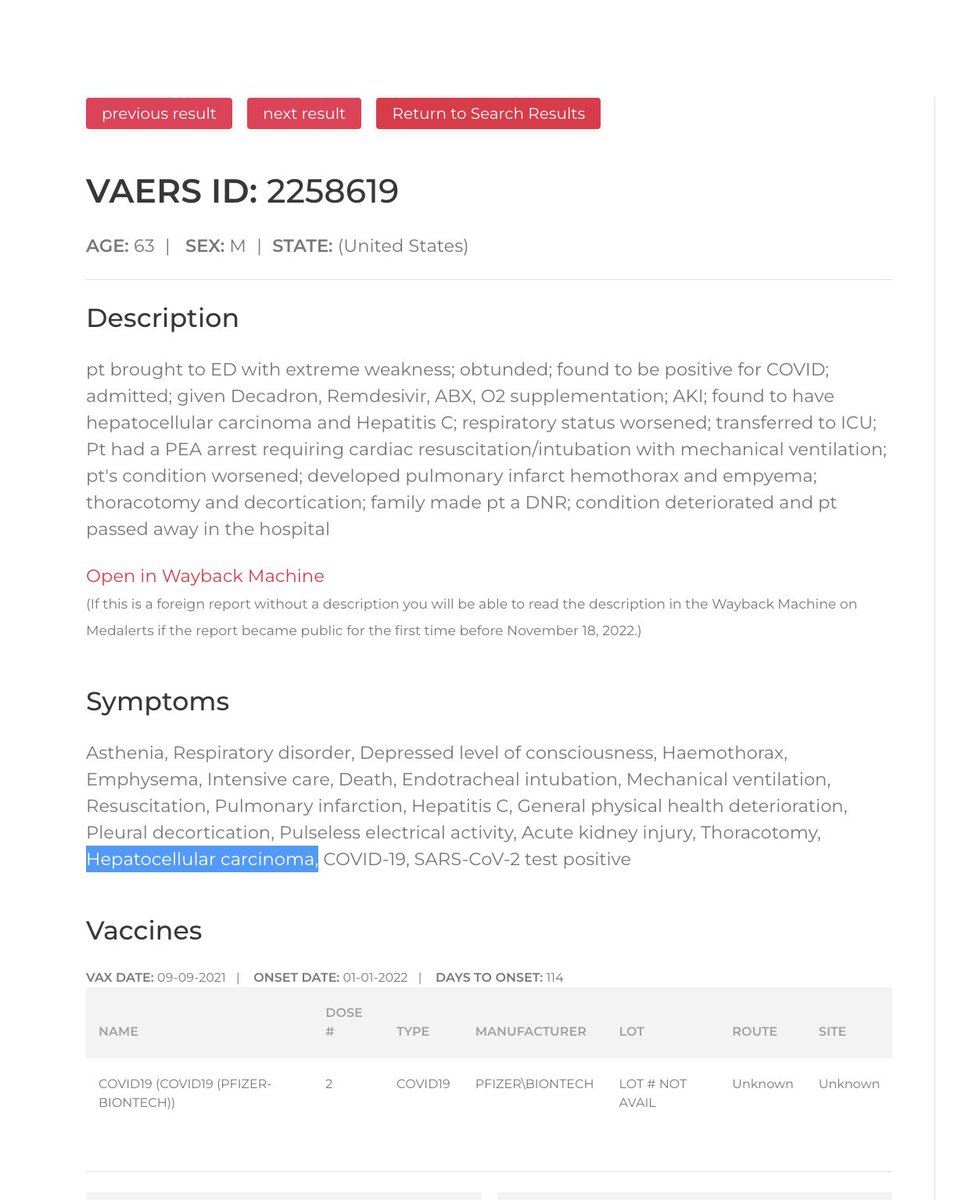

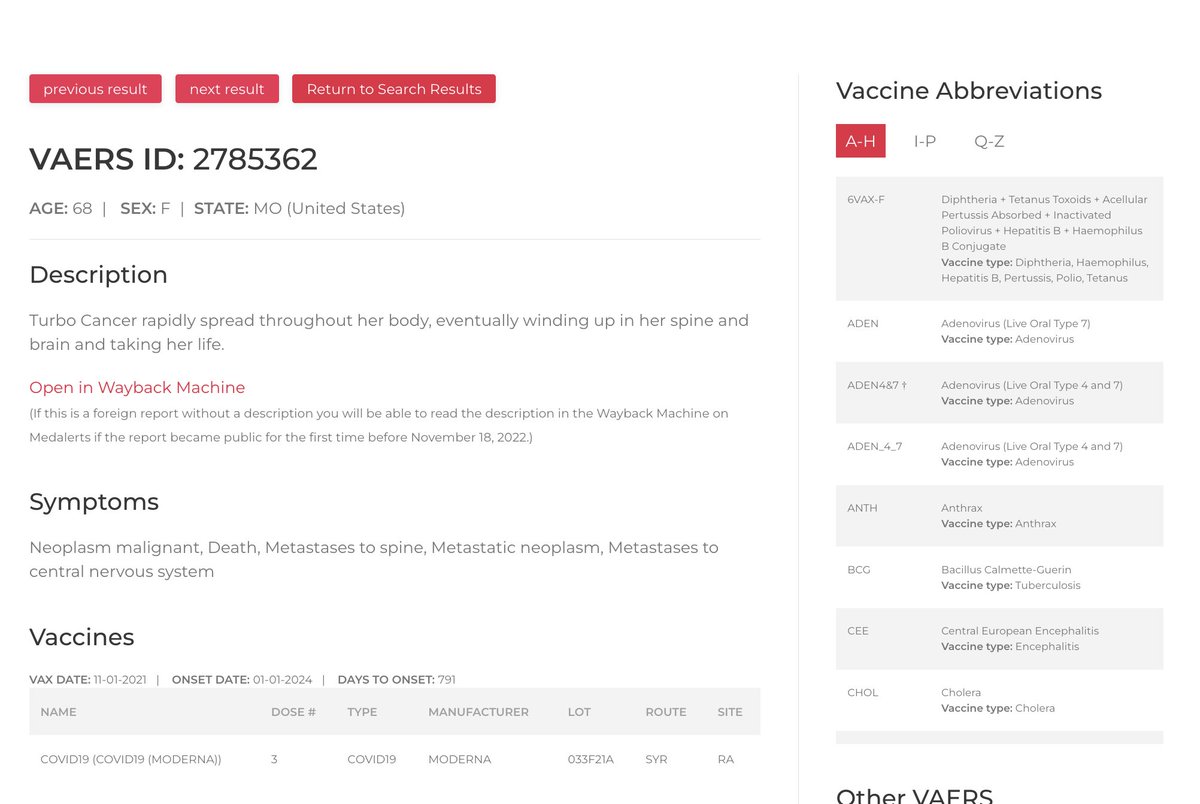

(44/57) VAERS ID 1037833: “SHE [WAS] INFORMED THAT 3 DAYS AFTER THE SHOT, SHE HAD [A] CT WITH CONTRAST FOR STAGE 1 LUNG CANCER.” (One Pfizer COVID injection.)

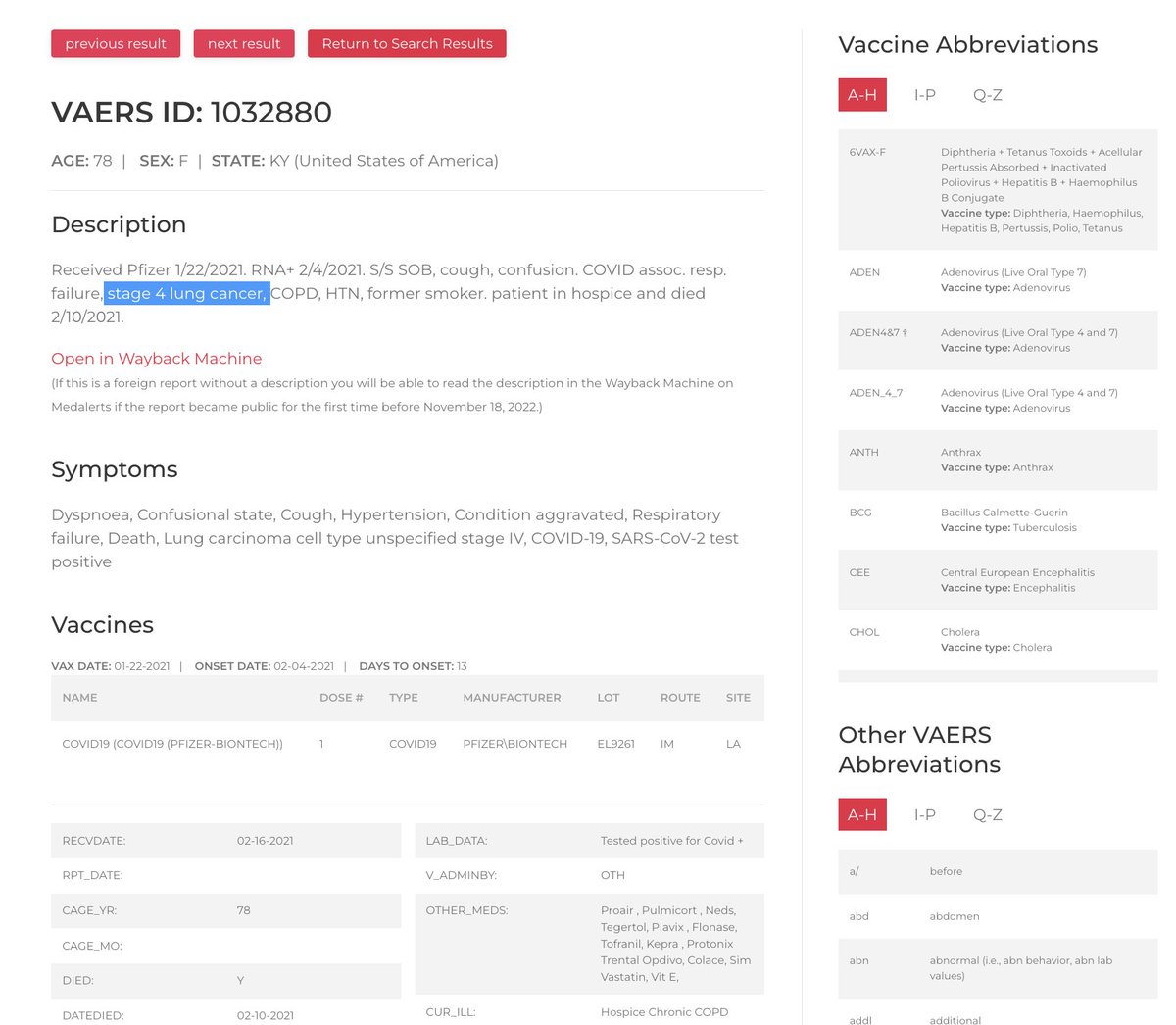


(45/57) VAERS ID 1248298: “PATIENT PRESENTS TO EMERGENCY DEPARTMENT ONE DAY AFTER VACCINATION…FOUND TO HAVE WIDELY METASTATIC...CANCER INVOLVING CHEST, ABDOMEN, AND PELVIS.” (Two Moderna COVID injections.)

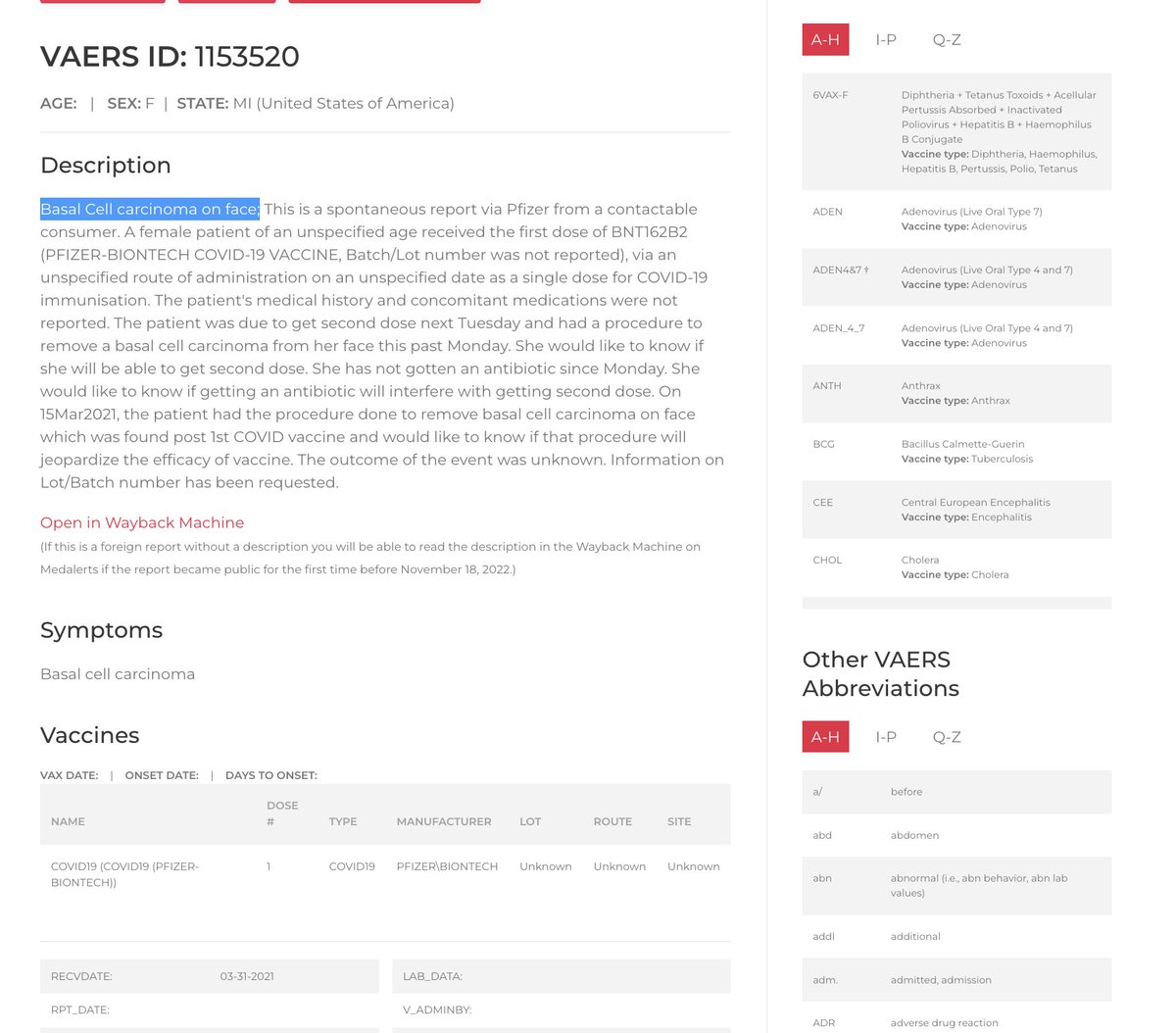
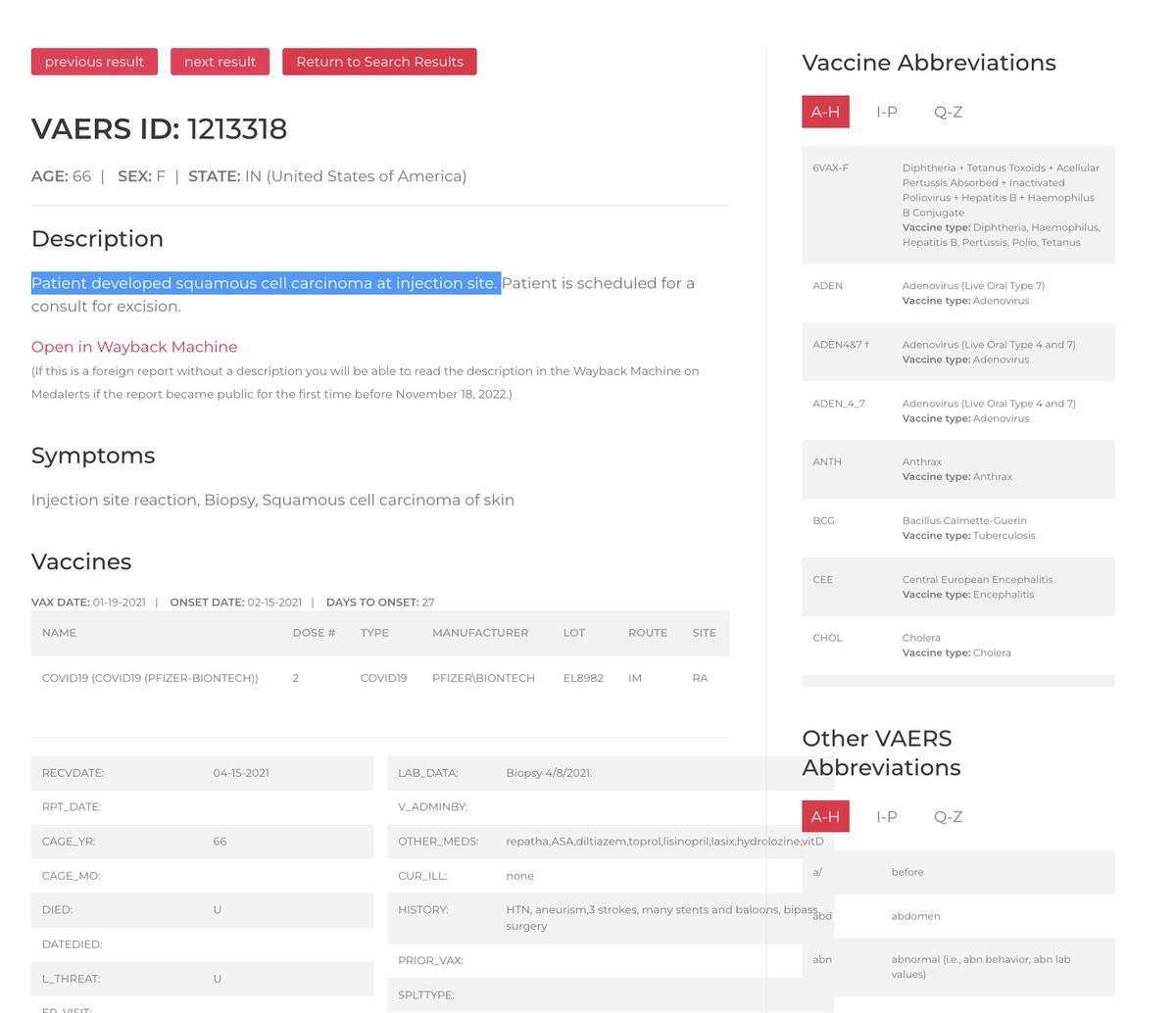

(46/57) VAERS ID 1290185: “PATIENT STATES THAT WITHIN 2 WEEKS OF THE FIRST VACCINE SHE NOTICED BREAST SWELLING, NIPPLE INVERSION AND TENDER AXILA OF THE RIGHT BREAST…[SHE NOW HAS] INVASIVE BREAST CARCINOMA.”
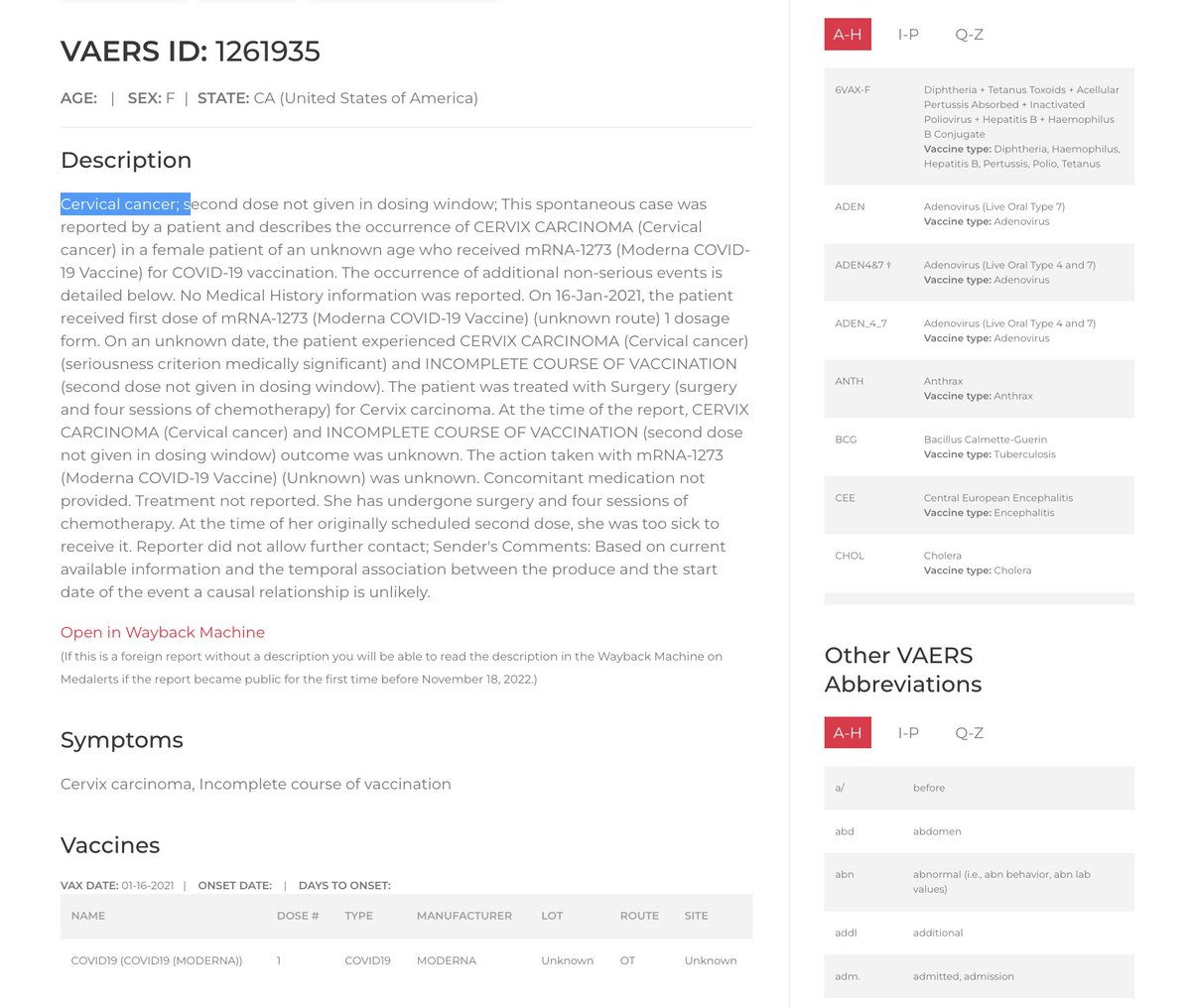
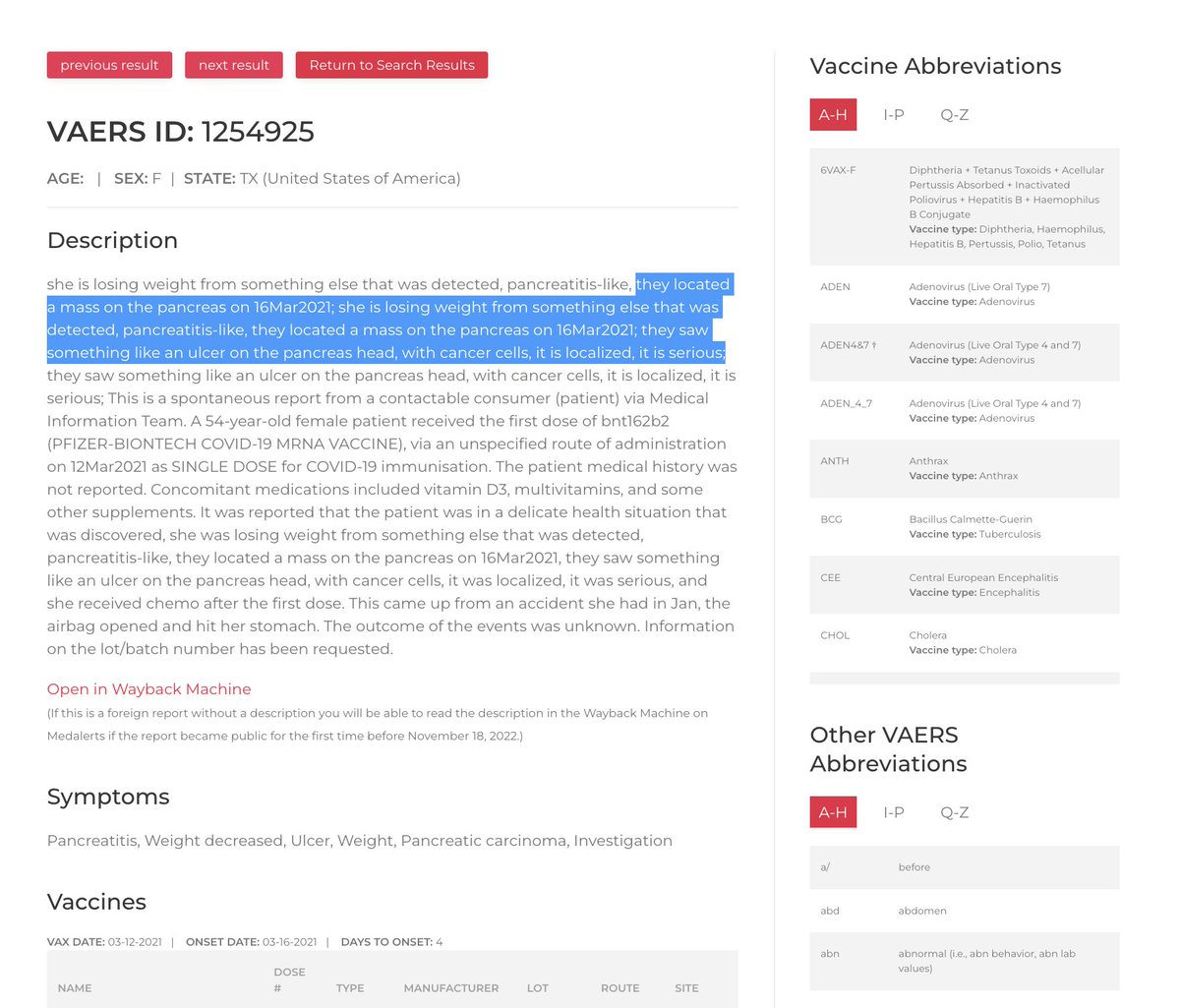
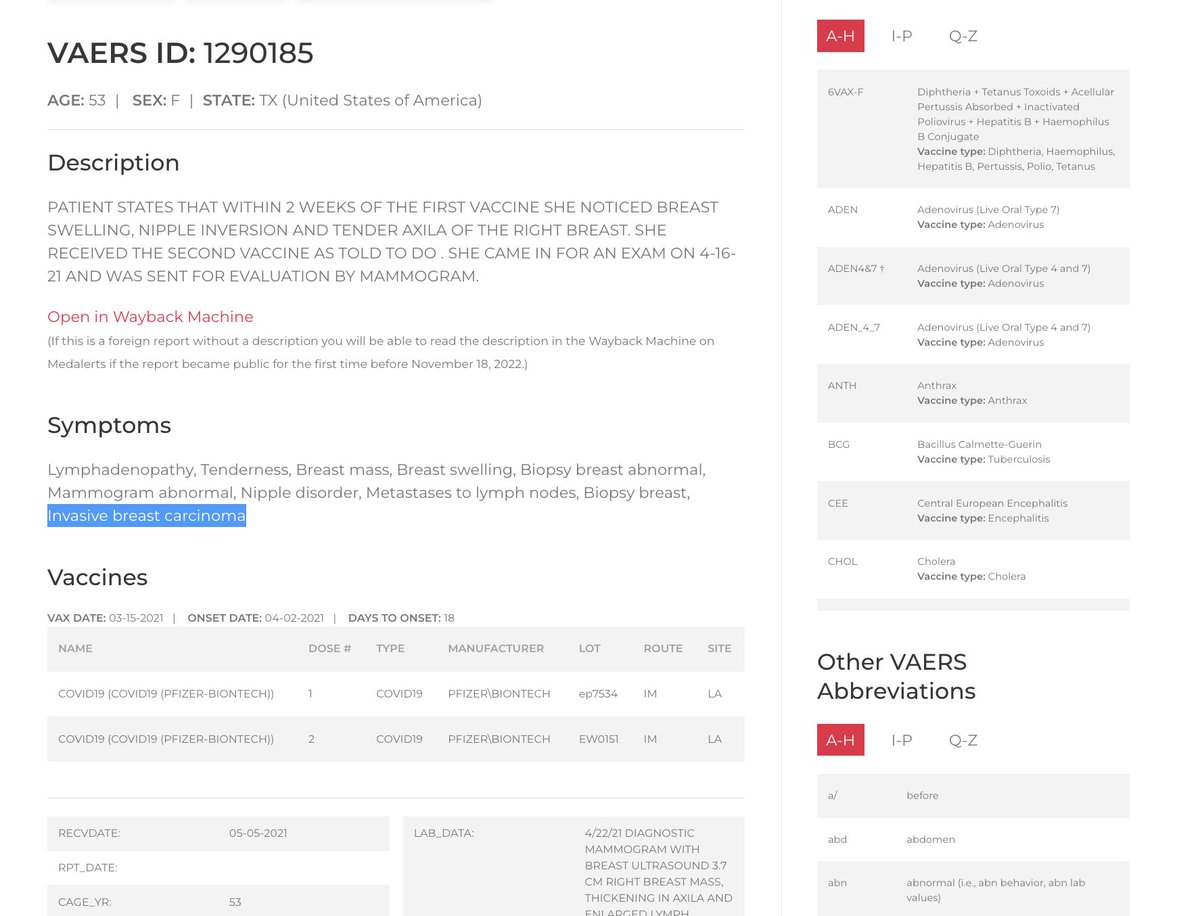

(47/57) SYMPTOMS TEXT SEARCH: CARCINOMA; TOTAL NUMBER OF REPORTS: 923
Note that in the context of the COVID injections, searching a single cancer-related term like “carcinoma” turns up more than 900 reports.
Also note that VAERS reports are only a small fraction of the true number of adverse-event cases. According to one study performed by Harvard Pilgrim Health Care, Inc. in 2011, it is estimated that VAERS is underreported by a factor of 100 or more.
Source: digital.ahrq.gov/sites/default/…
Note that in the context of the COVID injections, searching a single cancer-related term like “carcinoma” turns up more than 900 reports.
Also note that VAERS reports are only a small fraction of the true number of adverse-event cases. According to one study performed by Harvard Pilgrim Health Care, Inc. in 2011, it is estimated that VAERS is underreported by a factor of 100 or more.
Source: digital.ahrq.gov/sites/default/…

(48/57) “I HAVE A FAMILY MEMBER WHO WAS IMMUNO-COMPROMISED, FORCED TO TAKE [THE] VACCINE TO KEEP [THEIR] JOB, [AND] NOW HAS TURBO CANCER & [IS] FIGHTING FOR [THEIR] LIFE.”



(49/57) “MY EX TOOK IT...HE DIED 9 MONTHS LATER WITH TURBO CANCER.”

(50/57) “MY WIFE HAD HER BREAST CANCER IN CHECK BUT WAS MANDATED TO TAKE THE COVID SHOT [WHEN] SHE WAS A SCHOOL TEACHER. TURBO CANCER AND GONE IN 5 WEEKS.”




(51/57) “I LOST MY BELOVED MOTHER TO METASTATIC CANCER (SARCOMA KIDNEYS AND LUNGS) IN AUG [20]23. SHE DECLINED AFTER HER 5TH VACCINE (MODERNA) IN SEPT [20]22.”



(52/57) “MY MUM WAS A HEALTHY, INDEPENDENT, OUT-EVERYDAY WOMAN UNTIL SHE GOT THE SHOT. 2 DAYS LATER SHE HAD BLEEDING BEHIND HER EYES, A FEW MONTHS AFTER THAT, DIAGNOSED WITH LUNG AND BRAIN CANCER…3 DAYS AFTER DIAGNOSIS PASSED AWAY.”
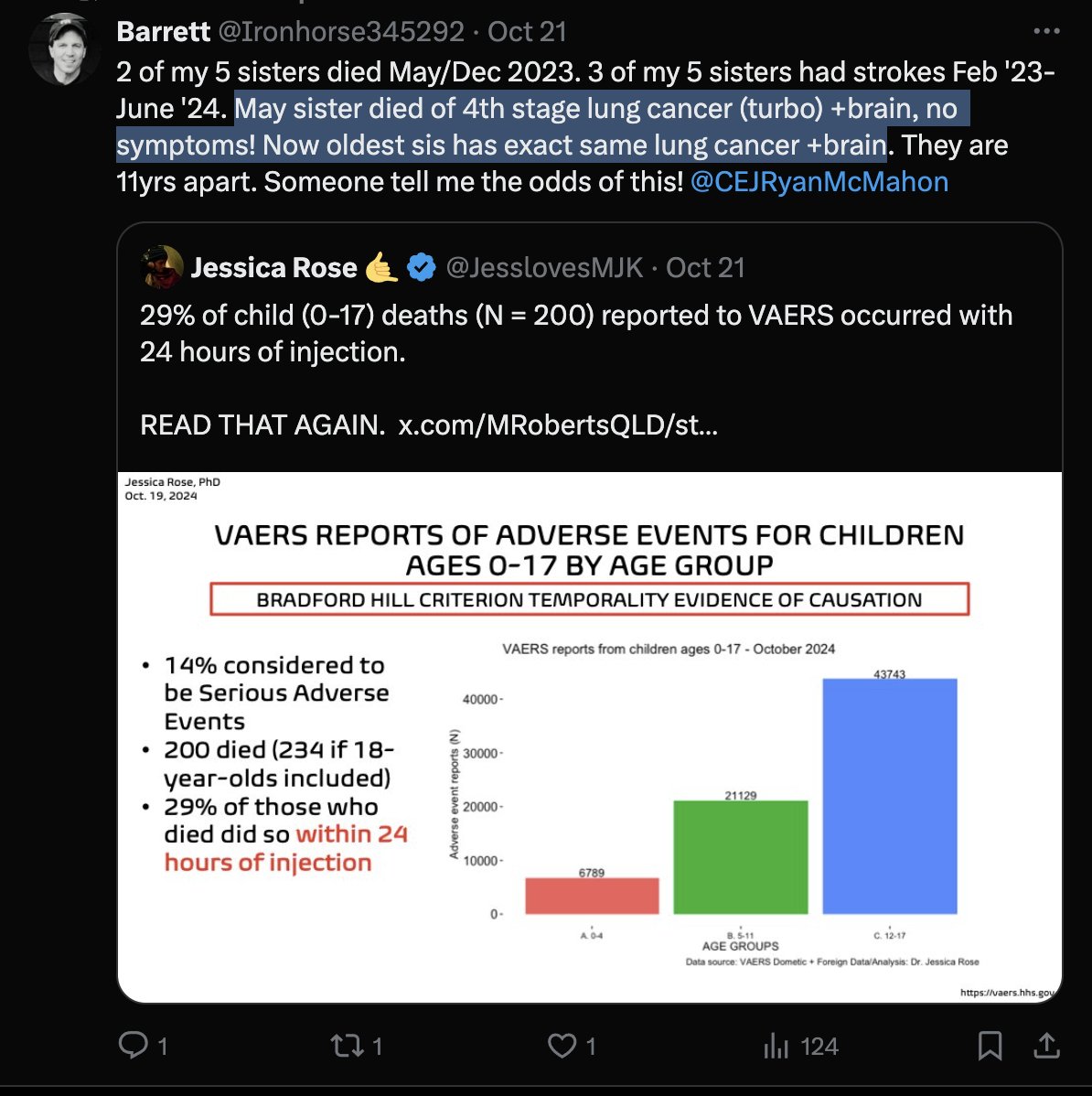


(53/57) “I’VE LOST 5 OF MY FRIENDS (45-55 ALL VAXXED) ALL HAD WHAT I’D DESCRIBE AS TURBO CANCERS THAT SPREAD TOO QUICKLY FOR TREATMENT IN SOME CASES.”




(54/57) “MY [MOTHER IN LAW] WAS DIAGNOSED WITH BRAIN CANCER THIS PAST APRIL, THEY DID OPERATE, BUT 8 [WEEKS] LATER, SHE DIED. SHE WAS [VACCINATED] AT LEAST TWICE THAT WE KNOW OF.”




(55/57) “I HAVE A 47 YEAR OLD FRIEND WHO DIED THIS WEEK. TURBO CANCER. VAX AND BOOSTED. BRAIN TUMORS AND STAGE 4 COLON CANCER IN A MATTER OF MONTHS. DIED A YEAR LATER.”


(56/57) “MY DAD PASSED AWAY IN MAY FROM TURBO CANCER! HE WAS DIAGNOSED IN SEPTEMBER OF 2023, 8 MONTHS LATER HE DIED. HE WAS EXTREMELY HEALTHY, AND IN EXCELLENT SHAPE. HE TOOK 2 SHOTS WITHOUT MY KNOWLEDGE…”




(57/57) “LOST MY FRIEND IN FEBRUARY TO A TURBO CANCER. SHE WENT FROM NO CANCER TO BONE CANCER AND STOMACH CANCER TO DEAD IN SEVERAL MONTHS. HER FAMILY PRESSURED HER TO TAKE THE SHOTS.”




(ADDENDUM TWEET 1) “You know, if you just read the pamphlet that comes with the COVID-19 vaccines, it says COMIRNATY has not been evaluated for…carcinogenicity…[Meaning] It hasn't been tested to see if it causes cancer.”
In this clip, EMT and whistleblower Harry Fisher shows us the package insert that comes with the COMIRNATY injection (i.e. Pfizer’s ostensibly FDA approved COVID injection). He notes that the insert says that the injection has not been tested for potential carcinogenicity. Fisher notes that this means that “it hasn’t been tested to see if it causes cancer.”
“They're constantly telling us it [the COVID injection] can't cause cancer, and they haven't even studied to see if it can,” Fisher adds. “They write it right there in the pamphlet.”
In this clip, EMT and whistleblower Harry Fisher shows us the package insert that comes with the COMIRNATY injection (i.e. Pfizer’s ostensibly FDA approved COVID injection). He notes that the insert says that the injection has not been tested for potential carcinogenicity. Fisher notes that this means that “it hasn’t been tested to see if it causes cancer.”
“They're constantly telling us it [the COVID injection] can't cause cancer, and they haven't even studied to see if it can,” Fisher adds. “They write it right there in the pamphlet.”
(ADDENDUM TWEET 2) PLEASE ADD YOUR OWN PERSONAL TURBO-CANCER STORY TO THIS THREAD.
For me: My first cousin once removed died of turbo cancer at the age of 40 and left behind one young son. Also: my uncle was diagnosed with skin cancer following his injection; my former barber was diagnosed with prostate cancer following his injection; my best friend’s father was diagnosed with colon cancer following his injection.
For me: My first cousin once removed died of turbo cancer at the age of 40 and left behind one young son. Also: my uncle was diagnosed with skin cancer following his injection; my former barber was diagnosed with prostate cancer following his injection; my best friend’s father was diagnosed with colon cancer following his injection.
(ADDENDUM TWEET 3) Another victim tells her story of a loved on developing a turbo cancer caused by a COVID injection:
https://x.com/SenseReceptor/status/1878999624670699624
(ADDENDUM TWEET 4) Another study showing a link between the Covid jabs and cancer, out of Italy.
Source: researchgate.net/publication/39…
Source: researchgate.net/publication/39…

(ADDENDUM TWEET 5) Another study showing a link between the Covid jabs and cancer, out of Korea:
Source: biomarkerres.biomedcentral.com/articles/10.11…
Source: biomarkerres.biomedcentral.com/articles/10.11…

(ADDENDUM TWEET 6) A case of metastatic breast carcinoma to the skin expressing SARS-CoV-2 spike protein possibly derived from mRNA vaccine.
Source: jdsjournal.com/article/S0923-…
Source: jdsjournal.com/article/S0923-…

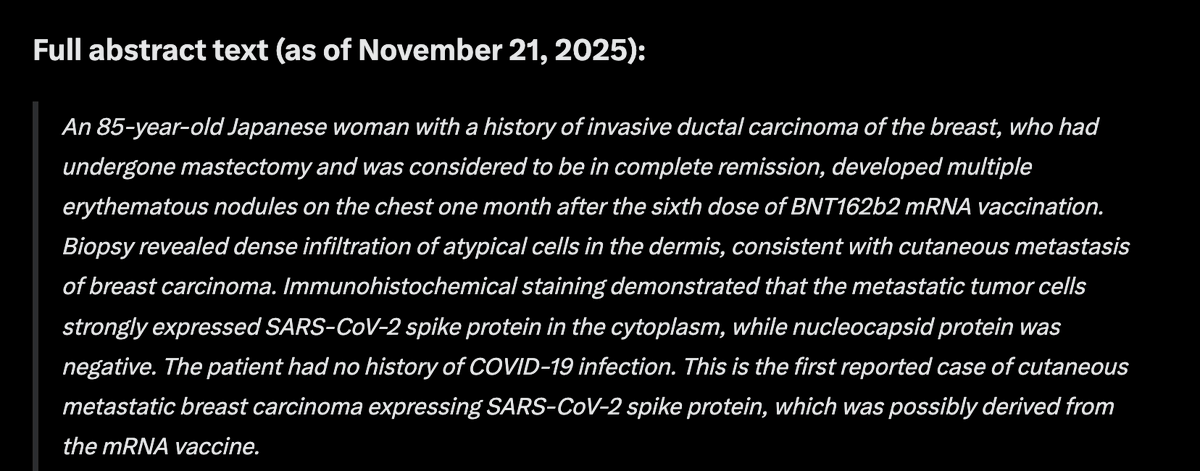
• • •
Missing some Tweet in this thread? You can try to
force a refresh





