I had been baffled for a while by this weird and inaccurate obsession with droplet transmission in healthcare.
How could some people in healthcare be so obstinately obsessed with *droplet* transmission while ignoring *aerosol* transmission.
And how could they be so fixated on denying aerosol transmission when we knew a hundred years ago that mitigation against airborne disease worked.
So I started doing some reading, and then I had a profound realisation, so I'd like to take you on a whistlestop tour of the last 150 or so years.
We start at the time of Florence Nightingale in the 1850s.
She had no idea how the science of it worked, but she knew that people in unventilated rooms were more likely to get ill with respiratory illness...
So she opened the windows.
So she opened the windows.
She could see with her own eyes that windows closed meant increased risk of infection and windows open meant decreased risk.
There wasn't a modern nuanced understanding of 'aerosol particles', but the point was that the *practical mitigation worked*.
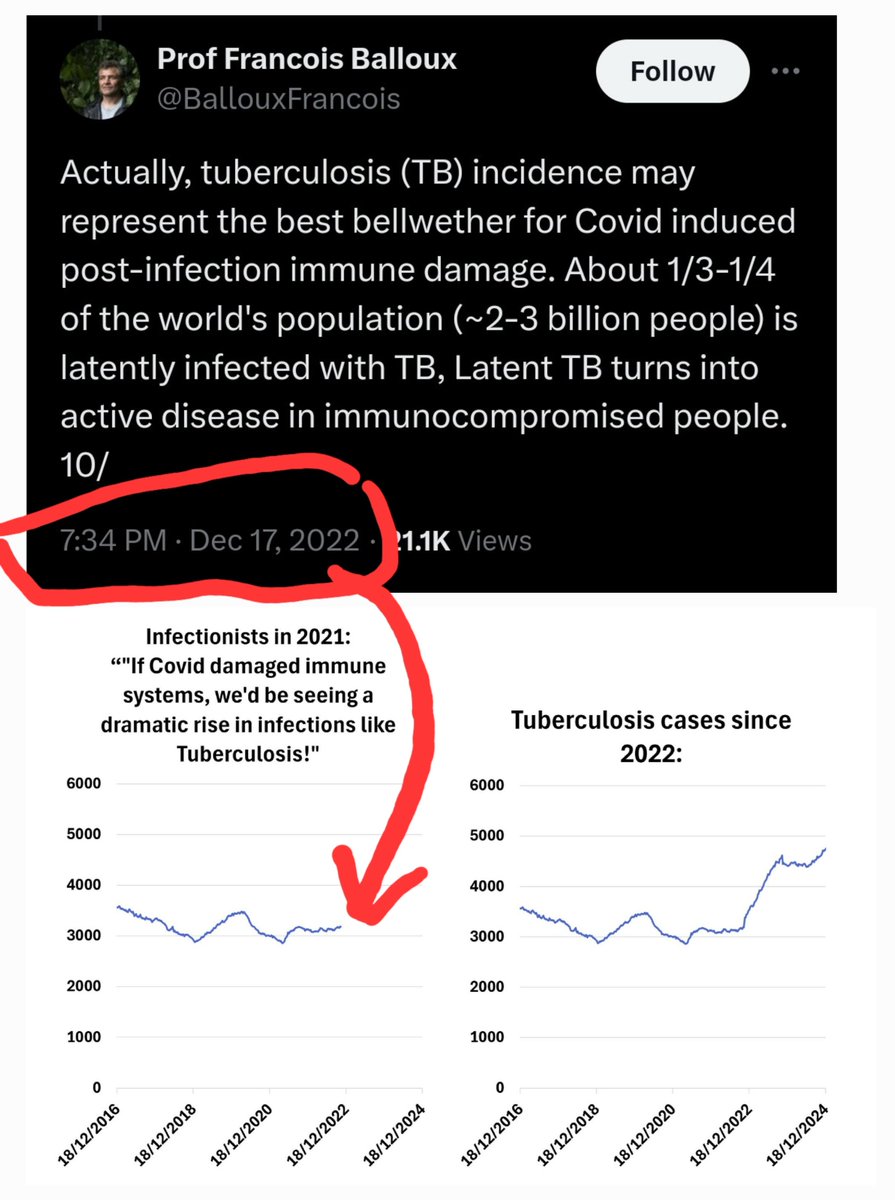
It especially helped with certain diseases like Flu and TB.
So... if they could understand this, what went wrong?
Hold that thought.
Meanwhile two dudes called Semmelweis and Lister were elsewhere concentrating on another type of transmission of pathogens... contact.
Meanwhile two dudes called Semmelweis and Lister were elsewhere concentrating on another type of transmission of pathogens... contact.
Pathogens on our skin, on surfaces... and the introduction of an idea that was astonishing to doctors:
That their bodies were sources of infection.
That their bodies were sources of infection.
They introduced a revolutionary idea to healthcare:
That washing with soap could remove or kill pathogens that then meant that operations and healthcare treatments would be less likely to cause new infections.
That washing with soap could remove or kill pathogens that then meant that operations and healthcare treatments would be less likely to cause new infections.
You may be thinking that this has nothing to do with aerosol transmission.
Well, maybe doctors aren't able to think about two things at the same time without their heads exploding.
Because despite the brilliant uptake of hand and surface hygiene in healthcare something went wrong.
Healthcare scientists had been studying different diseases and how they transmitted.
Before WW2, scientists had proven, by using clever tubes and chambers that prevented droplet transmission that a sick animal could infect a healthy animal with certain diseases, just by whatever was *floating* on its breath.
You see 'droplets' drop.
Like a blob of spit that you can see arc through the air and fall.
That's a droplet.
Like a blob of spit that you can see arc through the air and fall.
That's a droplet.
But some particles are so tiny that they can take advantage of they way forces apply differently to particles of different size... and they can float:
aerosols
aerosols
Like fog.
Or a cloud.
Or smoke.
Or a cloud.
Or smoke.
These particles can stay in the air for days.
Scientists have tracked smog particles (the same size as viral aerosols) that have stayed in the air for **weeks** without falling to the ground.
So before WW2, scientists knew that diseases could spread on particles that floated.
Airborne particles.
Aerosols.
Airborne particles.
Aerosols.
Again... what went wrong...
One of the most famous of these scientists started to work on how exactly these pathogens were spreading... droplets or aerosols...
Some of these experiments used animals again to try and figure out how the pathogens spread.
But some of the other experiments started to look at the particles themselves.
We're now in the post WW2 stage.
The fifties and sixties.
Pre-many vaccines, but mid-antibiotics.
The fifties and sixties.
Pre-many vaccines, but mid-antibiotics.
And here was this guy looking closely at the droplets and particles people produced.
And using the best techniques of the time to do it.
Looking at the droplets and aerosols themselves and figuring out what was in them.
Looking at the droplets and aerosols themselves and figuring out what was in them.
And looking at them in terms of the things they could detect:
Bacteria.
Bacteria.
At the time, you could have someone cough onto a petri dish, and you could watch the bacteria grow.
But you couldn't have someone cough onto a petri dish and watch viruses grow.
So they did the experiments looking for bacteria.
And what did they find?
That bacteria were mostly in the big droplet particles, but not the aerosol particles...
And what did they find?
That bacteria were mostly in the big droplet particles, but not the aerosol particles...
... at least, things like Scarlet Fever were mostly in the droplets...
*TB* was in the aerosols.
But they kind of put TB to one side... because TB infection is something that doesn't come on instantly.
You could be exposed to TB and not develop active TB.
You could be exposed to TB and not develop active TB for several years later.
And besides, you could treat TB with antibiotics, so it kind of got put aside as something to come back to.
And besides, you could treat TB with antibiotics, so it kind of got put aside as something to come back to.
Those droplets were full of bacteria.
And when you combine this understanding with the now long-established idea of surface and body hygiene, the idea is simple:
As long as you sanitise surfaces and hands, and as long as you intercept those droplets that fly through the air on arcs... you're safe.
And gradually, droplet theory started to dominate.
And the windows gradually shut.
And the ventilation declined.
And the ventilation declined.
And the HEPA filters developed in WW2 were forgotten about.
When they developed the ability to check droplets for flu... they found them!
But it was a lot longer before they checked the aerosols for flu... and that was where there was a big surprise waiting.
In the meanwhile, there was this kind of understanding that most things were spread by droplets.
They took what applied to bacteria that they could detect and applied it to viruses that they couldn't.
And meanwhile vaccines started to become available for a wider and wider range of pathogens... and treatments...
It doesn't matter whether something is droplet or aerosol if you have a reliable vaccine or treatment.
So who cares about transmission?
It's the cures that are the priority, right?
But science continued advancing in the background, and the ability to intercept aerosols developed....
... and the ability to detect viruses developed...
And when someone put those two developments together, they made the astonishing discovery that viruses like flu (or Covid) are spread in a different way to bacteria like S Pyogenes that was used in those bacterial droplet studies in the fifties.
*Droplets* are produced mainly in the *throat and mouth and upper airway*... not the lungs.
*Aerosols* are produced mainly in the *deep lungs*.
And Bacteria like S Pyogenes reproduce mainly in the *upper airway*.
And viruses replicate in a way that allows transmission mainly in the *deep lungs*.
So droplets... mainly contain bacteria... from the upper airway...
And aerosols... mainly contain viruses... from the lower lungs.
The habitat in the upper and lower airways is different... different cell types... with different defence mechanisms... and different chemistry...
Flu and Covid... and TB... they get produced *down deep*.
And when they checked the amount of the viruses in aerosols and droplets and compared them...
*There was more virus in the aerosols than the droplets*.
But hospitals since the 80s had been set up to deal with droplet spread, not aerosols.
And even worse than that, healthcare professionals had had droplet theory drilled into them.
And the healthcare professionals that concentrated on infection control... they had to go along with all of that droplet theory or break.
And infection control became more and more and more saturated with people who had been educated in droplet theory and obsessed with droplet theory.
With people who were stuck in outdated science.
With people who were misled by a simple fork in the path in the 50s when it was easier to detect bacteria than viruses.
With people who were following science that was not yet developed enough to understand that aerosols and droplets are produced in different parts of the body.
With people who did not know that the science they followed was limited by a lack of understanding of where different pathogens liked to reproduce.
And then you get into an even more complicated problem... because the people who *implement* infection control aren't the people who are curious.
They're managers.
They're people who are settling into the mundane tasks of checklists and box ticking to ensure that everything is done according to the rules.
They're people who are settling into the mundane tasks of checklists and box ticking to ensure that everything is done according to the rules.
Semmelweiss, Wells, Lister, Nightingale... they were ground breakers... innovators.... researchers... revolutionaries.
People who choose a career in management aren't revolutionaries.
And so the science develops and grows and changes... but the managers remain the same.
And they get tired and older and more stuck in their ways and less able to understand change and they get out of their depth in a pandemic and they preach their old doctrine and when they get asked a question about aerosols in an inquiry they freeze.
The scientists?
They're proving incredible stuff about transmission.
Go check out @ukhadds
Some of the science he shares about aerosol transmission is just light years beyond where the managers are.
They're proving incredible stuff about transmission.
Go check out @ukhadds
Some of the science he shares about aerosol transmission is just light years beyond where the managers are.
But meanwhile we're stuck in this strange limbo where people don't understand that aerosol transmission is significant...
... but that we've also regressed to a position where people don't seem to care about any mode of transmission...
... because as the science was ignored about transmission, people realised that they could ignore more science too... any science that made them feel uncomfortable.
They could ignore the science about how there aren't really any vaccines that can fully stop coronaviruses.
They could ignore the science about the risks posed by repeat infection.
They could ignore anything they wanted to, especially if it was scary.
But the problem about reality is that you can ignore it... but it's bigger than you.
And one day it will float by on an indoor air current, and get you.
Unless of course you understand airborne transmission and you're wearing a mask that intercepts aerosols.
Or you've opened the windows wide like Florence Nightingale.
@threadreaderapp can you please work your magic?
• • •
Missing some Tweet in this thread? You can try to
force a refresh