Events unfolding in Australia re PAs and workforce substitution.
Brace yourself for a tumble down the rabbit hole! 🧵
Brace yourself for a tumble down the rabbit hole! 🧵
https://twitter.com/UQHealth/status/1895247750712766475
Last year, @qldhealth laid the groundwork for the expansion of PAs in Queensland.
Frameworks were put in place that would allow PAs to prescribe + order ionising radiation despite NOT being recognised by the super-regulator APHRA.
2/health.qld.gov.au/__data/assets/…
Frameworks were put in place that would allow PAs to prescribe + order ionising radiation despite NOT being recognised by the super-regulator APHRA.
2/health.qld.gov.au/__data/assets/…
No PA courses currently in Aus. So where were the new PAs going to come from?
Overseas recruitment? Or were the universities gearing up to roll out new courses??
So the tweet above regarding the reorganisation of Medicine/Health Sciences at UQ piqued my interest.
3/
Overseas recruitment? Or were the universities gearing up to roll out new courses??
So the tweet above regarding the reorganisation of Medicine/Health Sciences at UQ piqued my interest.
3/
The UQ Med School has always been the Jewel in the Crown and the Med Faculty run almost semi-autonomously.
Well, it's all been reorganised. Medicine smoushed together with everyone else vaguely health-related. New super-Dean over the Medical School Dean.
4/
Well, it's all been reorganised. Medicine smoushed together with everyone else vaguely health-related. New super-Dean over the Medical School Dean.
4/
The new Dean has a mission.
To shape future health workforce, tailored to the needs of the community and generating evidence to guide its function.
Sounds great!
Except where have I heard this before? 🤔
Oh that's right. NHSE/HEE introducing PAs and other forms of
5/
To shape future health workforce, tailored to the needs of the community and generating evidence to guide its function.
Sounds great!
Except where have I heard this before? 🤔
Oh that's right. NHSE/HEE introducing PAs and other forms of
5/
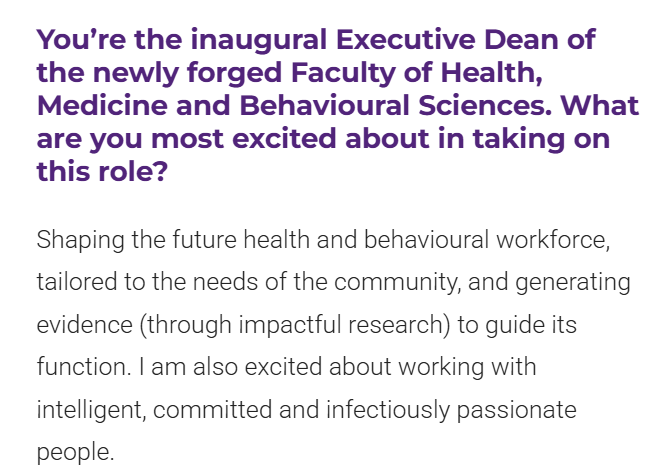
new roles aka workforce substitution.
Virtually WORD FOR WORD.
Further, they actually have a WHOLE department dedicated to this task - the Centre for the Business and Economics of Health. Devoted to reshaping workforce.
6/
Virtually WORD FOR WORD.
Further, they actually have a WHOLE department dedicated to this task - the Centre for the Business and Economics of Health. Devoted to reshaping workforce.
6/

A recent output from the CBEH was this travesty of a article, purporting to be an analysis of the evidence for PAs. But really just a puff piece.
No mention of the problems in the UK. The patient deaths.
7/theconversation.com/what-are-physi…
No mention of the problems in the UK. The patient deaths.
7/theconversation.com/what-are-physi…
They went so far as to lift words directly from a piece Martin McKee wrote, but not provide the context NOR the reference. Nice.
8/
8/
It is striking to me that the UQ Med degree is also in the process of being revamped. No indication of into what.
To summarise:
- the Govt puts frameworks in place for the expansion of PAs
- hospitals put business cases together
- the leading Medical School +
9/
To summarise:
- the Govt puts frameworks in place for the expansion of PAs
- hospitals put business cases together
- the leading Medical School +
9/
Health Sciences reorganises, including a new Dean
- purpose of above is to enable workforce reconfiguration' and 'innovation'
- paid advertising promoting the 'evidence' to back the plan (when there is none).
10/
- purpose of above is to enable workforce reconfiguration' and 'innovation'
- paid advertising promoting the 'evidence' to back the plan (when there is none).
10/
I feel like my tinfoil hat is showing!
But we have seen this all before. Straight out of the NHSE/HEE playbook.
I predict PA and other 'new role' courses announced by the end of this year, with intake next year.
The UK was a practice run. Brace yourself Australia!
But we have seen this all before. Straight out of the NHSE/HEE playbook.
I predict PA and other 'new role' courses announced by the end of this year, with intake next year.
The UK was a practice run. Brace yourself Australia!
@ama_qld @ASMOFnsw @brookmanknight @RACGPPresident @KangarooBeach @rahttled_doc @archiecurium @DrSteveRobson
• • •
Missing some Tweet in this thread? You can try to
force a refresh