
Consultant Acute Physician, The Royal London. Health policy nerd. Former Harveian Librarian, RCP. Antipodean. Views own.

 access medical records.
access medical records.

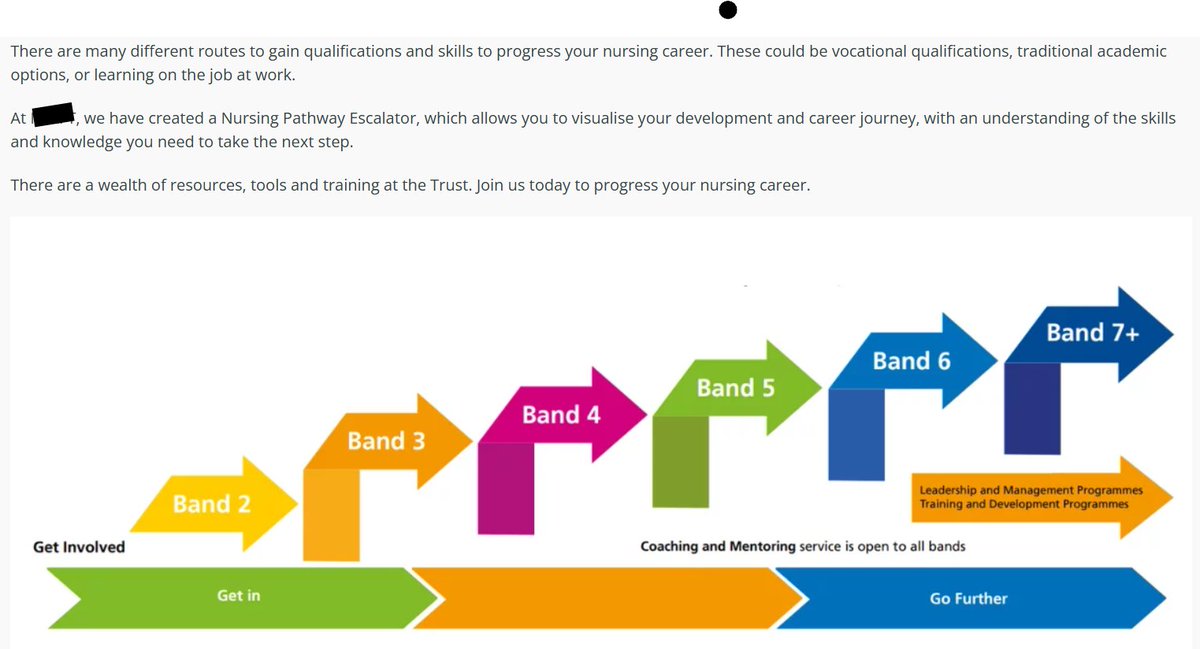 solution to workforce problems and as an engine for 'social mobility'.
solution to workforce problems and as an engine for 'social mobility'.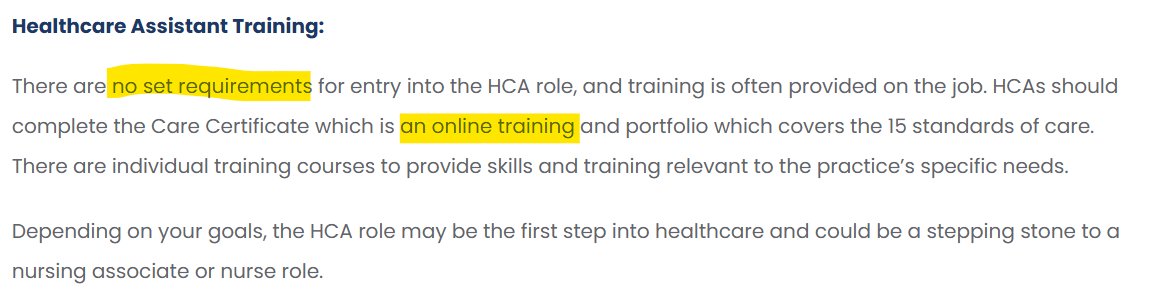
 Outcomes for young people with asthma in the UK are pretty rubbish.
Outcomes for young people with asthma in the UK are pretty rubbish.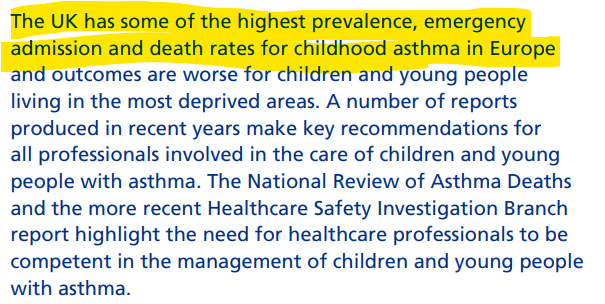
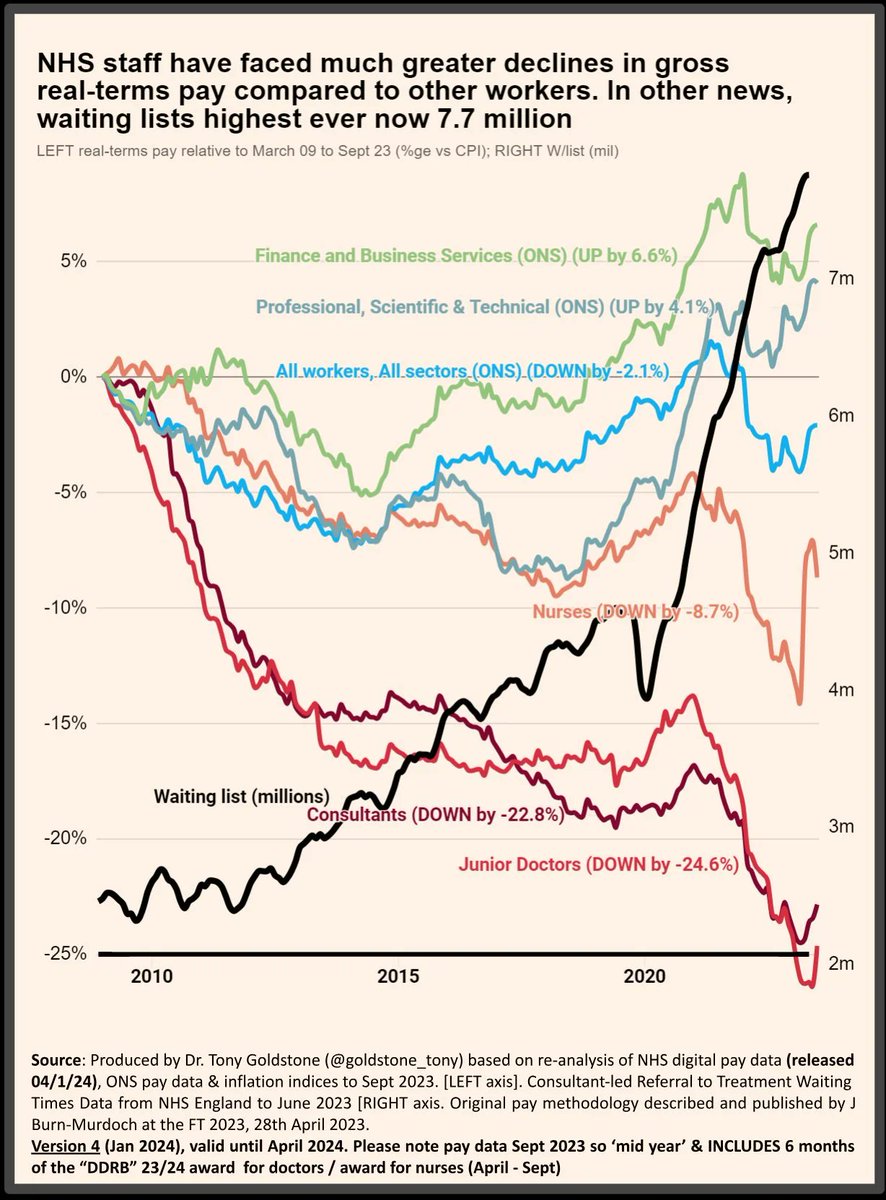
 There is LOTS of good stuff in this. Directly addresses real issues around pay, contracts, careers and bullying.
There is LOTS of good stuff in this. Directly addresses real issues around pay, contracts, careers and bullying.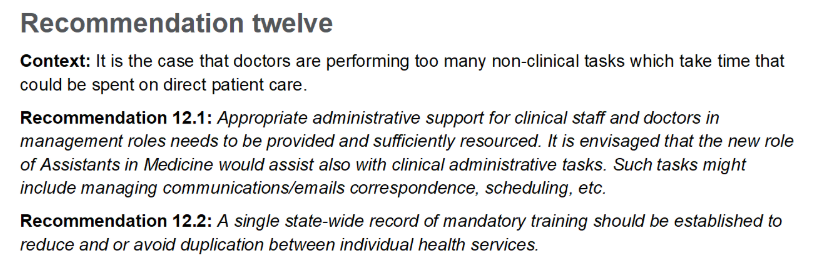

 anywhere in the world. Except perhaps Germany.
anywhere in the world. Except perhaps Germany.
 The problem formulation is eerily familiar.
The problem formulation is eerily familiar.



 Firstly, there are phalanxes of people who DO care about the built environment - architects, engineers, academic, manufacturers, estates people.
Firstly, there are phalanxes of people who DO care about the built environment - architects, engineers, academic, manufacturers, estates people. The Danish Super Hospital programme is ambitious.
The Danish Super Hospital programme is ambitious.
 Things are pretty normal. Hard to tell there has been a pandemic.
Things are pretty normal. Hard to tell there has been a pandemic. 