
Thoughts from yesterday's @KnowlexUK conference
Its not 2020. It is more akin to when harms from, the likes of "passive smoke", "lack of seat belts" & "asbestos" became undeniable - although not visible to all.
There are significant, persistent and undeniable harms.
1/6
Its not 2020. It is more akin to when harms from, the likes of "passive smoke", "lack of seat belts" & "asbestos" became undeniable - although not visible to all.
There are significant, persistent and undeniable harms.
1/6
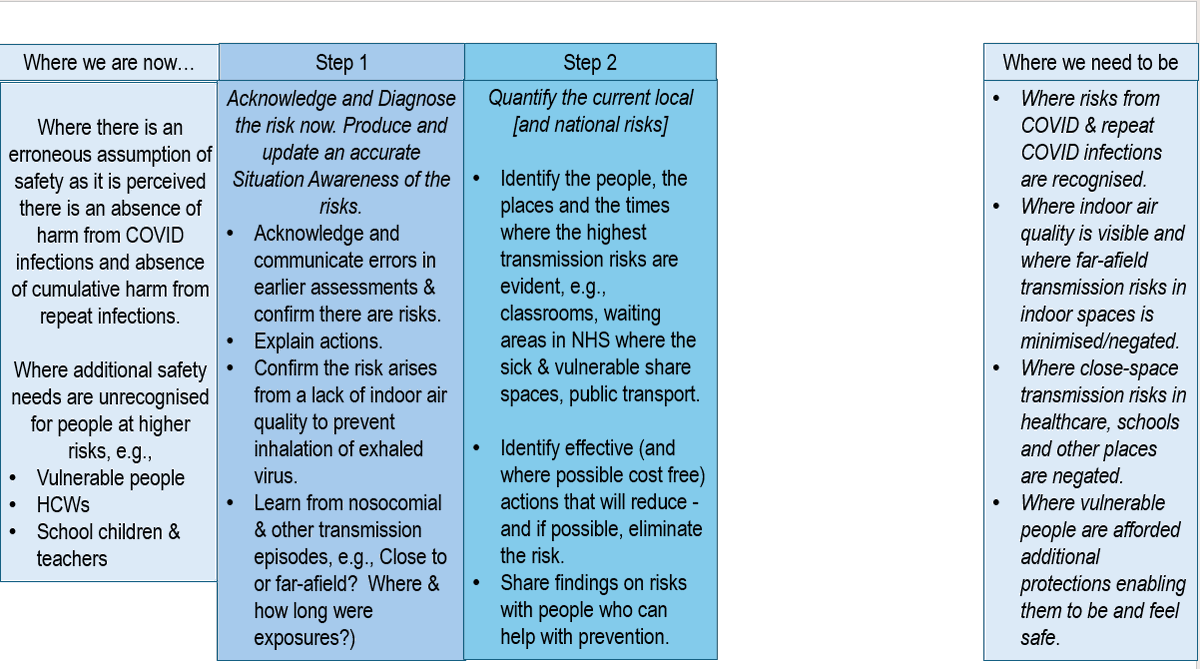
So where are we now, and where do we ?need to be to negate the harms
[starter for 10]
2/6
[starter for 10]
2/6

We will never get to where we need to be in one leap or by 1 action.
What is needed first?
Diagnose the problem and acknowledge the risks
3/6
What is needed first?
Diagnose the problem and acknowledge the risks
3/6

Step 2 - quantify the risk - local and national
4/6
4/6
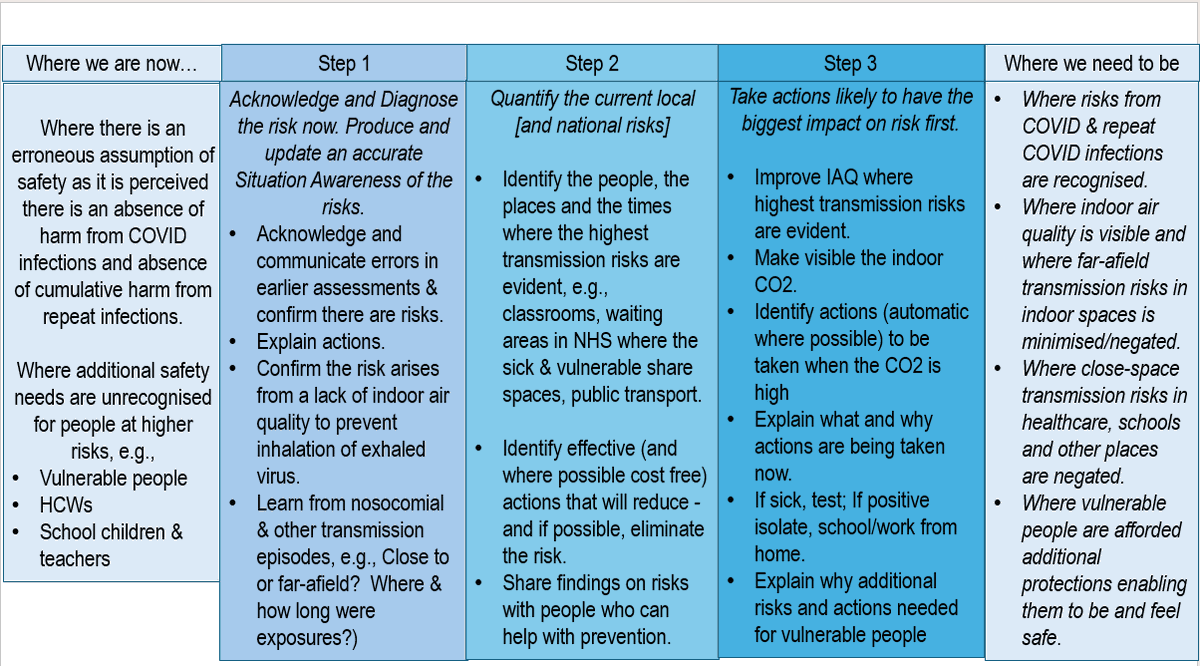
Step 3
Pareto the problem - what will bring the greatest safety leap first?
Get bang for your buck
5/6
Pareto the problem - what will bring the greatest safety leap first?
Get bang for your buck
5/6
Who is in charge of this disease & who is looking at & assessing data risks (apart from @1goodtern )
To whom is a case to be made and how much harm must arise before risks are accepted?
To reduce people needing / demanding healthcare you have to stop them getting sick.
end
To whom is a case to be made and how much harm must arise before risks are accepted?
To reduce people needing / demanding healthcare you have to stop them getting sick.
end
I did a rehearsal for the presentation & recorded it: here it is.
There are a couple of minor errors, it was Guinea pigs and not hamsters for TB.
The audience was mainly IPC people.
Main message - we cant get to where we want to be in 1 step.
There are a couple of minor errors, it was Guinea pigs and not hamsters for TB.
The audience was mainly IPC people.
Main message - we cant get to where we want to be in 1 step.
• • •
Missing some Tweet in this thread? You can try to
force a refresh
















