ALL CHRONIC DISEASES = lack of solar redox during daytime while having too much ALAN/nnEMF at day/night.
Oh so you still think sunglasses, clothing, LED lighting, and sunscreen are good modern human ideas that don't affect the SCN or peripheral clocks in your cells? Consider nature's lessons carefully. What does full spectrum sunlight destroy naturally? UVA and B light naturally lowers adrenalin (the stress hormone of the sympathetic nervous system) while its photons re-zip collagen that cortisol release causes at 4AM that wakes us up by allowing water flows to occur between glial cells and neurons via the aquaporin 4 gates in the brain. AM sunrise light has no UVA or UVB present initially. It has blue, green, and red present. It has more blue than any other part of the spectrum and this is stimulatory to waking us up. Naturally, UVA light shows up later in the AM, depending upon your location in latitude, and this frequency of UVA light acts to begin to re-zip the collagen in our skin and eyes. That initial blue light stimulus from the sun’s rise is used to unwind our collagen to increase water flows to stretch the interspaces in neurons to wake our body and mind up at dawn from sleep. The aquaporin 4 gates are what are destroyed in Multiple sclerosis, which is another autoimmune condition.
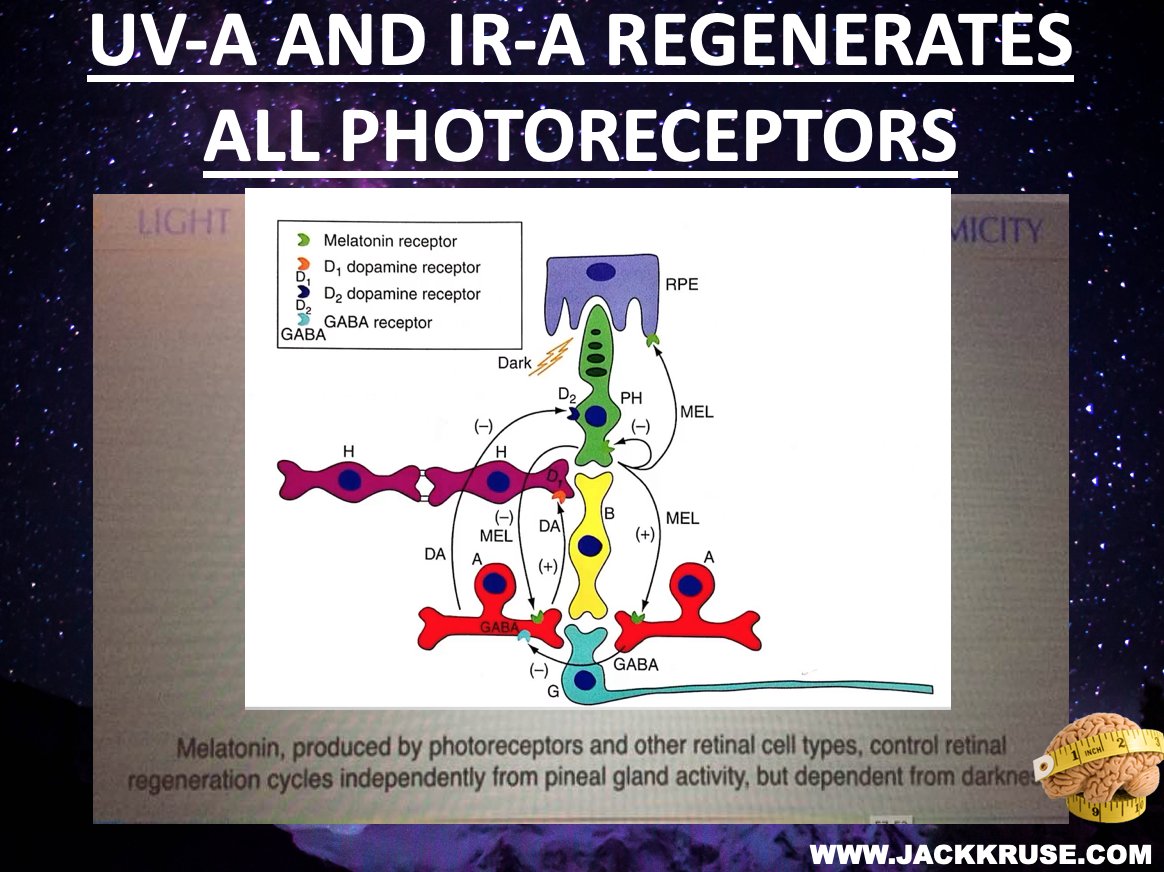
When we are missing UV and/or IR light for any reason, these photoelectric and photochemical are not made. When full spectrum sunlight is absent in someone who is chronically stressed for any reason, sleep cannot be induced by the adenosine chemical signal from the hypocretin neurons because the incident light signal of blue blocks it. What else blocks cellular regeneration by circadian de-coupling? Lack of full spectrum solar exposure is the most common reason and most overlooked issue in all of medicine these days. Proper ocular melatonin cycle requires that these two frequencies (UV/IR) of light be present to stimulate the regeneration processes in the eye during daytime. It also requires ABSENCE of blue 400-465nm at sunset!!!! When these things are off the result always = INFLAMMATION = too many protons and/or not enough electrons at the mitochondrial cellular level. If you think about your childhood, when you spent the day at the park of the beach, you might remember how easy it was to fall asleep and get a sunburn. The reason is simple, sunlight induces sleep because the regeneration pathways that use melanopsin need daylight to regenerate. When you did fall asleep, the redness of your skin did not come from the thermal burn, but it was from the increased blood flow due to the release of nitric oxide that acted to bring the arterioles of the dermis layers to the surface. This is a natural photochemical change induced by sunlight to allow the skin to absorb the UVA and UVB light at the surface. UVA and UVB light does not penetrate deep. To absorb the UV light we need the circulatory system to come from the dermis because UV light does not penetrate skin more than a millimeter. The NO engorges and vasodilates the arterioles containing the RBC’s. The RBC’s are filled with hemoglobin and porphyrins that absorb both UV and IR frequencies. Form meets function photoelectrically. The sunburn is really an absorption of too much thermal IR energy. It is a time phenomena not a sun phenomena based upon your sun callus and skin type. Deep sunburns can result from several factors: excessive sun, or thin skin, thick skin, or a poor adaptation to seasonal light due to chronic use of UV blocking makeup, clothing, or sunblock use in strong light cycles. Today we bury the sunlight and live under alien sun's at night and get diseases caused by inflammation. The sun is not the cause of our problems..........no matter the paradigm's belief or your own.
Sunlight is a gift of Nature.
UVB = Vitamin D
UVB = Sex steroid off-switch
UVB = Melanin production/fecundity/fertility
UVB = β-Endorphins production
UVB = Analgesic
UVB = Leptin Sensitivity via adiponectin/placenta
UVB = Weight-Loss/satiety/appetite regulation
UVB = Anti-Viral/fungal & Anti-Bacterial/mold
UVA = Nitric Oxide = Blood Pressure Regulation
Controls stems depots for Acetyl choline neuron regeneration, weight loss
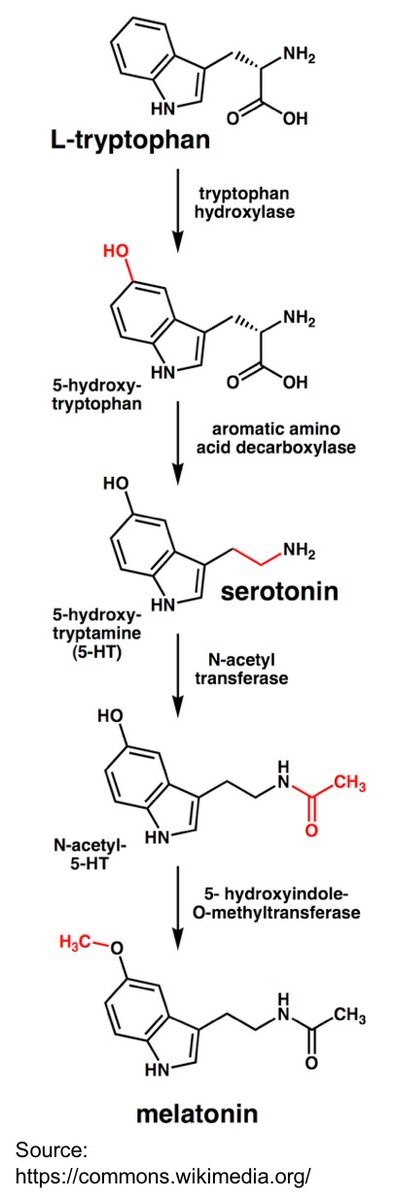
IRA = Melatonin Production
IRA = Photoprevention vs Sunburn
IRA = Builds coherent water domains
IRA = Anti-inflammatory lowers pain
IRA = Builds Collagen/piezoelectric
Red Light = Mitochondrial Function, H20, CO2 NO production
Red Light = Reduces Blood Clotting
Blue Light = Circadian Health (morning)
Blue Light = Stimulates stem cell programming
Blue Light = Adipose Regulation with IR-A and UV
Oh so you still think sunglasses, clothing, LED lighting, and sunscreen are good modern human ideas that don't affect the SCN or peripheral clocks in your cells? Consider nature's lessons carefully. What does full spectrum sunlight destroy naturally? UVA and B light naturally lowers adrenalin (the stress hormone of the sympathetic nervous system) while its photons re-zip collagen that cortisol release causes at 4AM that wakes us up by allowing water flows to occur between glial cells and neurons via the aquaporin 4 gates in the brain. AM sunrise light has no UVA or UVB present initially. It has blue, green, and red present. It has more blue than any other part of the spectrum and this is stimulatory to waking us up. Naturally, UVA light shows up later in the AM, depending upon your location in latitude, and this frequency of UVA light acts to begin to re-zip the collagen in our skin and eyes. That initial blue light stimulus from the sun’s rise is used to unwind our collagen to increase water flows to stretch the interspaces in neurons to wake our body and mind up at dawn from sleep. The aquaporin 4 gates are what are destroyed in Multiple sclerosis, which is another autoimmune condition.
When we are missing UV and/or IR light for any reason, these photoelectric and photochemical are not made. When full spectrum sunlight is absent in someone who is chronically stressed for any reason, sleep cannot be induced by the adenosine chemical signal from the hypocretin neurons because the incident light signal of blue blocks it. What else blocks cellular regeneration by circadian de-coupling? Lack of full spectrum solar exposure is the most common reason and most overlooked issue in all of medicine these days. Proper ocular melatonin cycle requires that these two frequencies (UV/IR) of light be present to stimulate the regeneration processes in the eye during daytime. It also requires ABSENCE of blue 400-465nm at sunset!!!! When these things are off the result always = INFLAMMATION = too many protons and/or not enough electrons at the mitochondrial cellular level. If you think about your childhood, when you spent the day at the park of the beach, you might remember how easy it was to fall asleep and get a sunburn. The reason is simple, sunlight induces sleep because the regeneration pathways that use melanopsin need daylight to regenerate. When you did fall asleep, the redness of your skin did not come from the thermal burn, but it was from the increased blood flow due to the release of nitric oxide that acted to bring the arterioles of the dermis layers to the surface. This is a natural photochemical change induced by sunlight to allow the skin to absorb the UVA and UVB light at the surface. UVA and UVB light does not penetrate deep. To absorb the UV light we need the circulatory system to come from the dermis because UV light does not penetrate skin more than a millimeter. The NO engorges and vasodilates the arterioles containing the RBC’s. The RBC’s are filled with hemoglobin and porphyrins that absorb both UV and IR frequencies. Form meets function photoelectrically. The sunburn is really an absorption of too much thermal IR energy. It is a time phenomena not a sun phenomena based upon your sun callus and skin type. Deep sunburns can result from several factors: excessive sun, or thin skin, thick skin, or a poor adaptation to seasonal light due to chronic use of UV blocking makeup, clothing, or sunblock use in strong light cycles. Today we bury the sunlight and live under alien sun's at night and get diseases caused by inflammation. The sun is not the cause of our problems..........no matter the paradigm's belief or your own.
Sunlight is a gift of Nature.
UVB = Vitamin D
UVB = Sex steroid off-switch
UVB = Melanin production/fecundity/fertility
UVB = β-Endorphins production
UVB = Analgesic
UVB = Leptin Sensitivity via adiponectin/placenta
UVB = Weight-Loss/satiety/appetite regulation
UVB = Anti-Viral/fungal & Anti-Bacterial/mold
UVA = Nitric Oxide = Blood Pressure Regulation
Controls stems depots for Acetyl choline neuron regeneration, weight loss
IRA = Melatonin Production
IRA = Photoprevention vs Sunburn
IRA = Builds coherent water domains
IRA = Anti-inflammatory lowers pain
IRA = Builds Collagen/piezoelectric
Red Light = Mitochondrial Function, H20, CO2 NO production
Red Light = Reduces Blood Clotting
Blue Light = Circadian Health (morning)
Blue Light = Stimulates stem cell programming
Blue Light = Adipose Regulation with IR-A and UV

2. My thesis is life evolved decentralized systems governed by light, using UPEs, electromagnetic fields, and quantum-level processing is reinforced by the AD-light dysregulation connection. The ipRGC-SCN-habenula pathway, melanin’s photophysical roles, and SCAN’s concentric organization all reflect this principle, supported by the ECS.
Modern light environments, ALAN, LEDs, sunglasses, disrupt this harmony, driving inflammation and diseases like AD, MS, and mental health disorders, but AM sunlight, full-spectrum light, and circadian alignment can restore balance, leveraging light’s primacy to enhance health. This decentralized perspective reveals life’s true essence around light, charge, and resonance, a truth the retina, brain, and mitochondria embody.
CITES
jlb.onlinelibrary.wiley.com/doi/full/10.11…
medicalxpress.com/news/2022-08-i…
Modern light environments, ALAN, LEDs, sunglasses, disrupt this harmony, driving inflammation and diseases like AD, MS, and mental health disorders, but AM sunlight, full-spectrum light, and circadian alignment can restore balance, leveraging light’s primacy to enhance health. This decentralized perspective reveals life’s true essence around light, charge, and resonance, a truth the retina, brain, and mitochondria embody.
CITES
jlb.onlinelibrary.wiley.com/doi/full/10.11…
medicalxpress.com/news/2022-08-i…
3. I reframe the GOE’s as an electrical crisis: life evolved decentralized systems to manage oxygen’s electromagnetic stress, using heme proteins, UPEs, and quantum-level processing, with light as the primary regulator.
The Leptin Rx leverages this ancient wisdom, using sunlight to restore circadian alignment, support the ECS, and mitigate modern stressors like blue light, nnEMF, and ferroptosis, which drive diseases like AD, MS, ALS, and mental health disorders.
This decentralized perspective reveals life’s true essence, light, charge, and resonance, a truth encoded in mitochondria, heme proteins, and the brain since the GOE.
The Leptin Rx leverages this ancient wisdom, using sunlight to restore circadian alignment, support the ECS, and mitigate modern stressors like blue light, nnEMF, and ferroptosis, which drive diseases like AD, MS, ALS, and mental health disorders.
This decentralized perspective reveals life’s true essence, light, charge, and resonance, a truth encoded in mitochondria, heme proteins, and the brain since the GOE.



4. The Cost of Silence and the Toxin of Centralized Medicine: A Call for Common Sense New blog.
Every word we utter carries consequences, but so does every silence we choose. Silence when you know better can speak louder than ignorance shouted from the rooftops. Yet, centralized medicine and its cadre of scientists seem deaf to this truth.
For too long, the American taxpayer has been footing a trillion-dollar bill each year, following advice that yields no return on equity (ROE). Chronic diseases like demyleination are exploding, and the technocracy’s light, sold as progress, has become a toxin, poisoning our health and our future. I give you more answers to the puzzle today.
patreon.com/posts/decentra…
Every word we utter carries consequences, but so does every silence we choose. Silence when you know better can speak louder than ignorance shouted from the rooftops. Yet, centralized medicine and its cadre of scientists seem deaf to this truth.
For too long, the American taxpayer has been footing a trillion-dollar bill each year, following advice that yields no return on equity (ROE). Chronic diseases like demyleination are exploding, and the technocracy’s light, sold as progress, has become a toxin, poisoning our health and our future. I give you more answers to the puzzle today.
patreon.com/posts/decentra…
5. If you have a demyelinating disease like BPD, AD, PD, ALS, Depression, Schizophrenia, MS, and Autism pay attention. A meta analysis of 29 studies found that blue blockers can:
→ Improve sleep quality.
→ Help you fall asleep faster.
→ Reduce insomnia in shift workers, travellers & sleep disorders.
→ Advance your circadian rhythm (sleep earlier, wake more refreshed).
→ Even lower manic symptoms in bipolar disorder because of myelin improvements!
Your eyes contain light sensitive cells that suppress melatonin, especially when exposed to blue light and some green (from phones, screens, lights).
Blue-blocking glasses create “virtual darkness” → triggering melatonin release → telling your body it’s time to wind down.
This prevents hormonal disruption, as blue light at night can raise cortisol, disrupt leptin signalling, and lead to insulin resistance.
In simple terms increased hunger, and weight gain in the long run.
Why they're an easy win:
- One-time purchase.
- Portable, effortless, and fits any lifestyle.
- They're safe if used when your sensing blue light not in solar spectra
Buy glasses that have been tested properly : luciaeyes.com
Put them on after sunset, 2 hours before bed and use in tandem with circadian friendly lighting like candles
You will likely fall asleep faster, sleep deeper, and wake up easier. Meyelination require optimal circadian signaling.
→ Improve sleep quality.
→ Help you fall asleep faster.
→ Reduce insomnia in shift workers, travellers & sleep disorders.
→ Advance your circadian rhythm (sleep earlier, wake more refreshed).
→ Even lower manic symptoms in bipolar disorder because of myelin improvements!
Your eyes contain light sensitive cells that suppress melatonin, especially when exposed to blue light and some green (from phones, screens, lights).
Blue-blocking glasses create “virtual darkness” → triggering melatonin release → telling your body it’s time to wind down.
This prevents hormonal disruption, as blue light at night can raise cortisol, disrupt leptin signalling, and lead to insulin resistance.
In simple terms increased hunger, and weight gain in the long run.
Why they're an easy win:
- One-time purchase.
- Portable, effortless, and fits any lifestyle.
- They're safe if used when your sensing blue light not in solar spectra
Buy glasses that have been tested properly : luciaeyes.com
Put them on after sunset, 2 hours before bed and use in tandem with circadian friendly lighting like candles
You will likely fall asleep faster, sleep deeper, and wake up easier. Meyelination require optimal circadian signaling.

6. Blue Light Toxicity and Systemic Effects:
Chronic blue light exposure disrupts the ipRGC-SCN-habenula pathway, leading to flatlined cortisol cycles, suppressed dopamine and melatonin, and hyperactivation of glucocorticoid receptors (GRs) in the SCN, PHb, and hypothalamus.
This suppresses adrenal cortisol secretion, a hallmark of blue light toxicity in modern humans. Exogenous steroids, when combined with blue light toxicity and low vitamin C, amplify this dysfunction, contributing to steroid-induced psychosis and mental illness.
The literature also shows us nicotine addiction’s link to this pathway, that blue light-toxic individuals show reduced sensitivity to nicotine due to altered ACh receptor dynamics, while blue-blocking glasses may increase nicotine sensitivity by restoring balance.
Chronic blue light exposure disrupts the ipRGC-SCN-habenula pathway, leading to flatlined cortisol cycles, suppressed dopamine and melatonin, and hyperactivation of glucocorticoid receptors (GRs) in the SCN, PHb, and hypothalamus.
This suppresses adrenal cortisol secretion, a hallmark of blue light toxicity in modern humans. Exogenous steroids, when combined with blue light toxicity and low vitamin C, amplify this dysfunction, contributing to steroid-induced psychosis and mental illness.
The literature also shows us nicotine addiction’s link to this pathway, that blue light-toxic individuals show reduced sensitivity to nicotine due to altered ACh receptor dynamics, while blue-blocking glasses may increase nicotine sensitivity by restoring balance.

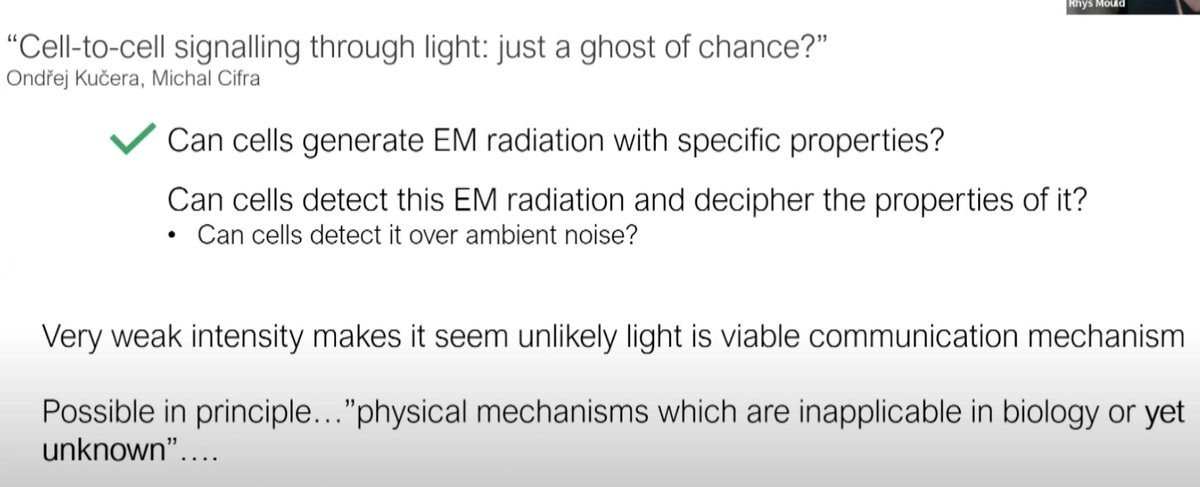
7. ipRGCs, Melanin, and UPEs:
ipRGCs, like the retina’s broader metabolic strategy to use a Warburg metabolism where melanin is absent, are light-sensitive and vulnerable to blue light toxicity. Melanin, present in the retinal pigment epithelium (RPE) and potentially acting as a cryptochrome chromophore (Leask, 1992), amplifies UPE production through its broad-spectrum light absorption and radical generation. Blue light overstimulates melanopsin in ipRGCs and melanin in the RPE, increasing ROS and UPEs (380-450 nm), as predicted for GDF15-related mitochondrial stress. This disrupts dopamine and melatonin synthesis, impairing ipRGC regeneration and circadian signaling to the SCN and habenula. The resulting UPE spike signals mitochondrial stress, elevating GDF15 and contributing to disease, aligning with your thesis’ emphasis on light-driven quantum feedback loops which are recursive.
ipRGCs, like the retina’s broader metabolic strategy to use a Warburg metabolism where melanin is absent, are light-sensitive and vulnerable to blue light toxicity. Melanin, present in the retinal pigment epithelium (RPE) and potentially acting as a cryptochrome chromophore (Leask, 1992), amplifies UPE production through its broad-spectrum light absorption and radical generation. Blue light overstimulates melanopsin in ipRGCs and melanin in the RPE, increasing ROS and UPEs (380-450 nm), as predicted for GDF15-related mitochondrial stress. This disrupts dopamine and melatonin synthesis, impairing ipRGC regeneration and circadian signaling to the SCN and habenula. The resulting UPE spike signals mitochondrial stress, elevating GDF15 and contributing to disease, aligning with your thesis’ emphasis on light-driven quantum feedback loops which are recursive.


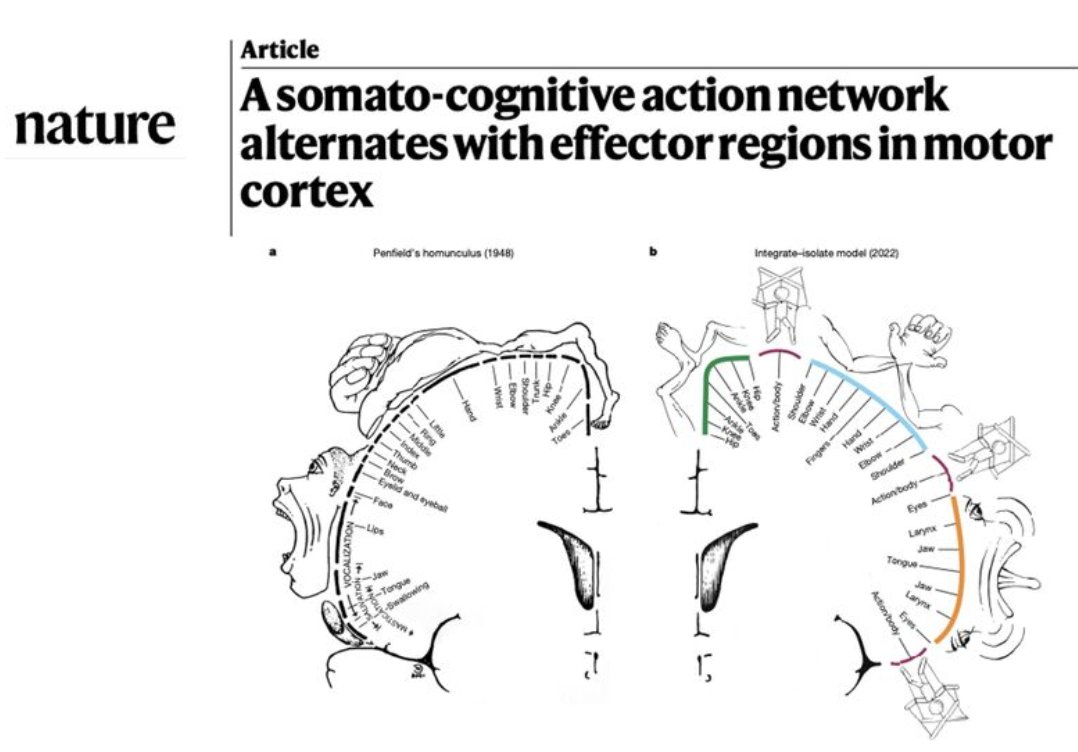
8. Habenula, SCAN, and Neural Circuitry:
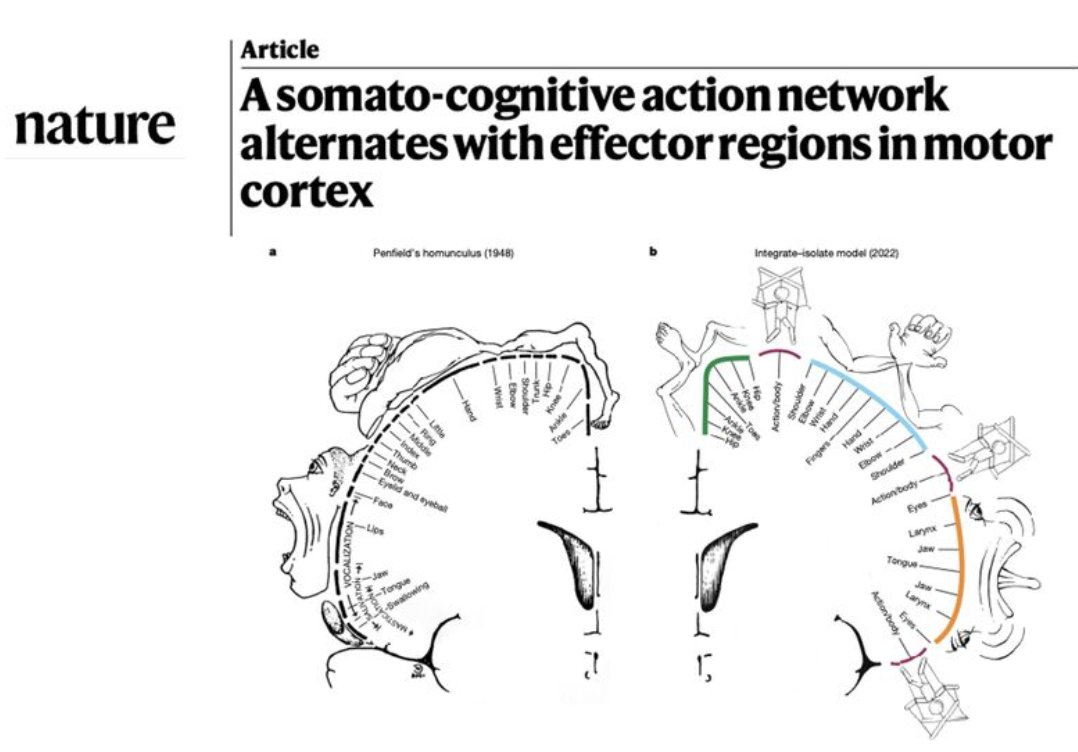
The habenula’s role as a light relay center, connecting the retina to the midbrain and to the frontal lobes, complements SCAN’s concentric organization in the motor cortex. This is a recursive light loop that controls the entire physiology of the human.
Both structures operate in a decentralized, non-hierarchical manner, integrating sensory (light via ipRGCs), cognitive (habenula’s role in mood), and motor signals (SCAN).
Blue light-induced depletion of dopamine and GABA in the habenula disrupts this integration, impairing SCAN’s distributed processing and contributing to mood disorders and neurodegeneration. Melanin’s enhancement of action potentials and proton conductance (via its semiconductor properties) supports neural circuitry in both regions, but blue light and nnEMF disrupt this, slowing conduction and increasing UPEs, as seen in MS and ALS. nnEMF disrupt myelination at some level in all these diseases and this affects the neurologic function distal to the defect by altering UPE spectra.
The habenula’s role as a light relay center, connecting the retina to the midbrain and to the frontal lobes, complements SCAN’s concentric organization in the motor cortex. This is a recursive light loop that controls the entire physiology of the human.
Both structures operate in a decentralized, non-hierarchical manner, integrating sensory (light via ipRGCs), cognitive (habenula’s role in mood), and motor signals (SCAN).
Blue light-induced depletion of dopamine and GABA in the habenula disrupts this integration, impairing SCAN’s distributed processing and contributing to mood disorders and neurodegeneration. Melanin’s enhancement of action potentials and proton conductance (via its semiconductor properties) supports neural circuitry in both regions, but blue light and nnEMF disrupt this, slowing conduction and increasing UPEs, as seen in MS and ALS. nnEMF disrupt myelination at some level in all these diseases and this affects the neurologic function distal to the defect by altering UPE spectra.
9. Tell me, you think food guru or health influencers can get you to this level? If so, let me know so I can block you from my feed.

10. The internalization of melanin from primate to hominid gave us the ability to tap the absorption spectra of and the specialization of aromatic amino acids.
This occured after 600 million years of the conservation of DHA in the CNS of compext life reflect the general rule of evolutionary complexity: expanding endogenous UPEs to process information at a quantum level. The movement of POMC to chromosome 2 in humans optimized this system, enhancing the brain’s ability to generate and respond to UV-range UPEs, driving the emergence of advanced consciousness. This built a recursive photonic loop between the sun and our cells that allowed for CNS complexity to explode in short evolutionary time scales giving silly talking monkey's abilities no one can explain until now. Decentralized Medicine has a path to explain this. bigthink.com/starts-with-a-…
This occured after 600 million years of the conservation of DHA in the CNS of compext life reflect the general rule of evolutionary complexity: expanding endogenous UPEs to process information at a quantum level. The movement of POMC to chromosome 2 in humans optimized this system, enhancing the brain’s ability to generate and respond to UV-range UPEs, driving the emergence of advanced consciousness. This built a recursive photonic loop between the sun and our cells that allowed for CNS complexity to explode in short evolutionary time scales giving silly talking monkey's abilities no one can explain until now. Decentralized Medicine has a path to explain this. bigthink.com/starts-with-a-…
11. @threadreaderapp make me a roll.
• • •
Missing some Tweet in this thread? You can try to
force a refresh