PolyBio Spring Symposium 2025 (@polybioRF)
Thread below 👇
Thread below 👇
29/ Marcelo Freire’s team found SARS-CoV-2 spike protein (green) in colon and ileum biopsies from Long COVID patients but not in healthy controls. This supports gut persistence of viral antigen as a potential driver of chronic symptoms. 
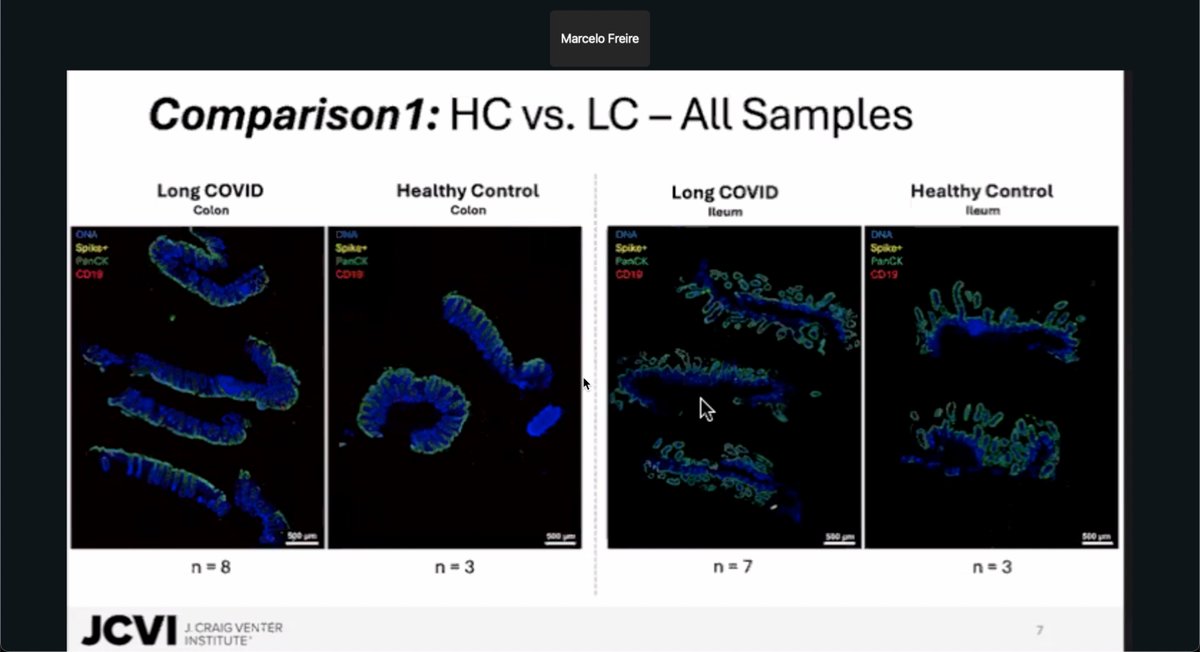
30/ In healthy controls, SARS-CoV-2 spike protein is rarely detected in gut tissue. Region-of-interest (ROI) analysis confirms minimal spike signal and immune activation, reinforcing that spike persistence seen in Long COVID is not a background feature.

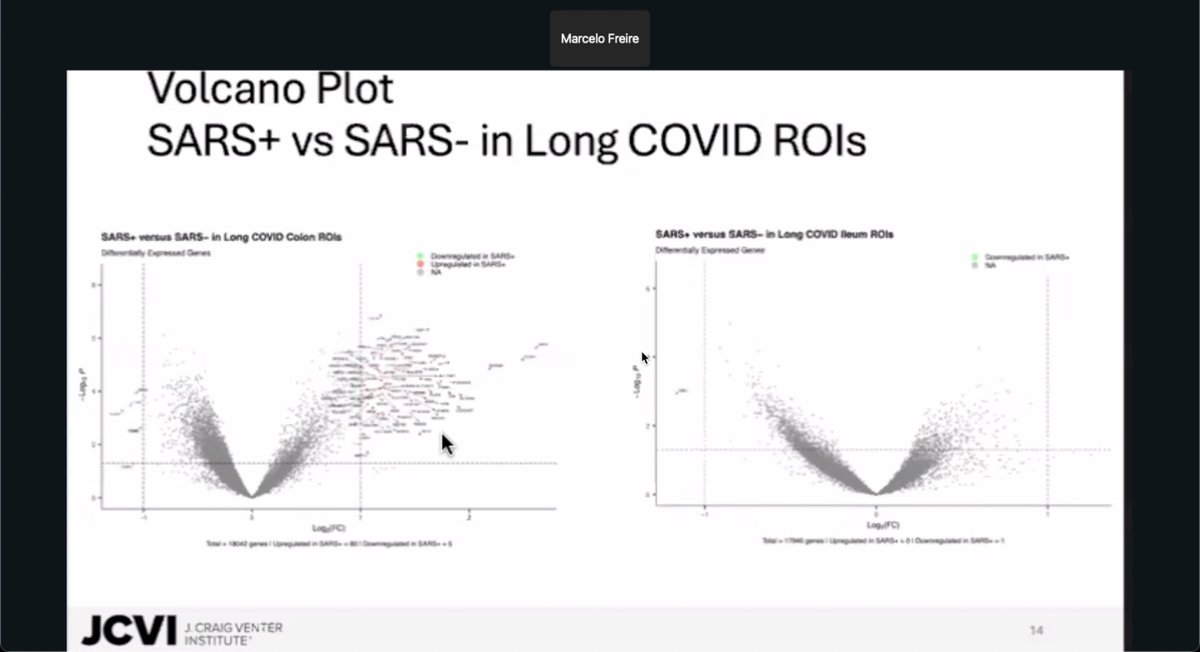
31/ In Long COVID colon samples, regions with detectable SARS-CoV-2 spike protein show clear transcriptional changes, including many upregulated genes. No such differential expression is seen in ileum samples, highlighting tissue-specific immune responses to viral persistence.
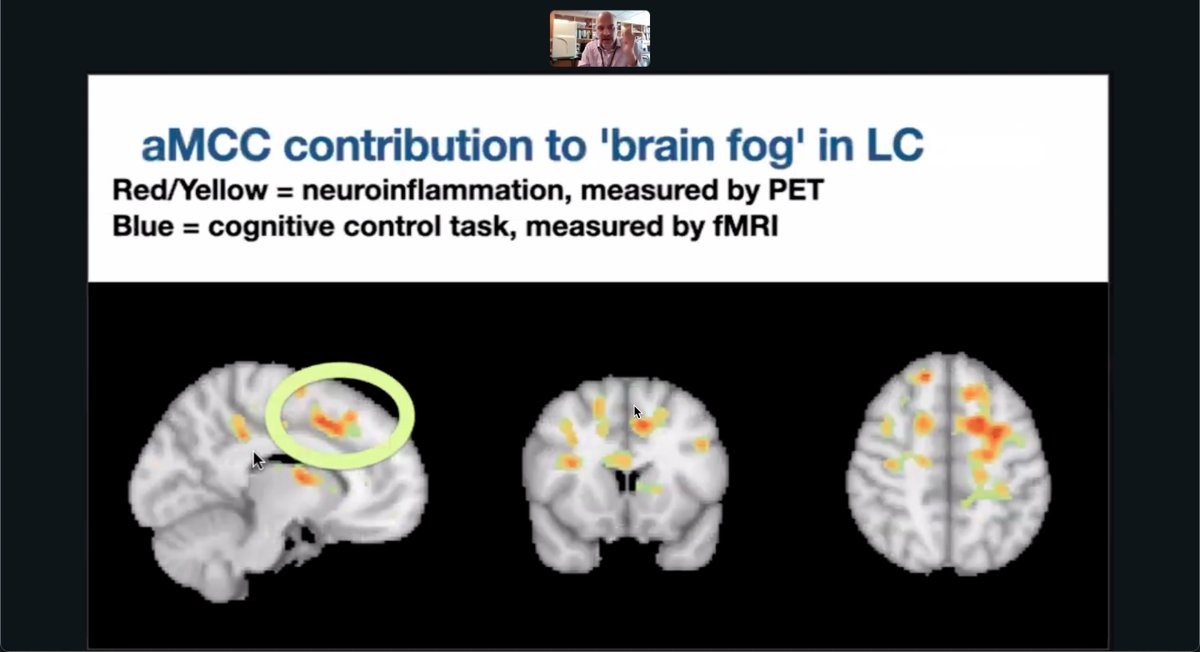
32/ Michael VanElzakker shows that Long COVID patients have elevated neuroinflammation (red/yellow) in the anterior midcingulate cortex (aMCC), a region tied to cognitive control (blue). This overlap may help explain the brain fog reported in persistent COVID.
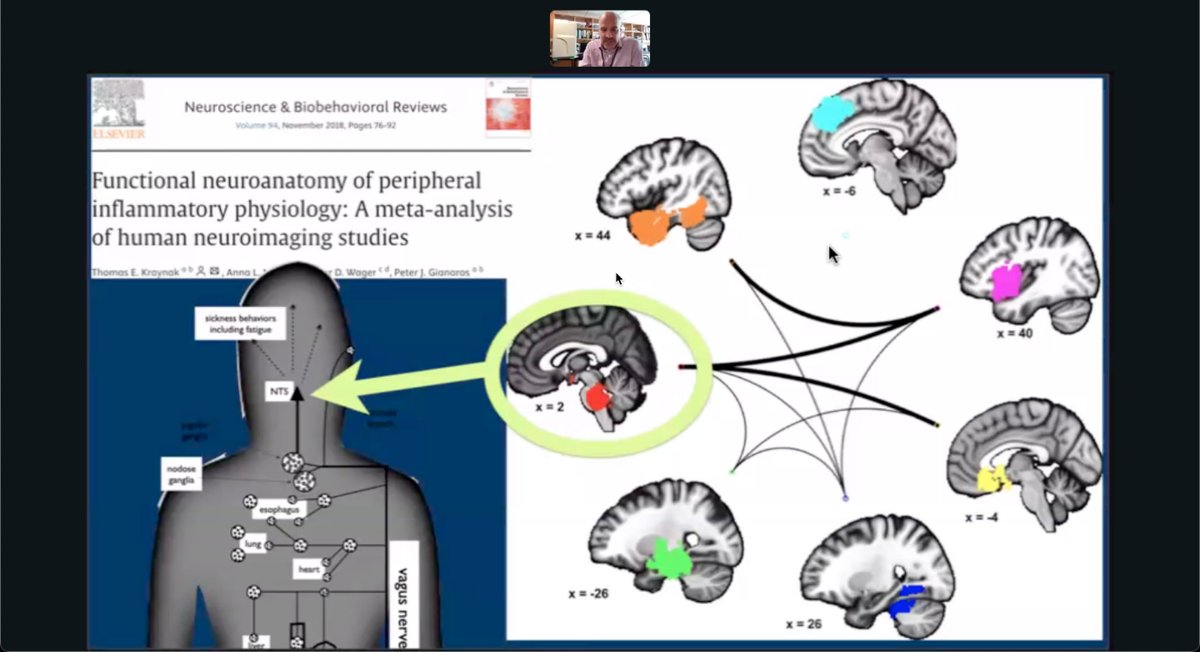
33/ Vagus nerve signaling from peripheral inflammation activates brain regions like the insula, amygdala, and anterior cingulate cortex. These areas coordinate “sickness behaviors” such as fatigue, supporting a brain-body model of Long COVID symptoms.
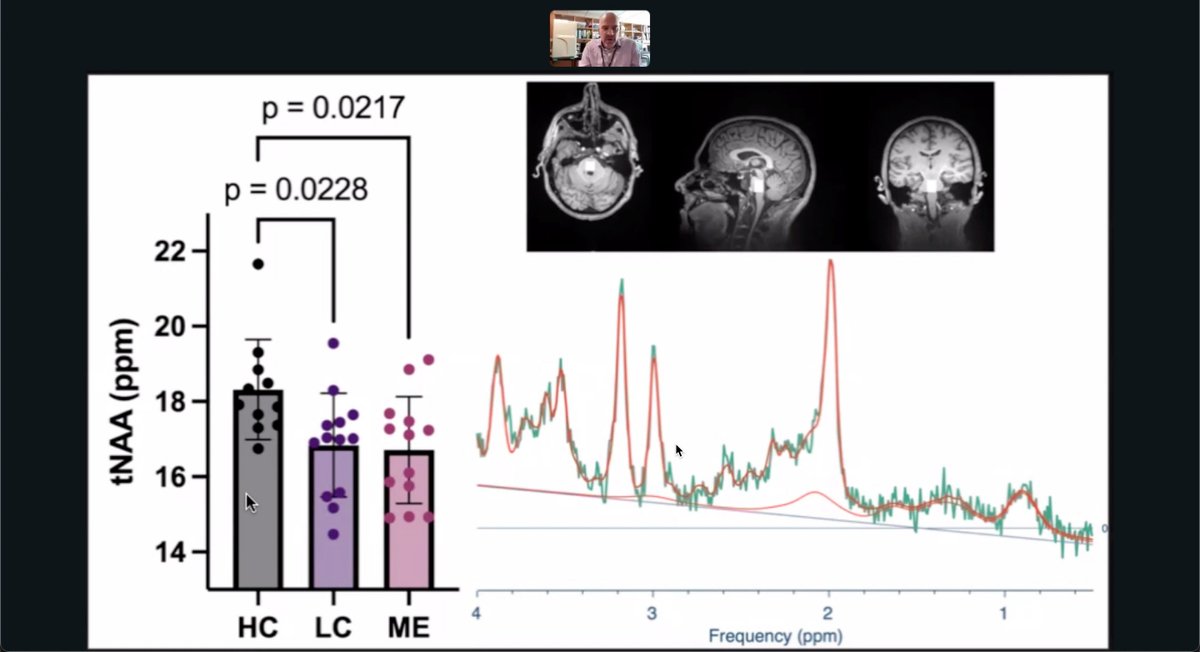
34/ Using brain MR spectroscopy, researchers found reduced total N-acetylaspartate (tNAA)—a marker of neuronal health—in Long COVID and ME/CFS patients compared to healthy controls. This suggests overlapping neurobiological changes in fatigue-related conditions.
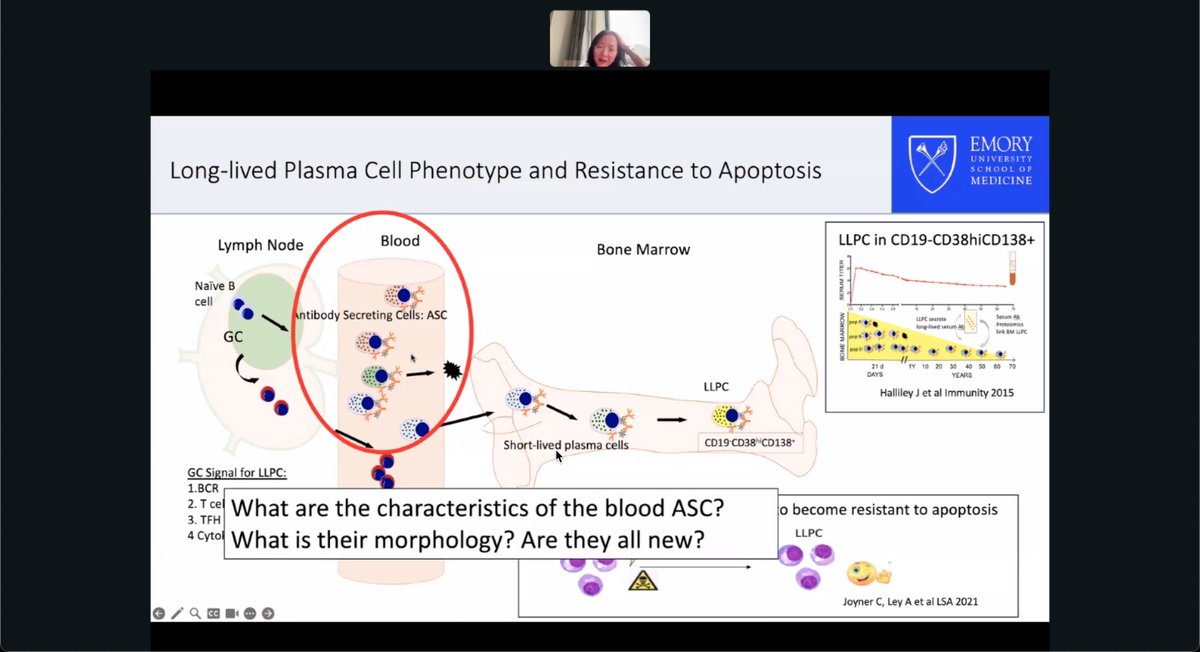
35/ F. Eun-Hyung Lee is investigating antibody-secreting cells (ASCs) in blood during Long COVID. These cells may adopt features of long-lived plasma cells—resisting apoptosis and persisting outside bone marrow—potentially sustaining chronic immune activation.
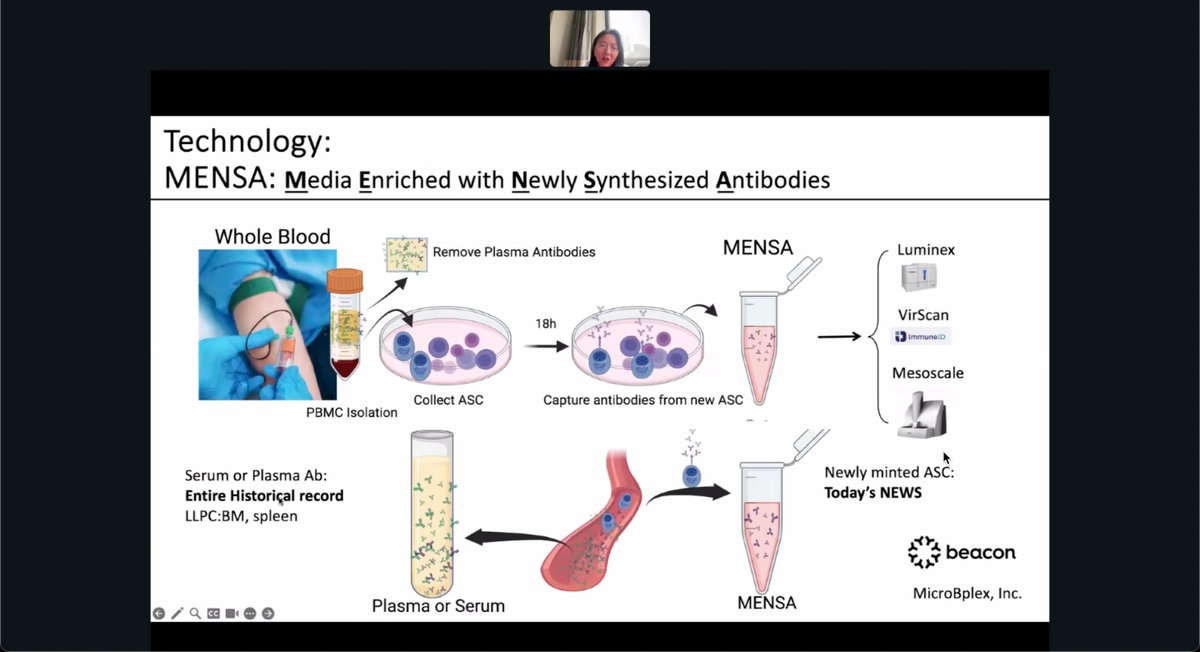
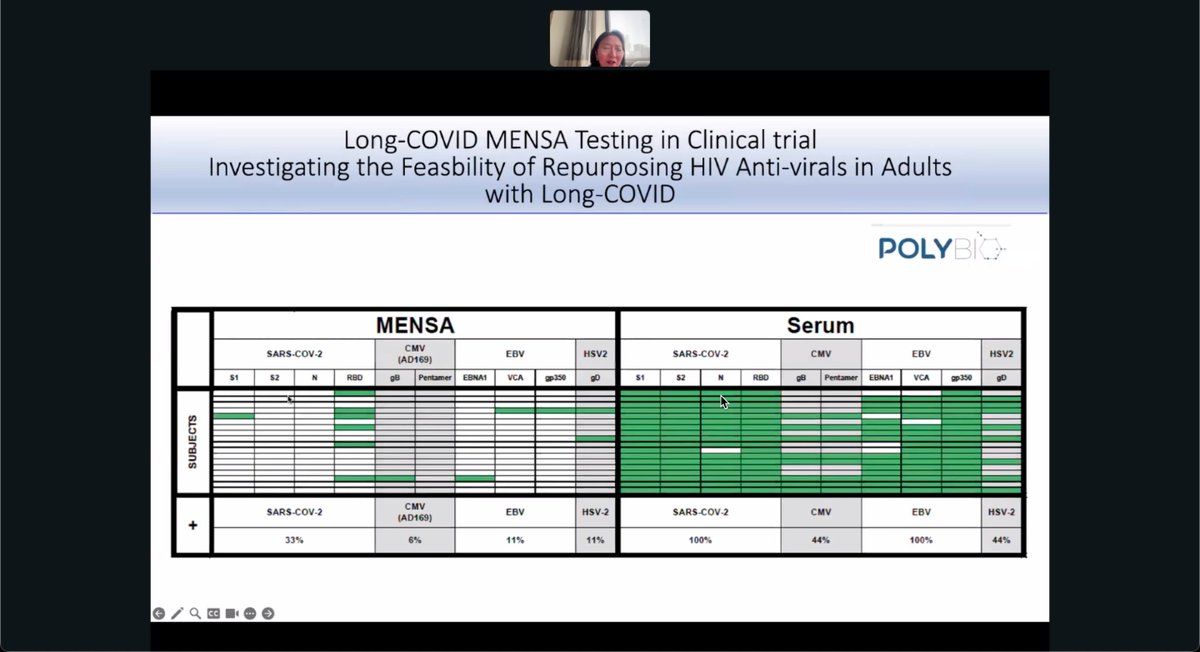
36/ The MENSA assay isolates freshly produced antibodies from circulating antibody-secreting cells (ASCs), offering a real-time snapshot of active immune responses. Unlike serum, which reflects long-term memory, MENSA reveals what the immune system is targeting right now.
37/ Emory researchers show MENSA spikes only after new infection or vaccination, while serum antibodies stay high long after. MENSA detects active antibody production, revealing recent immune activity rather than long-term memory.

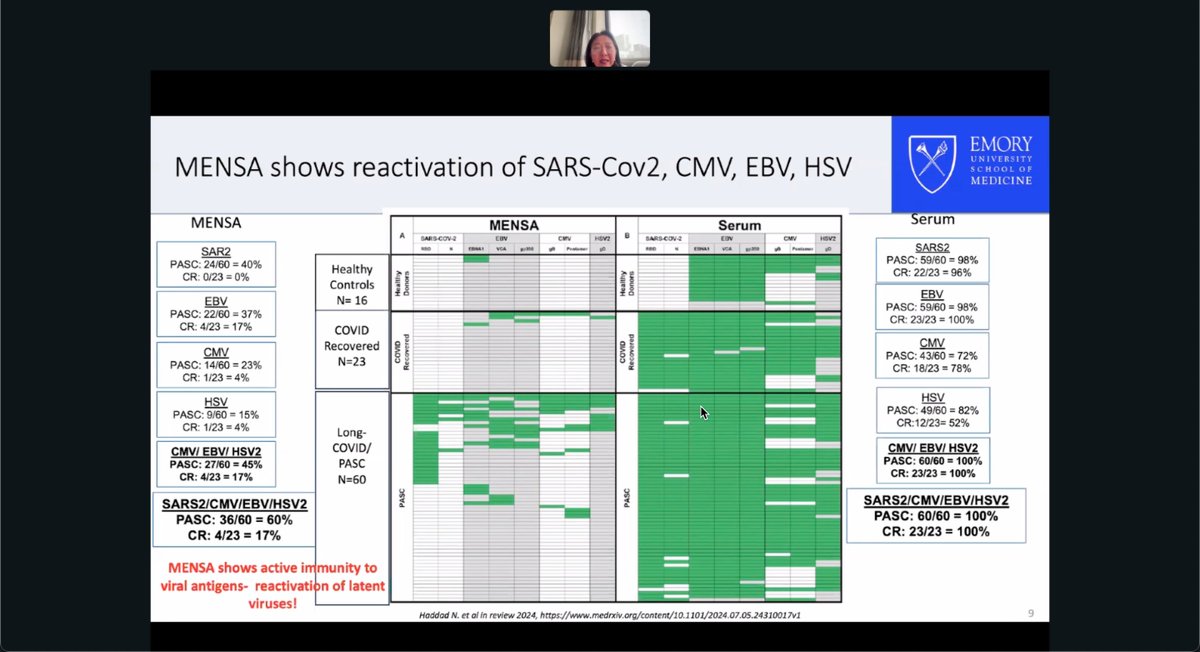
38/ Emory study finds 60% of people with long COVID show active immune responses to SARS-CoV-2, EBV, CMV, or HSV in MENSA, vs just 17% of recovered. This suggests viral reactivation, not just memory, may drive persistent symptoms.
39/ PolyBio trial shows 33% of long COVID patients had active antibody-secreting cells to SARS-CoV-2 (vs 100% memory in serum), supporting ongoing viral activity. MENSA testing may help identify those who could benefit from antiviral treatment.
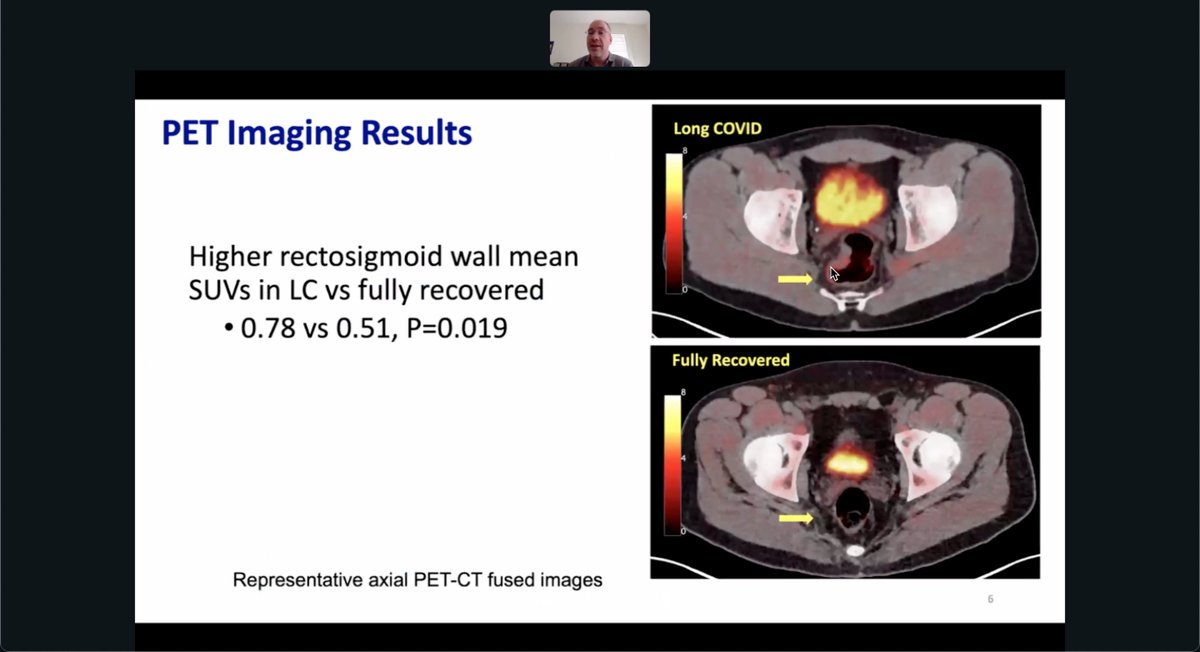
40/ Tim Henrich explains how PET imaging shows long COVID patients have significantly higher rectosigmoid wall inflammation than those fully recovered, with mean SUV 0.78 vs 0.51 (P = 0.019), supporting localized gut immune activation in long COVID.
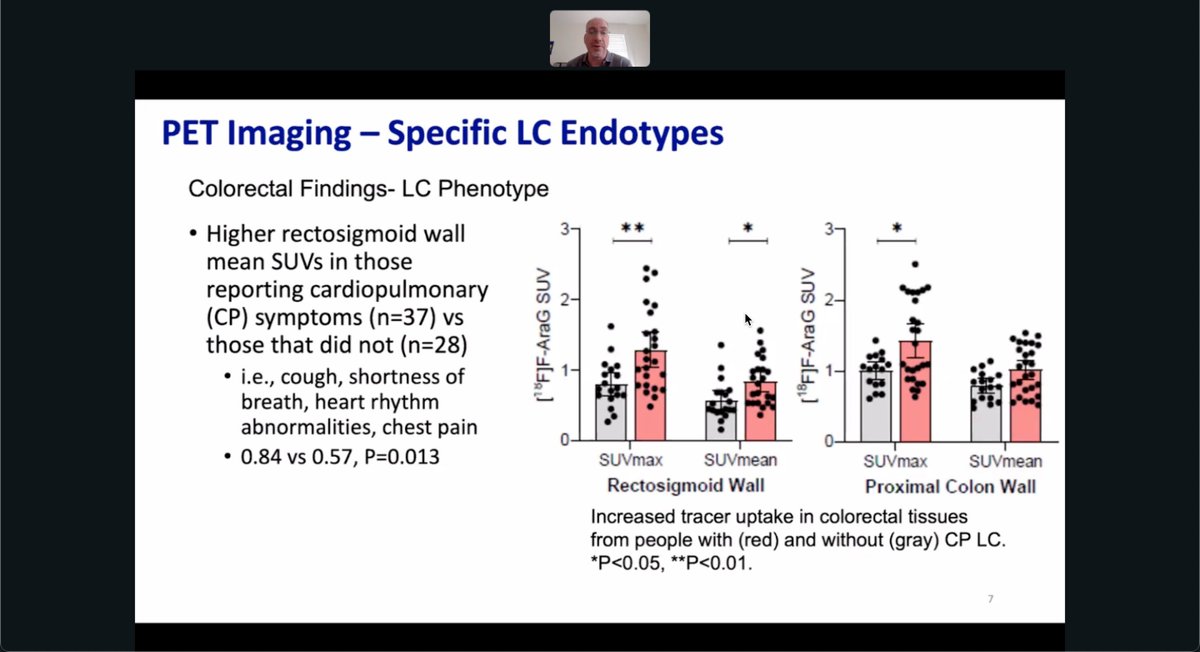
41/ PET scans of 65 long COVID patients show those with cardiopulmonary symptoms had higher rectosigmoid wall inflammation (SUVmean 0.84 vs 0.57, P = 0.013), linking gut immune activation to systemic symptoms like chest pain and shortness of breath.
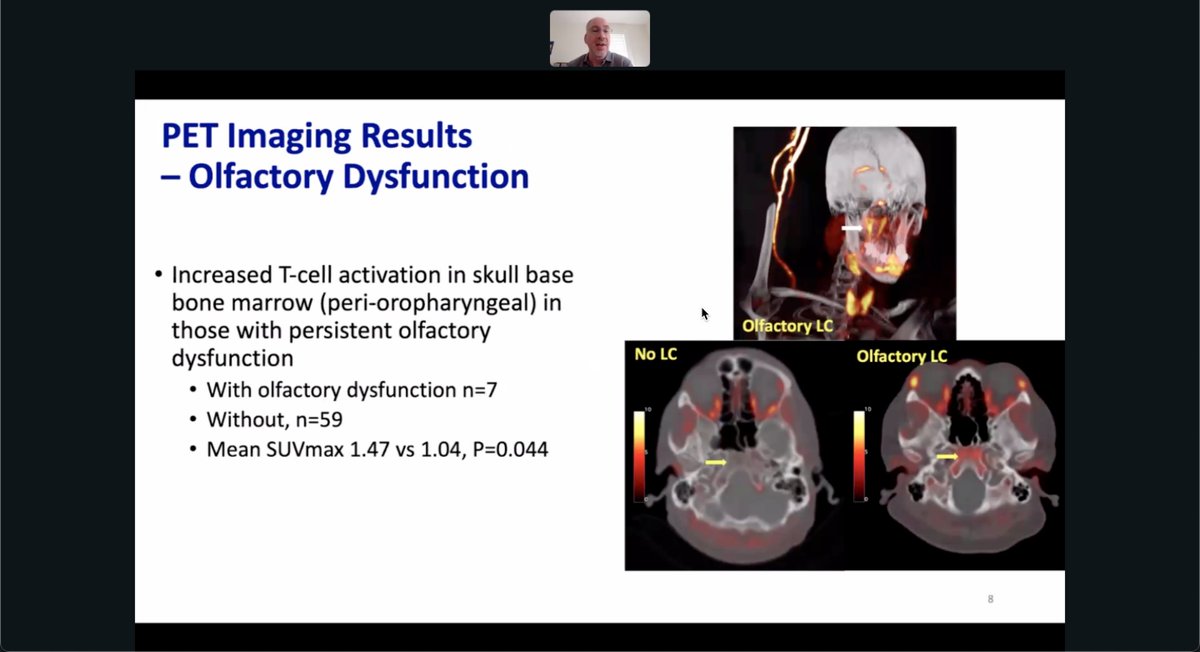
42/ PET imaging in 66 patients found that those with long COVID and persistent smell loss (n=7) had elevated T-cell activation in skull base marrow, with SUVmax 1.47 vs 1.04 in others (P = 0.044), linking immune activity to olfactory symptoms.
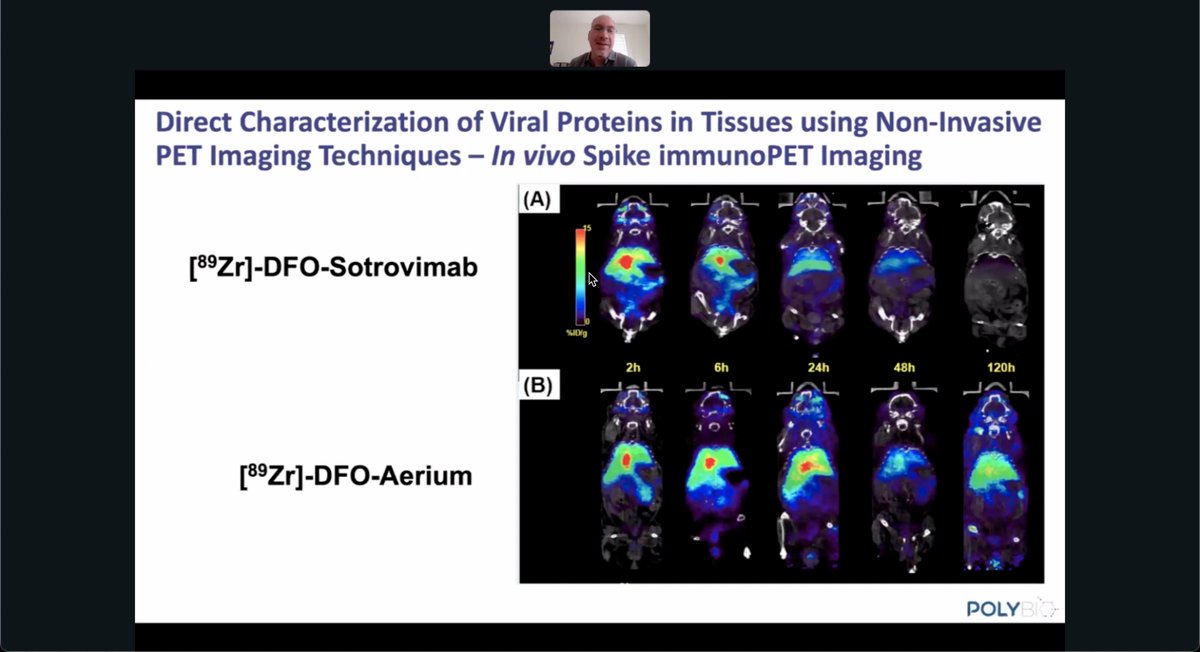
43/ At UCSF, [⁸⁹Zr]-DFO-Sotrovimab PET imaging, now IND-pending, revealed in vivo tissue localization of SARS-CoV-2 spike protein. Signal persisted up to 120 hours, supporting viral persistence in long COVID. [⁸⁹Zr]-DFO-Aerium showed similar targeting.
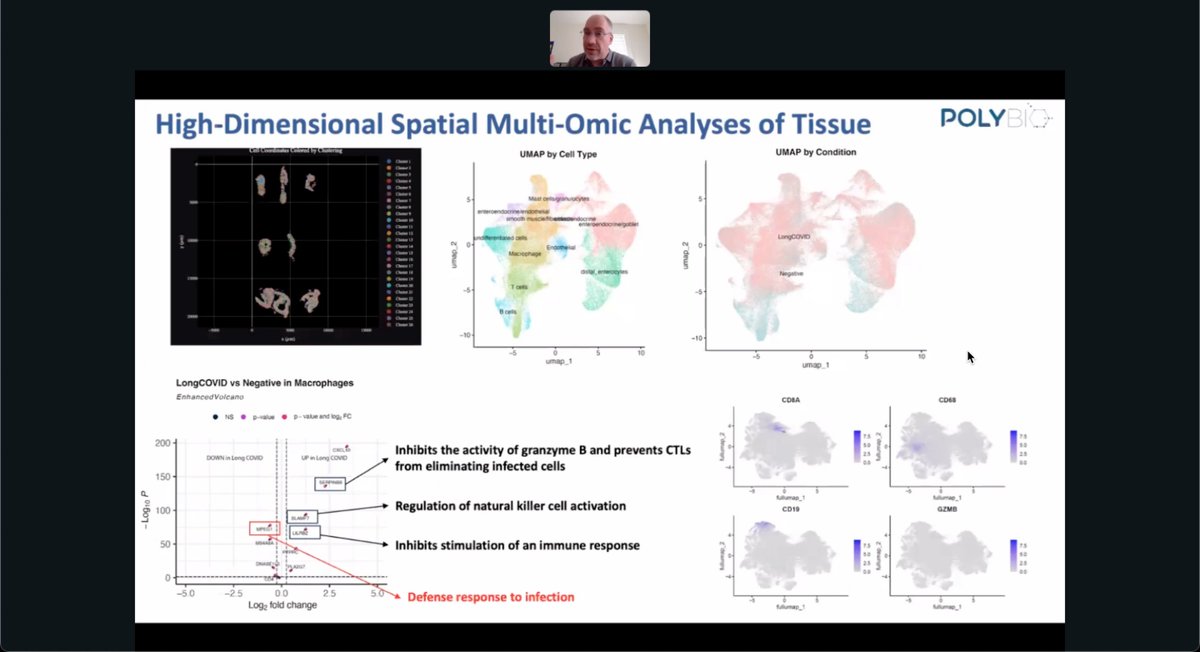
44/ At UCSF, spatial multi-omic profiling of gut biopsies showed distinct immune signatures in long COVID. Macrophages upregulated genes like SLAMF7 and LILRB1, which inhibit cytotoxic responses and promote viral persistence.
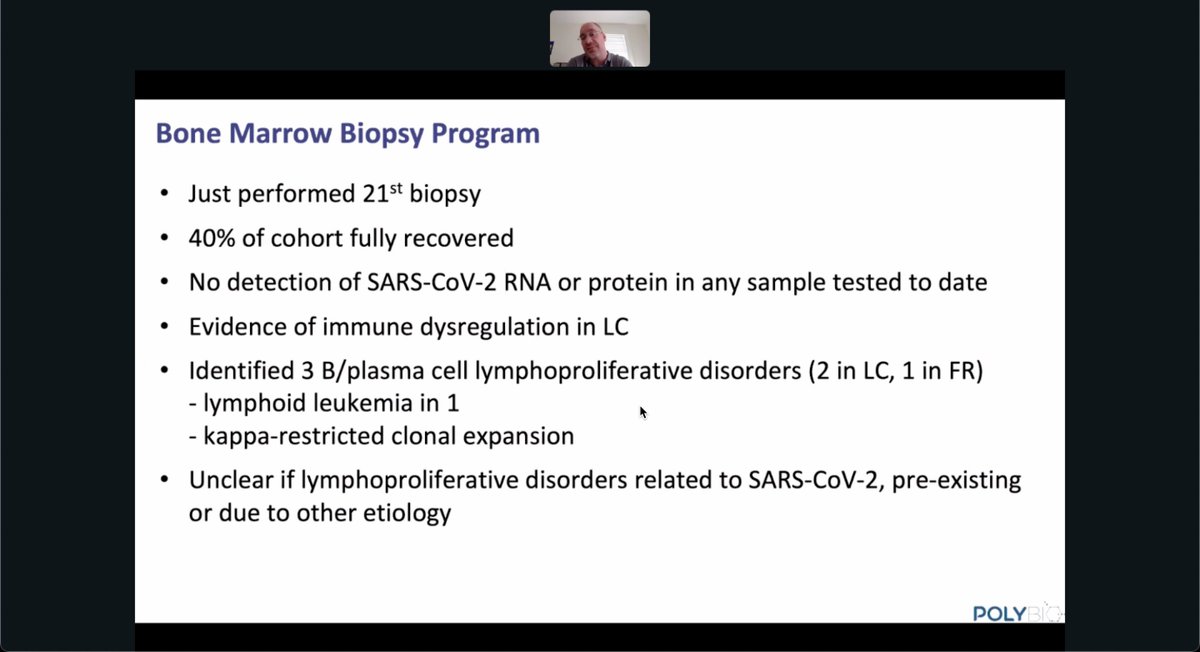
45/ At UCSF, bone marrow biopsies from 21 participants found no SARS-CoV-2 RNA or protein but revealed immune dysregulation in long COVID. Three lymphoproliferative disorders were detected, though links to SARS-CoV-2 remain unclear.
46/ Huaitao Cheng studied 10 patients with GI long COVID and 7 controls, finding inflammation, dysbiosis, and nutrient malabsorption. Tissue analyses included single-cell RNA-seq, bulk RNA-seq, microbiome profiling, and ddPCR.

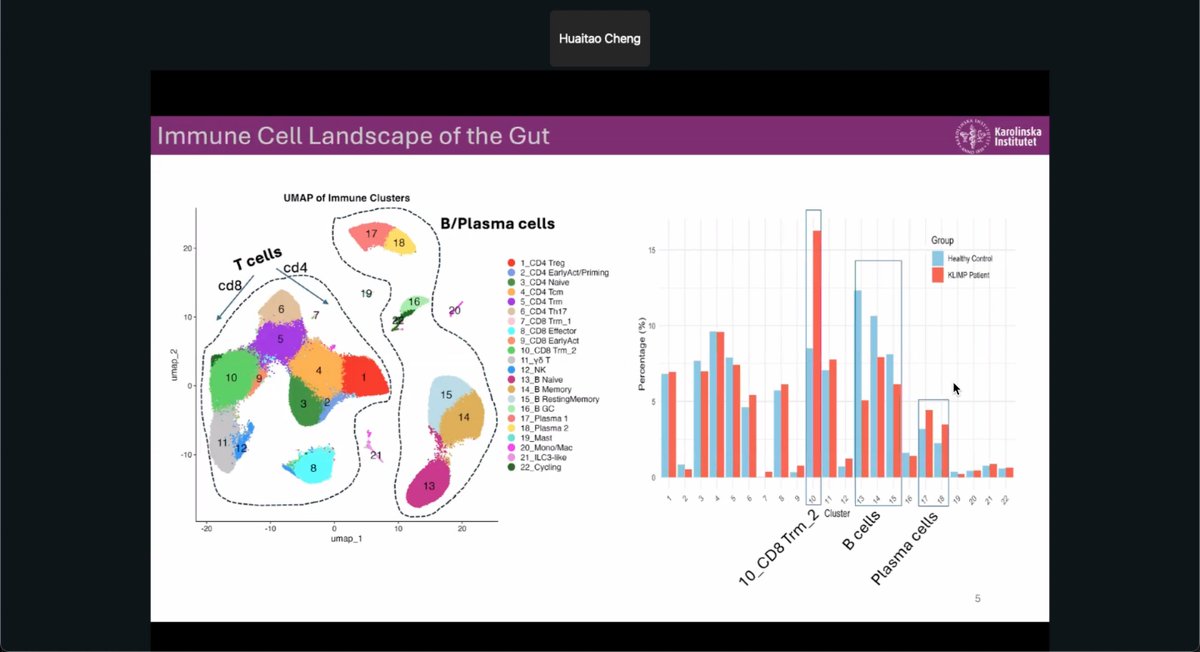
47/ At Karolinska Institutet, single-cell gut profiling revealed that patients with GI long COVID had more plasma cells and fewer B cells and CD8 Trm cells compared to healthy controls, suggesting disrupted local immune regulation.
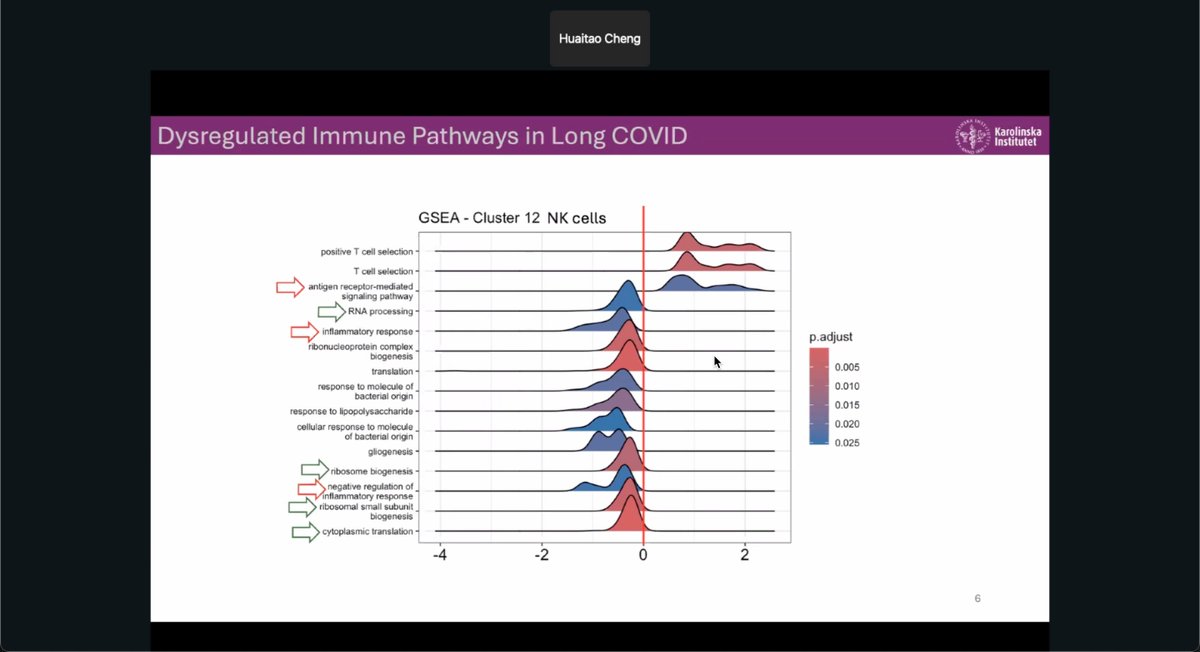
48/ NK cells from long COVID patients showed dysregulation in inflammatory, ribosomal, and antigen signaling pathways, indicating broad disruption in immune regulation and cellular stress responses.
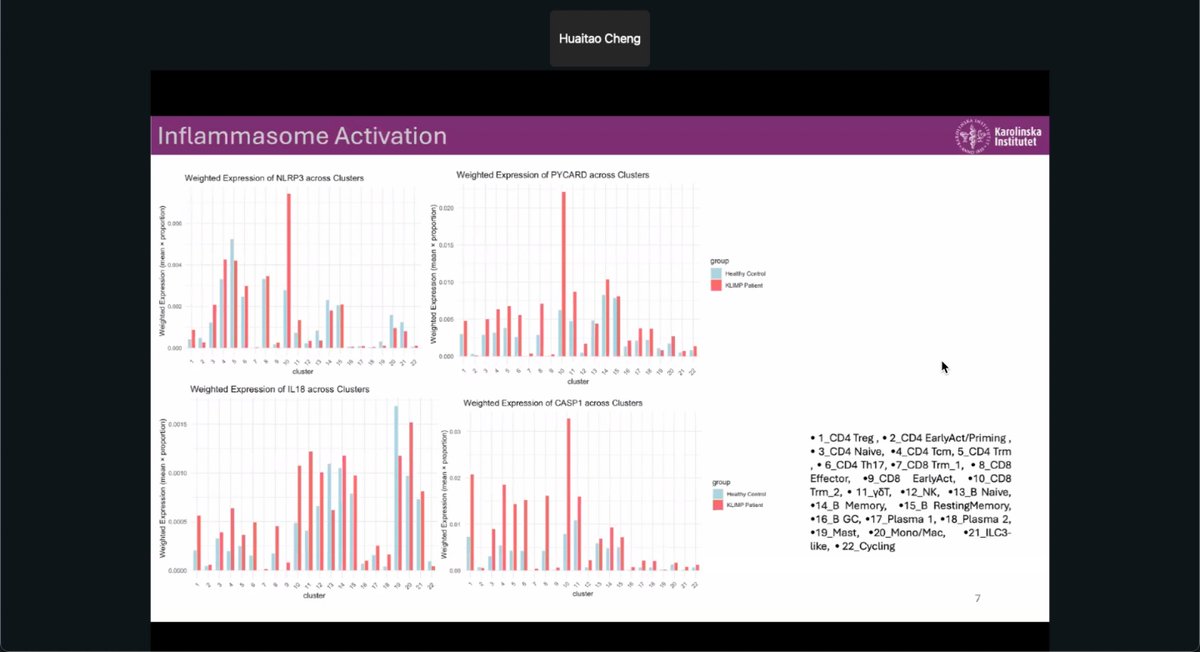
49/ Gut immune cells from long COVID patients showed elevated expression of NLRP3, PYCARD, IL18, and CASP1, key inflammasome genes, pointing to persistent innate immune activation and inflammation.
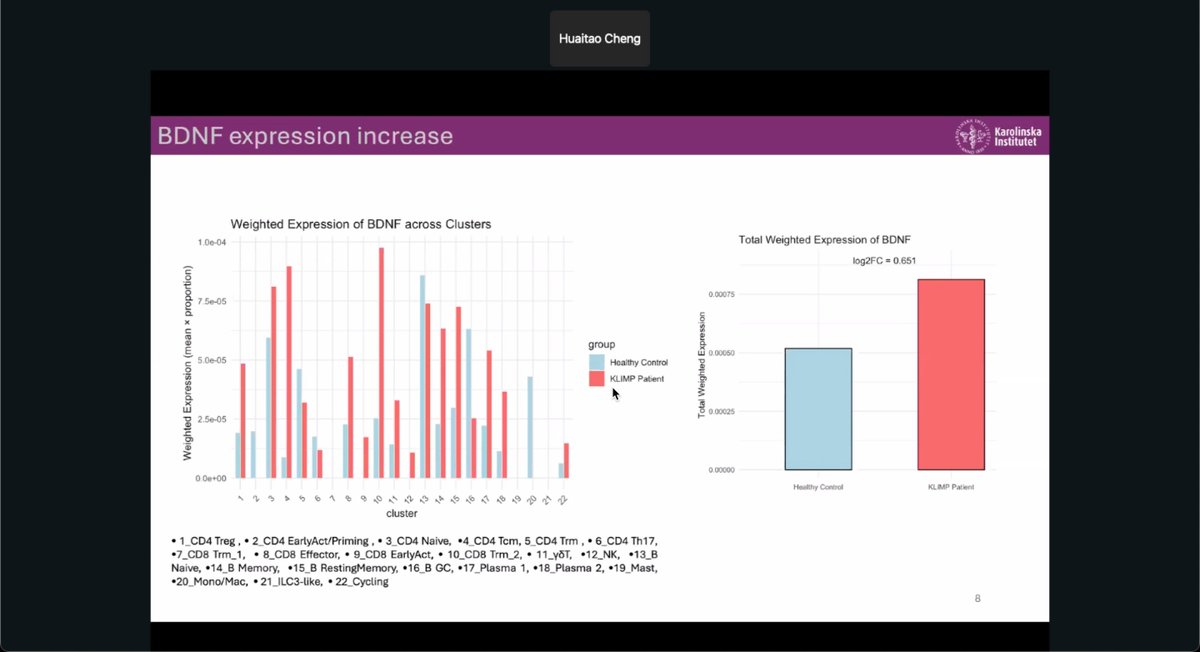
50/ Gut immune cells from long COVID patients showed increased BDNF expression compared to controls, suggesting altered neuroimmune signaling that may influence gut-brain interactions in long COVID.
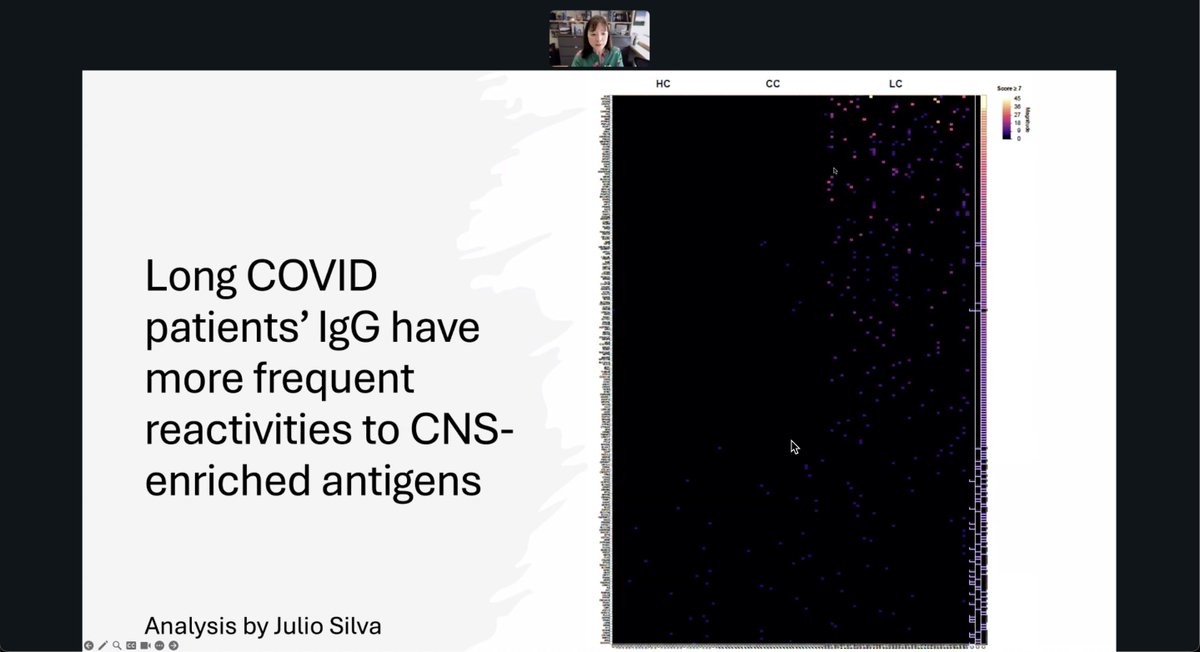
51/ Akiko Iwasaki found that 55 long COVID patients had significantly higher IgG reactivity to human neural tissues, including the thalamus, than 42 convalescent and 39 healthy controls, suggesting potential autoimmune targeting in long COVID.

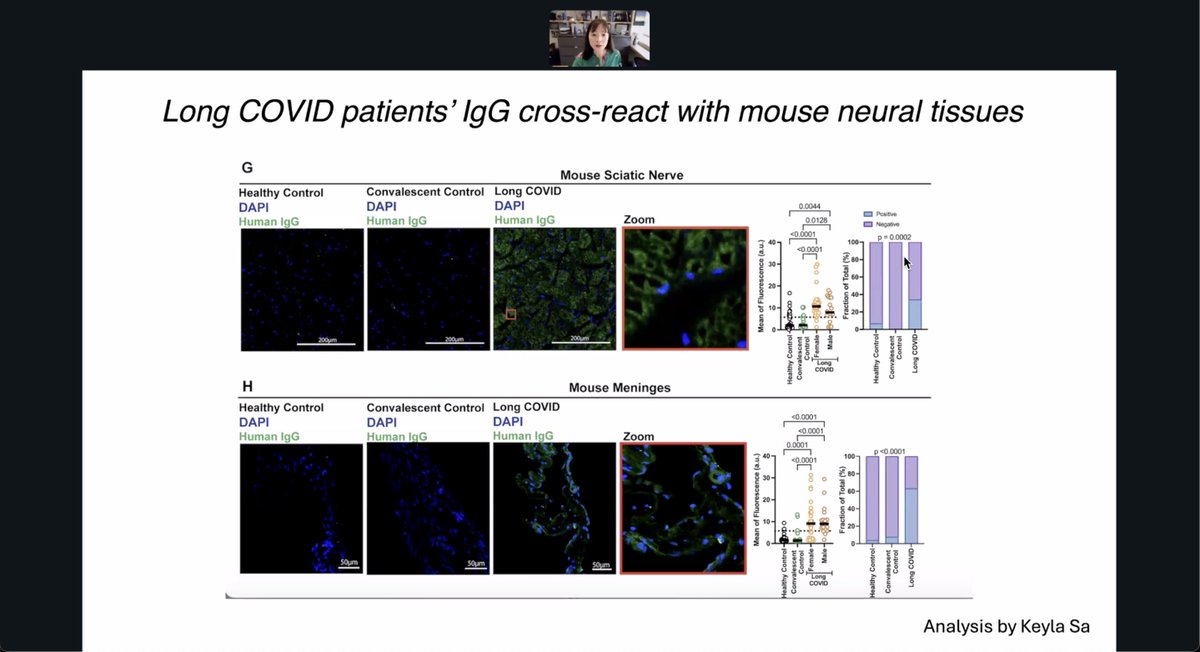
52/ IgG from 55 long COVID patients showed strong cross-reactivity with mouse neural tissues, including sciatic nerve and meninges, significantly more than controls, suggesting potential autoantibody-driven neuroinflammation in long COVID.
53/ 12 long COVID patients with headaches had IgG that strongly cross-reacted with mouse meninges, showing elevated fluorescence and perivascular localization, suggesting antibody-driven neuroinflammation linked to headache symptoms.

54/ IgG from long COVID patients showed markedly more frequent reactivity to CNS-enriched antigens compared to controls, indicating a potential autoimmune component targeting the central nervous system.
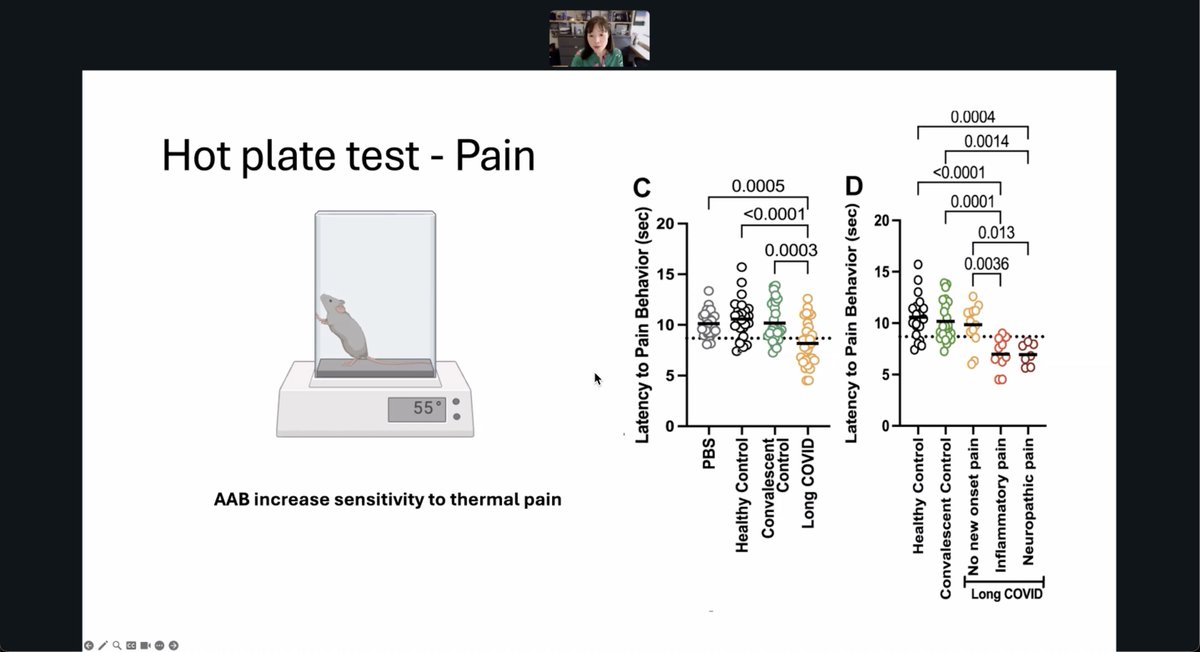
55/ IgG from long COVID patients reduced latency to pain behavior in mice during a hot plate test, suggesting autoantibodies may increase thermal pain sensitivity, particularly in those with neuropathic or inflammatory symptoms.
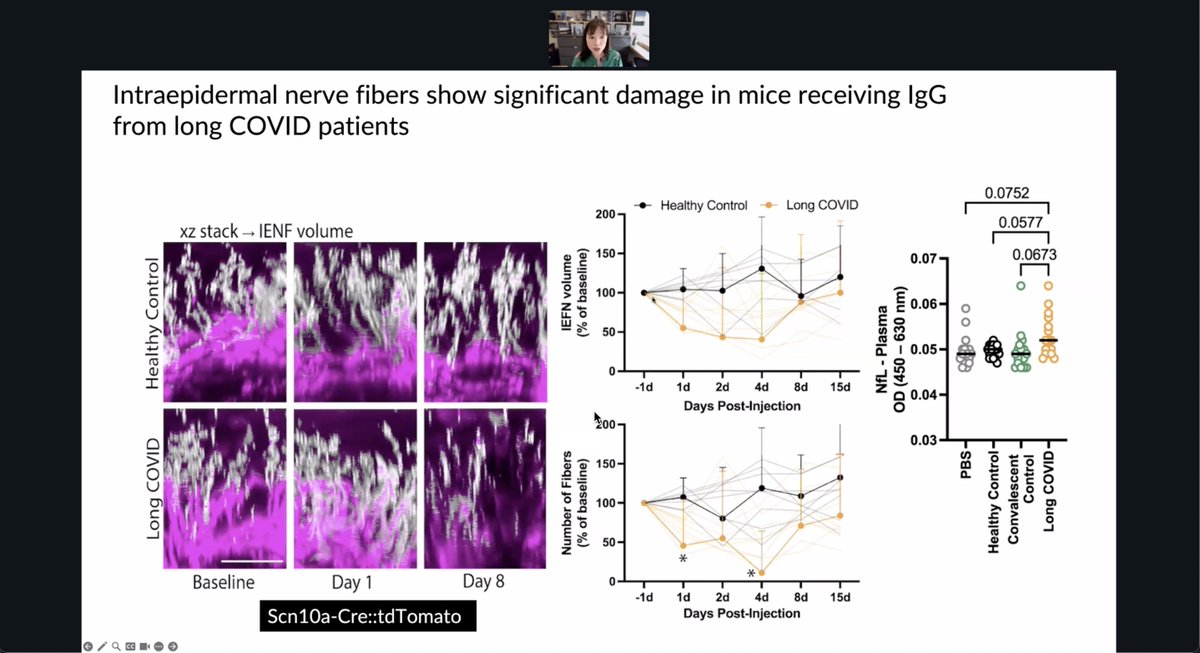
56/ Mice injected with IgG from long COVID patients showed rapid intraepidermal nerve fiber loss by day 1, supporting a direct autoimmune contribution to nerve damage and sensory symptoms in long COVID.
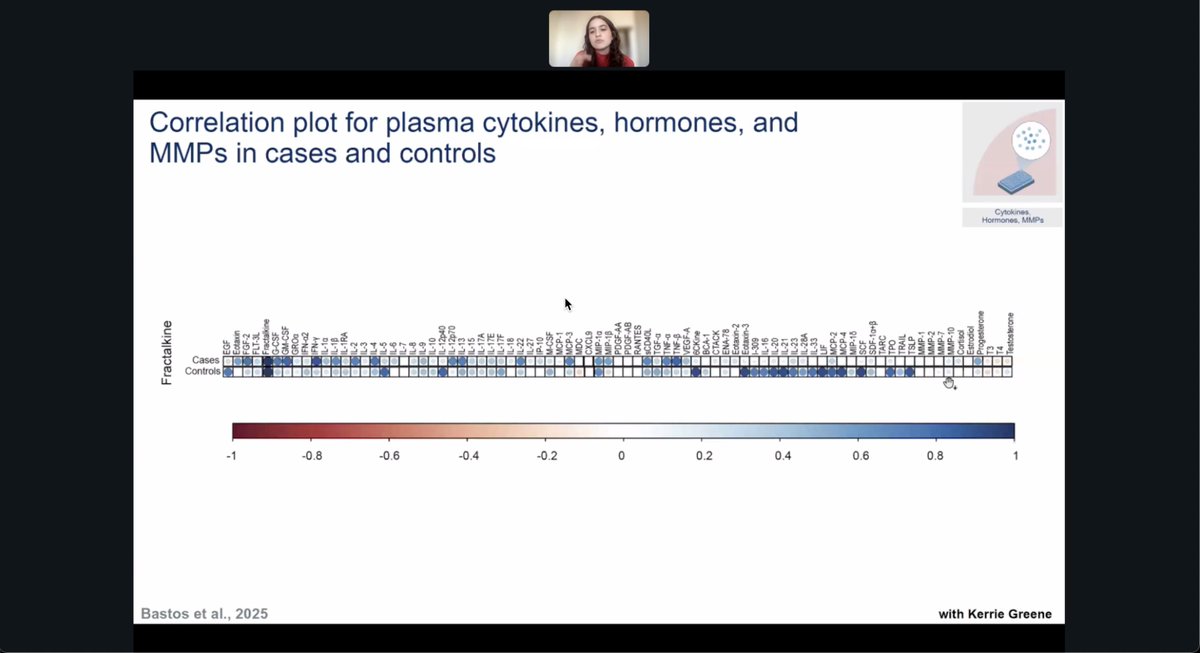
57/ Stronger correlations between fractalkine and multiple immune markers in long COVID patients compared to controls, highlighting altered signaling between chemokines, cytokines, and MMPs that may drive persistent inflammation.
58/ Identified two distinct clusters of long COVID cases based on CSF matrix metalloproteinase profiles, suggesting different patterns of tissue remodeling and neuroinflammation among patients.

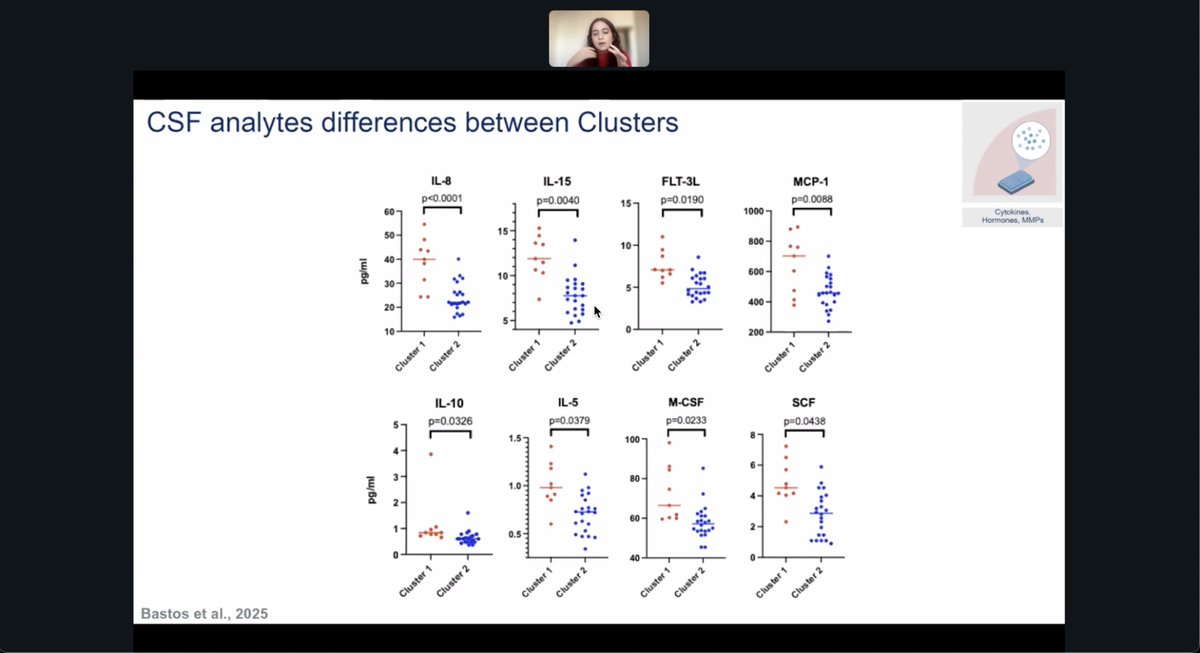
59/ Found that CSF analytes like IL-8, IL-15, and MCP-1 significantly differ between long COVID patient clusters, suggesting biologically distinct subtypes with different inflammatory profiles.
60/ Found distinct long COVID clusters show different seropositivity to viruses like SARS-CoV-2, HSV, and parvovirus B19, hinting at varied prior exposures or reactivations shaping immune profiles.
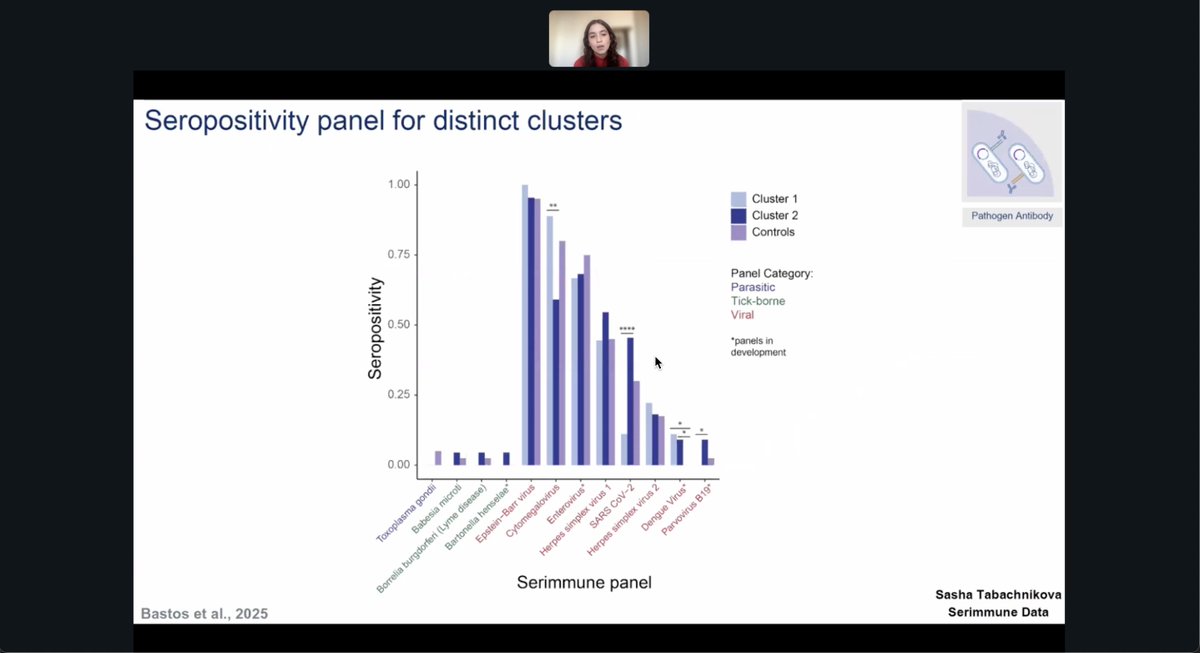
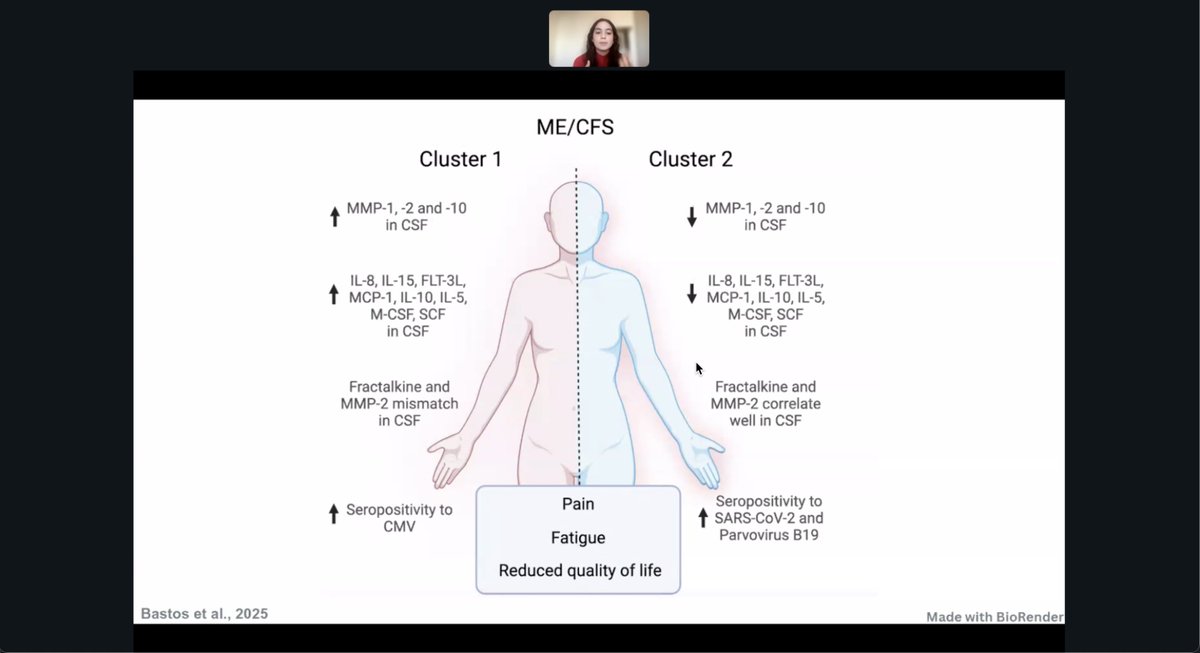
61/ Two ME/CFS clusters were identified with distinct CSF immune profiles and viral serologies. Cluster 1 showed elevated cytokines and CMV exposure, while Cluster 2 showed higher SARS-CoV-2 and parvovirus B19 seropositivity. Both shared fatigue and pain.
62/ Proposes that the nucleus of the solitary tract may mediate vagus nerve-driven sickness symptoms in Long COVID by linking gut-derived signals to brain circuits, raising questions about vagus sensitization and immune–brain crosstalk.

63/ A pilot study with 4 Long COVID patients and 8 controls found significantly elevated BOLD signals in the nucleus of the solitary tract after vagus nerve stimulation, suggesting altered brainstem activity in Long COVID.

64/ Brain imaging in 5 Long COVID patients and 8 controls showed greater activation in brainstem regions like the nucleus of the solitary tract during vagus stimulation, hinting at brainstem hypersensitivity in Long COVID.

65/ Tissue models showed SARS-CoV-2 clears quickly in bronchial cultures but persists in intestinal ones. Drug responses differ too—molnupiravir worked in lungs but not gut, highlighting unique challenges in treating GI infections.

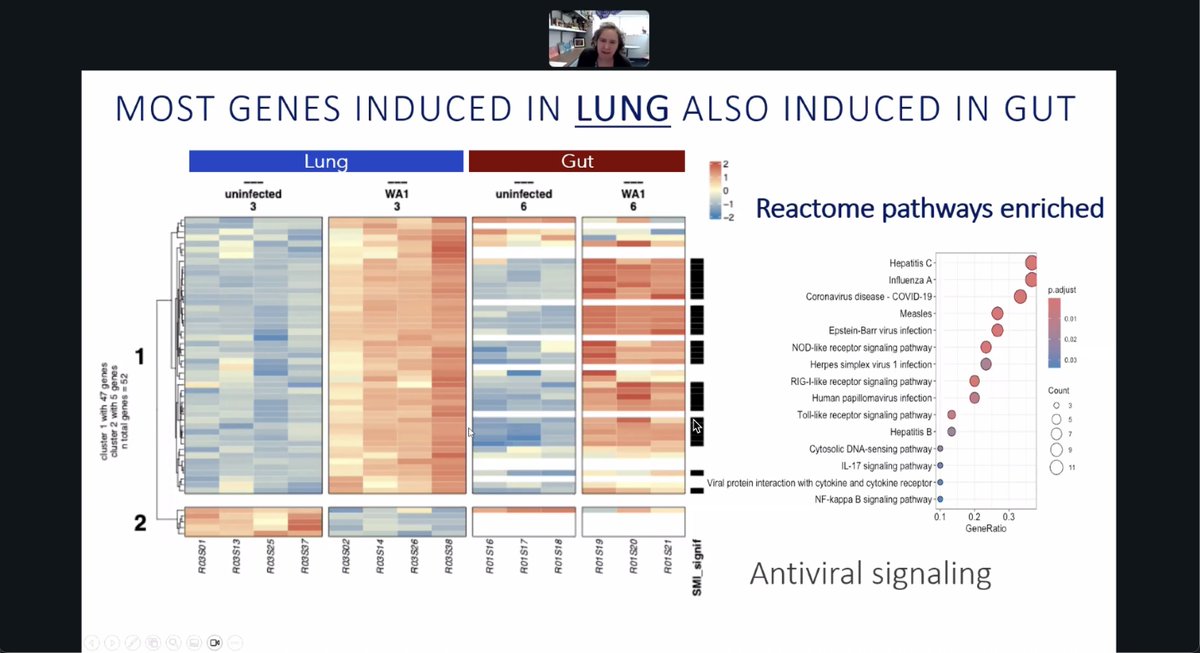
66/ Lung and gut cells infected with SARS-CoV-2 showed shared antiviral gene activation but different kinetics and sensitivities, reinforcing that SARS-CoV-2 infection behaves distinctly across tissue types.
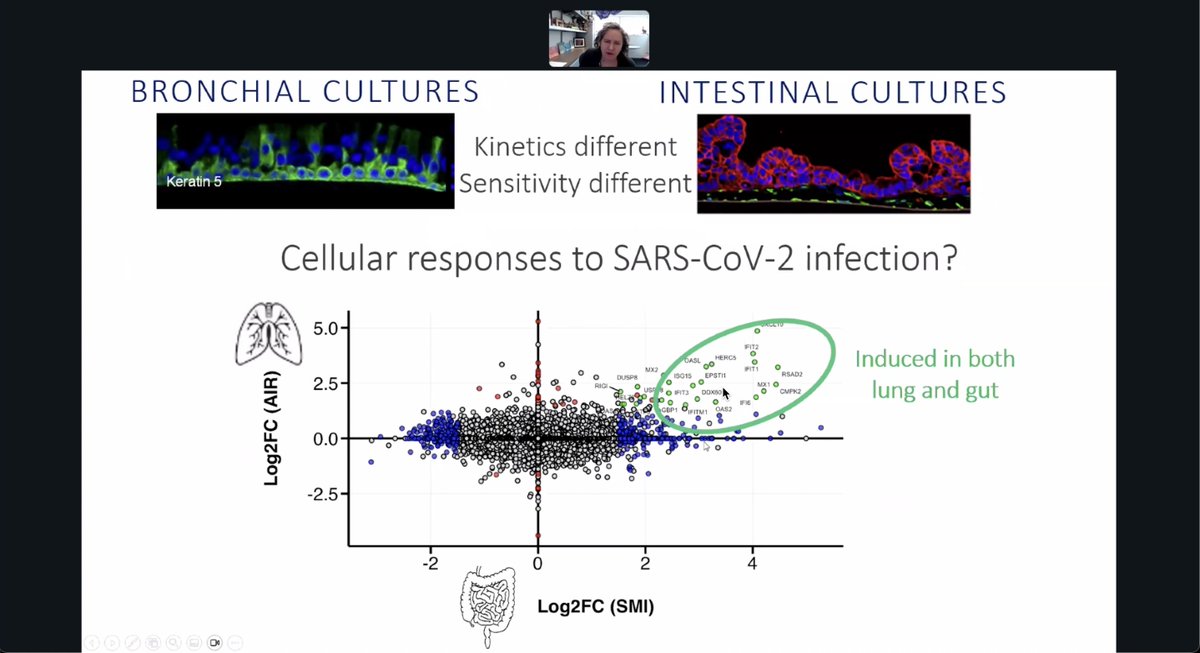
67/ Lung and gut cultures exposed to SARS-CoV-2 shared most upregulated genes, activating overlapping antiviral pathways like RIG-I and NOD-like receptor signaling, despite tissue-specific infection kinetics.
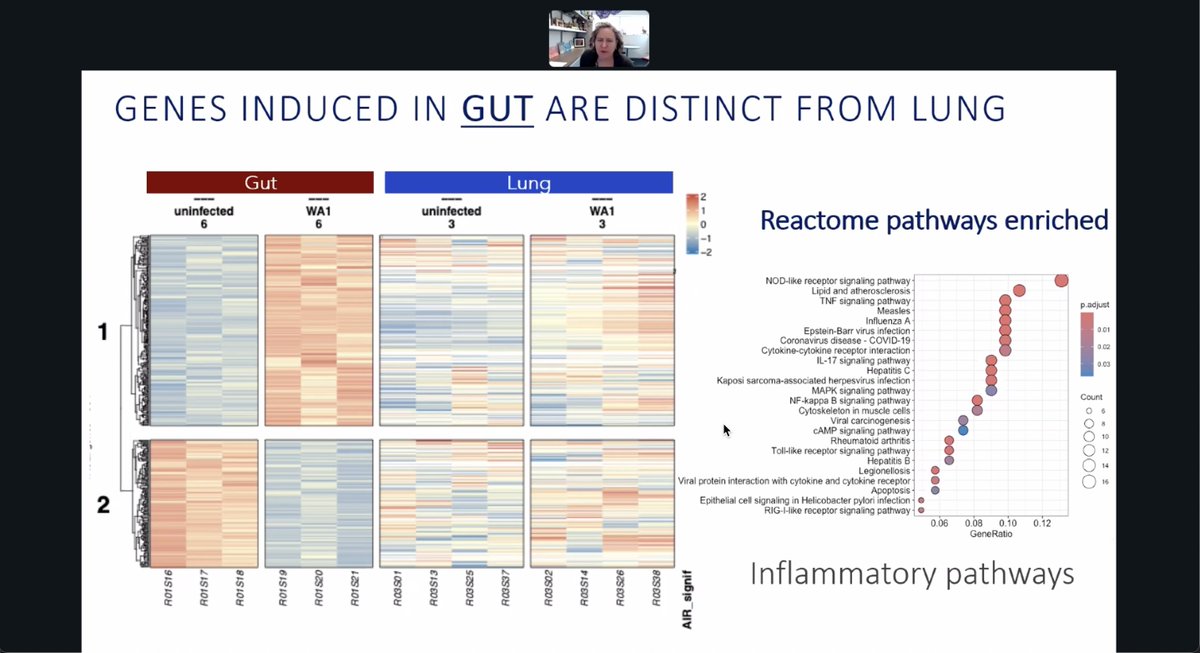
68/ Genes uniquely induced in SARS-CoV-2–infected gut cultures activated distinct inflammatory pathways, including NF-κB, IL-17, and TNF, highlighting GI-specific immune signaling compared to the lung.
69/ SARS-CoV-2 tissue models show IFN-β reduces viral RNA in both lung and gut, while JAK or NFκB inhibition reverses this effect, suggesting immune modulation may need site-specific strategies for COVID-19 persistence.

70/ Intestinal epithelial cells secrete cytokines that may drive systemic pathology, raising the possibility of combining immunomodulators with antivirals to treat chronic viral persistence more effectively.

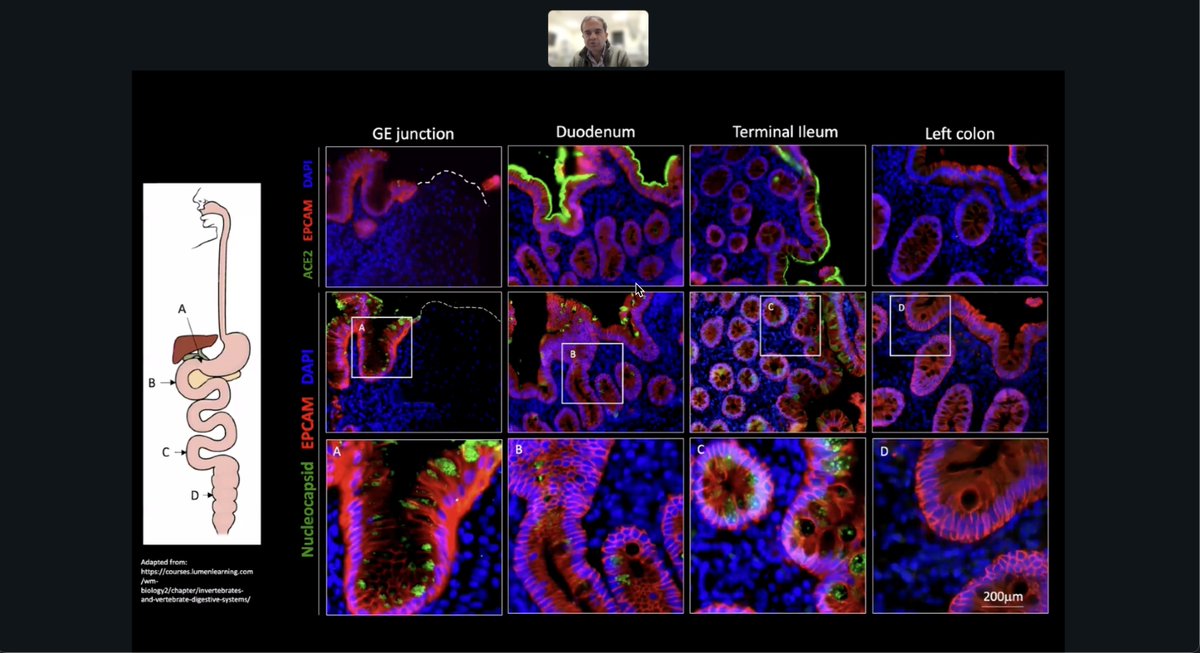
71/ Researchers visualized SARS-CoV-2 nucleocapsid protein in human GI tissues, showing viral persistence in the duodenum and ileum months post-infection, with strong ACE2 expression at epithelial surfaces suggesting ongoing viral-host interaction.
72/ RNA-seq analysis of GI tissues from COVID-19 patients showed reduced dendritic and other myeloid cells but increased goblet and epithelial subtypes, suggesting disrupted gut immunity and altered barrier function during infection.

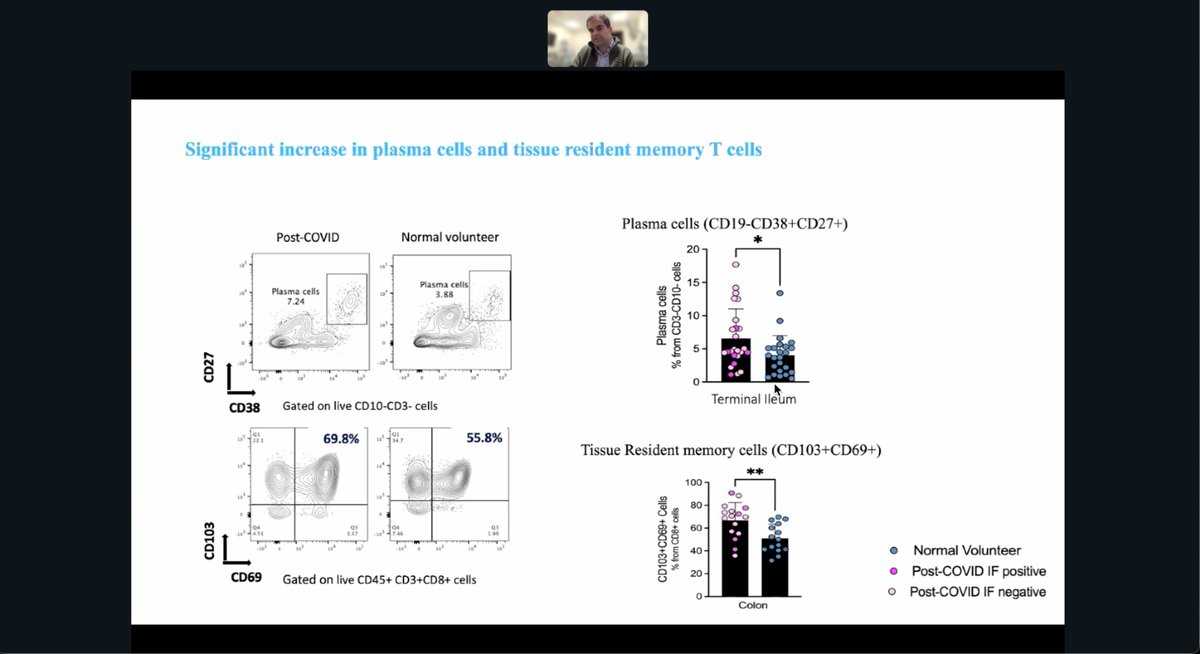
73/ Post-COVID patients had more plasma cells in the terminal ileum and more tissue-resident memory T cells in the colon than healthy controls, pointing to persistent mucosal immune activation after infection.
74/ Researchers showed SARS-CoV-2 can infect and replicate in human lung macrophages, triggering inflammasome activation and inflammatory cytokine release, suggesting a direct mechanism for immune-driven lung pathology.

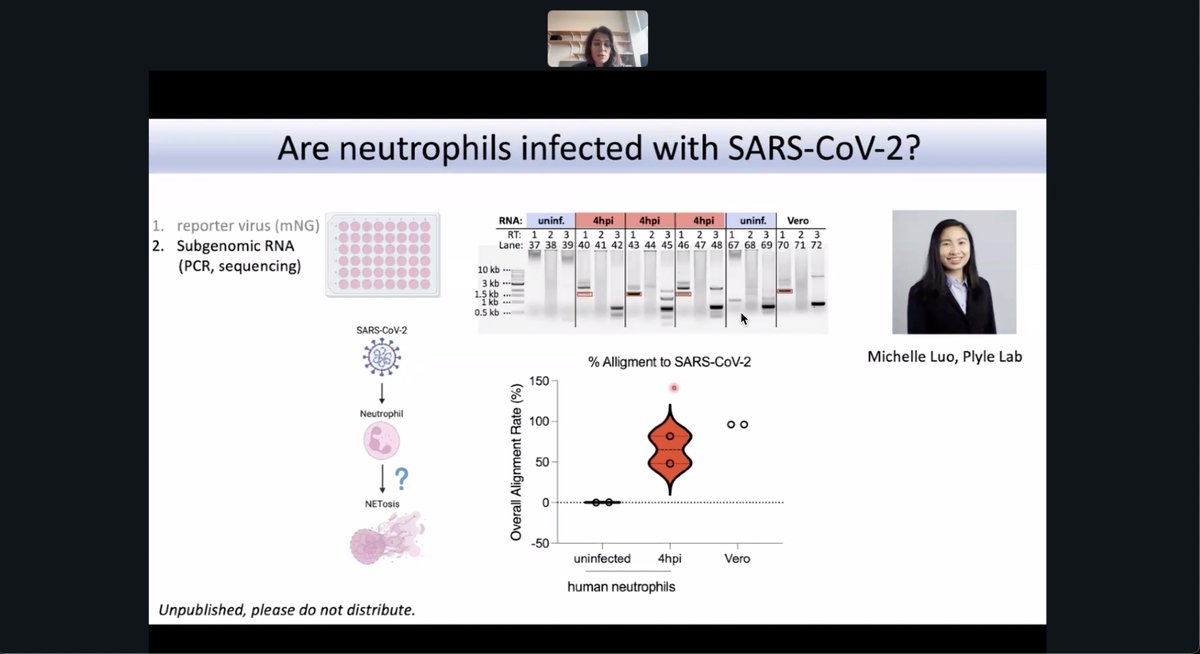
75/ SARS-CoV-2 can enter human neutrophils, with 38% becoming virus-positive—a signal suppressed by Paxlovid—suggesting active infection and a possible link to NETosis in COVID-19.

76/ Subgenomic RNA of SARS-CoV-2 in human neutrophils 4 hours post-infection, with alignment rates approaching those in Vero cells, suggesting active viral replication in this immune cell type.
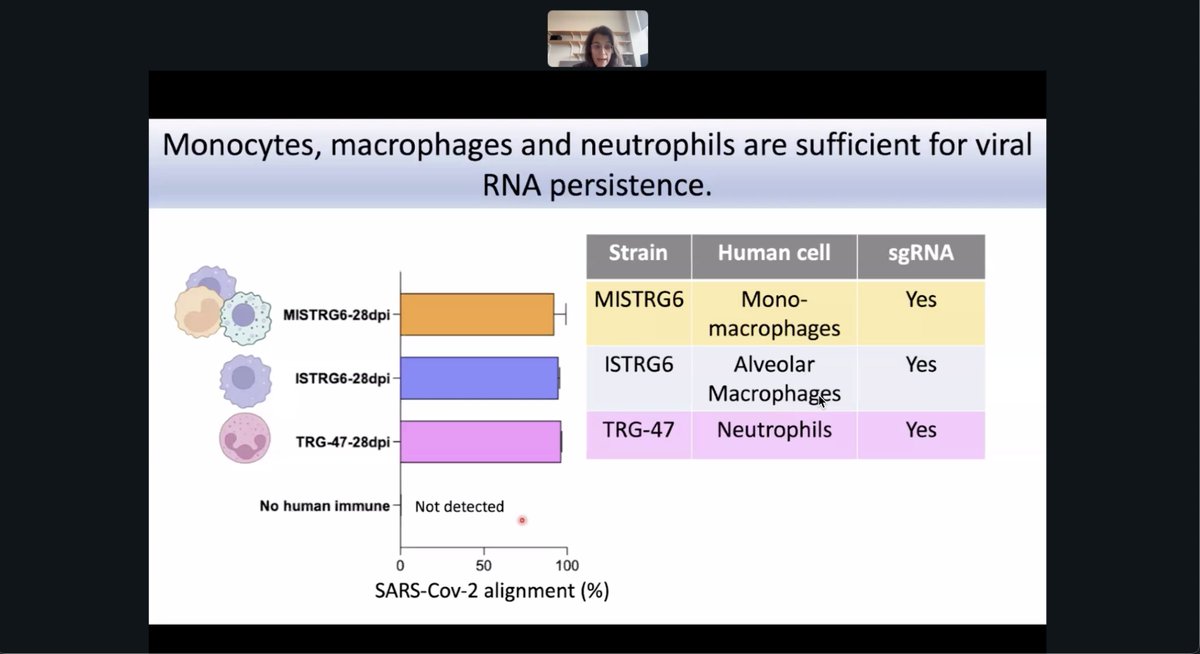
77/ Viral RNA persists in humanized mice via monocytes, macrophages, and neutrophils, all showing subgenomic RNA and high SARS-CoV-2 alignment, confirming these cells support RNA persistence.
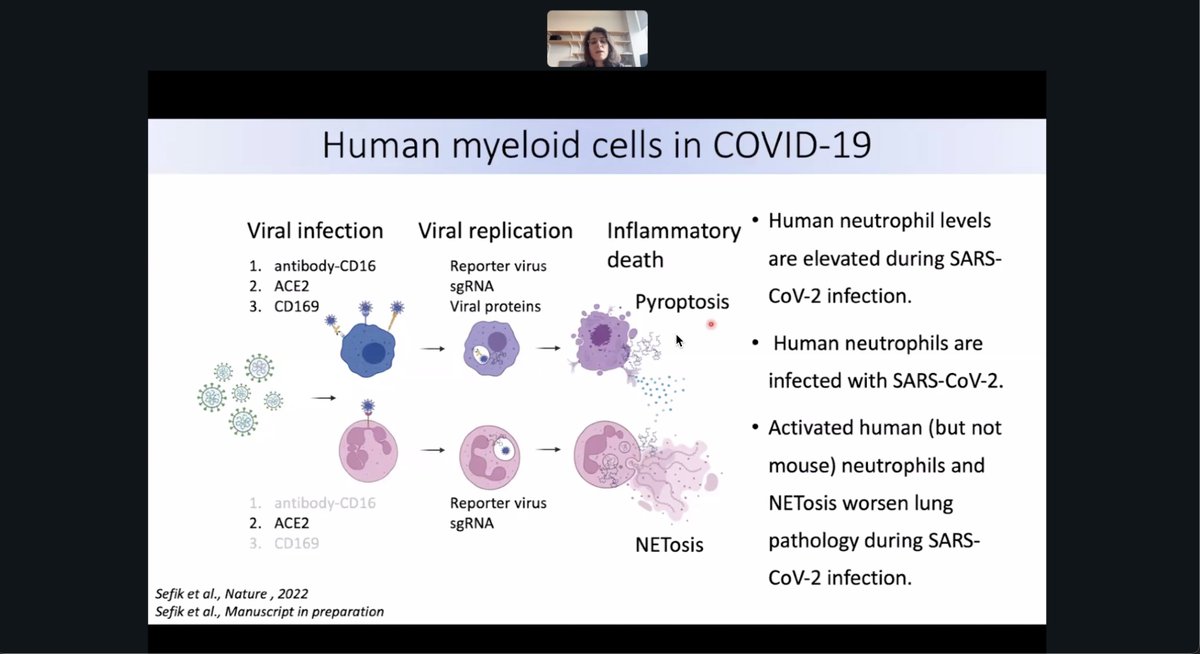
78/ Human neutrophils are infected by SARS-CoV-2 and undergo NETosis, while monocytes and macrophages support viral replication and trigger pyroptosis, collectively driving lung inflammation in COVID-19.
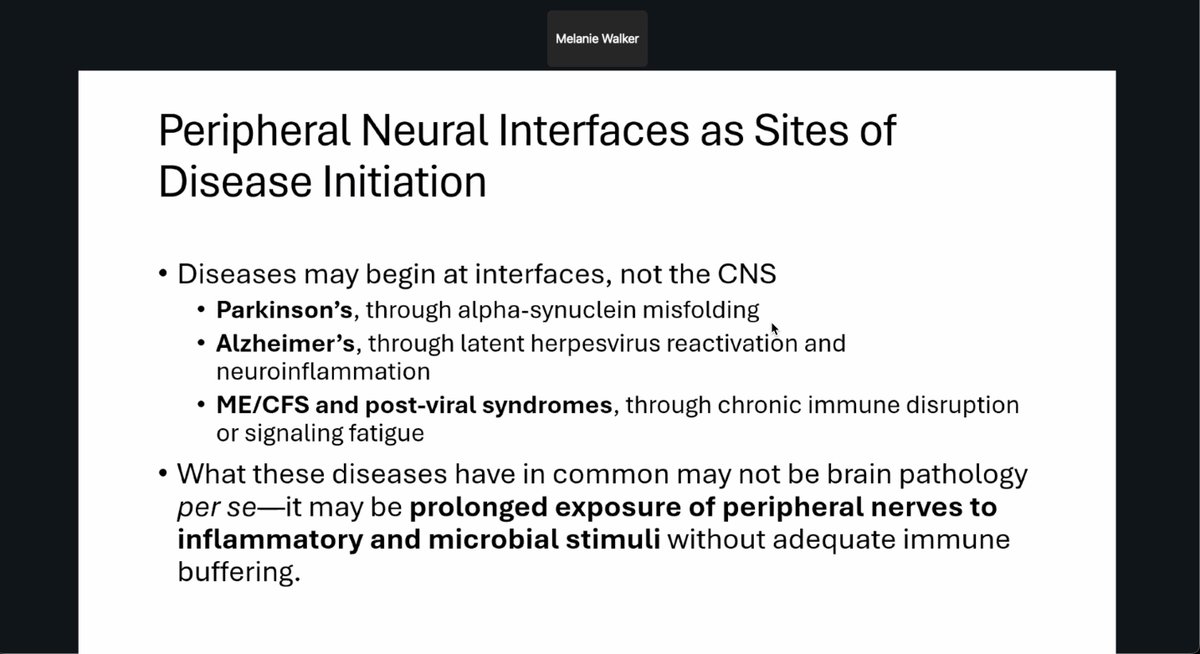
79/ Melanie Walker suggest diseases like Parkinson’s, Alzheimer’s, and ME/CFS may begin at peripheral neural interfaces, where prolonged immune exposure—not central brain pathology—triggers dysfunction.
80/ Wanting to collect vagus nerves within 30 minutes of organ procurement to study neuro-immune interfaces, preserving RNA and protein for analysis in the Human Virome Project.

81/ Steven Deeks shows validation of HIV biomarkers replaced severe clinical endpoints and fast-tracked drug approvals, transforming treatment with over 30 therapies approved between 1987 and 2020.

82/ The RAVEN network helps validate biomarkers of the HIV reservoir, crucial for cure strategies. Samples undergo deep analysis across multiple labs, from viral quantification to immune profiling.

83/ Researchers propose that Long COVID care could be transformed by a biomarker that is accessible, fast, scalable, prognostic, and responsive to treatment. The VIPER cohort aims to identify such a surrogate marker for disease tracking.
84/ The VIPER cohort tackles the Long COVID biomarker problem by unifying lab efforts through data sharing and central analysis, enabling deep phenotyping, consistent biomarker assessment, and future-ready, harmonized research across sites.

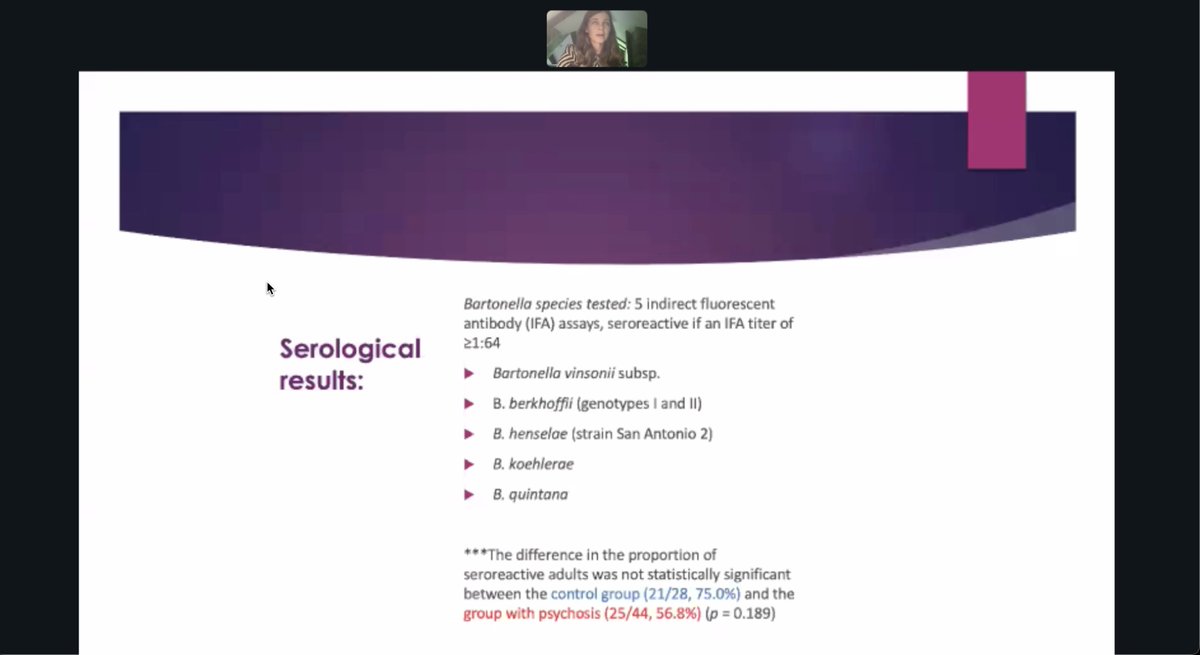
85/ Researchers found no statistically significant difference in Bartonella seroreactivity between adults with psychosis (56.8%) and controls (75%) using five IFA antibody tests across multiple species.
86/ 43.2% of adults with psychosis tested PCR-positive for Bartonella DNA, compared to 14.3% of controls. This difference was statistically significant with a p-value of 0.021.

87/ Shannon Stott isolated rare viral particles using ACE2-based capture, showing intact SARS-CoV-2 virions in blood by EM and dSTORM. ACE2 binding yielded significantly higher RNA copies than plasma capture, confirming specific enrichment.

88/ Clinical validation showed their assay detects multiple SARS-CoV-2 variants, including Omicron, with high specificity and minimal cross-reactivity. A blinded panel confirmed accurate quantification down to 4 copies/mL with strong linearity (R² = 0.97).

89/ They found viral particles in 72% of plasma, 62% of stool, and 43% of saliva samples from COVID patients, but none in pre-COVID healthy controls, confirming assay specificity and viral persistence across compartments.

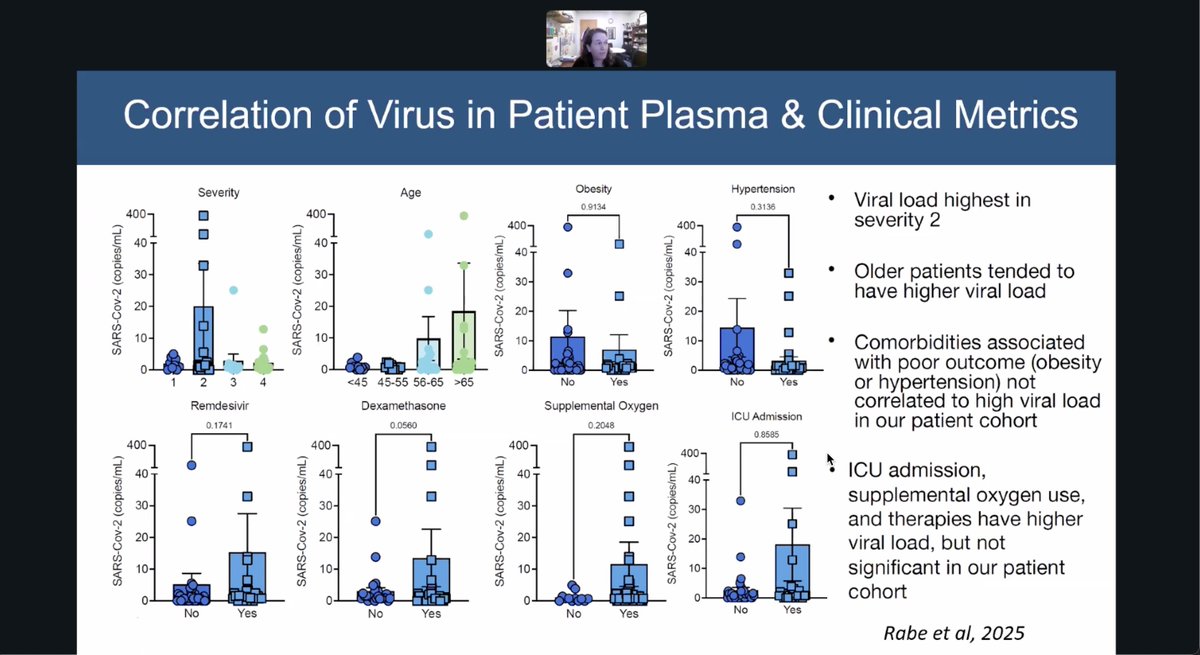
90/ Plasma viral load in COVID patients peaked in those with moderate severity and older age, but showed no strong correlation with obesity, hypertension, or ICU admission, highlighting complex links between viremia and outcomes.
91/ Serial blood monitoring in a COVID patient showed sharp viral decline after treatment, but low-level SARS-CoV-2 RNA persisted up to 100 days, suggesting prolonged viremia may occur even after clinical recovery.

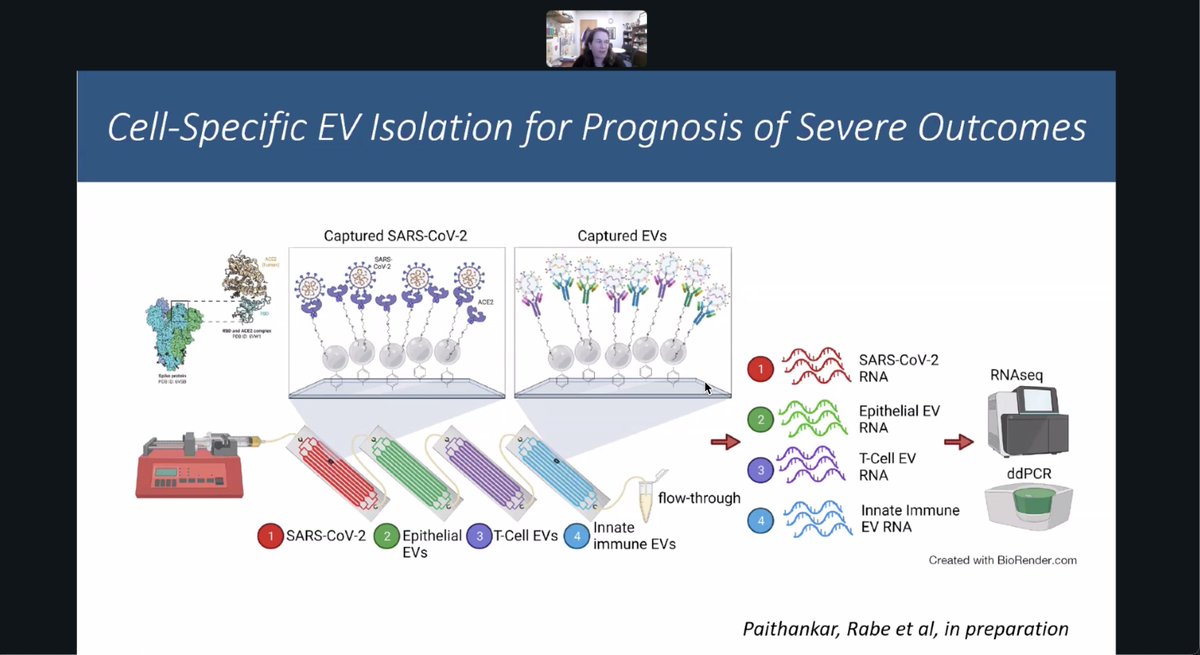
92/ Researchers developed a method to isolate extracellular vesicles by cell type, enabling RNA analysis from virus, epithelial, T cell, and innate immune sources to better predict severe COVID outcomes.
93/ A pending PolyBio grant aims to detect viral particles in long COVID using the HB-Chip on plasma from 100 individuals including long COVID, convalescent, acute, and pre-pandemic controls, with plans to expand the cohort and track samples over time.
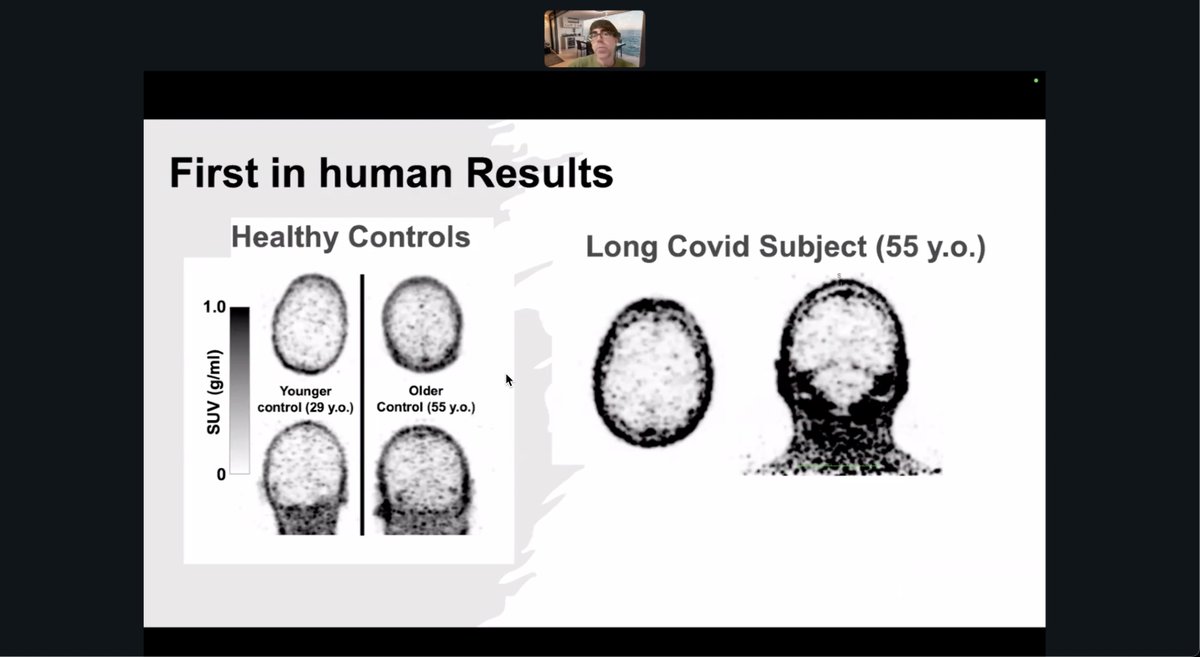
94/ In a first-in-human scan, a 55-year-old long COVID subject showed markedly higher brain tracer uptake compared to both younger and age-matched healthy controls, suggesting possible neuroinflammation or altered brain metabolism.
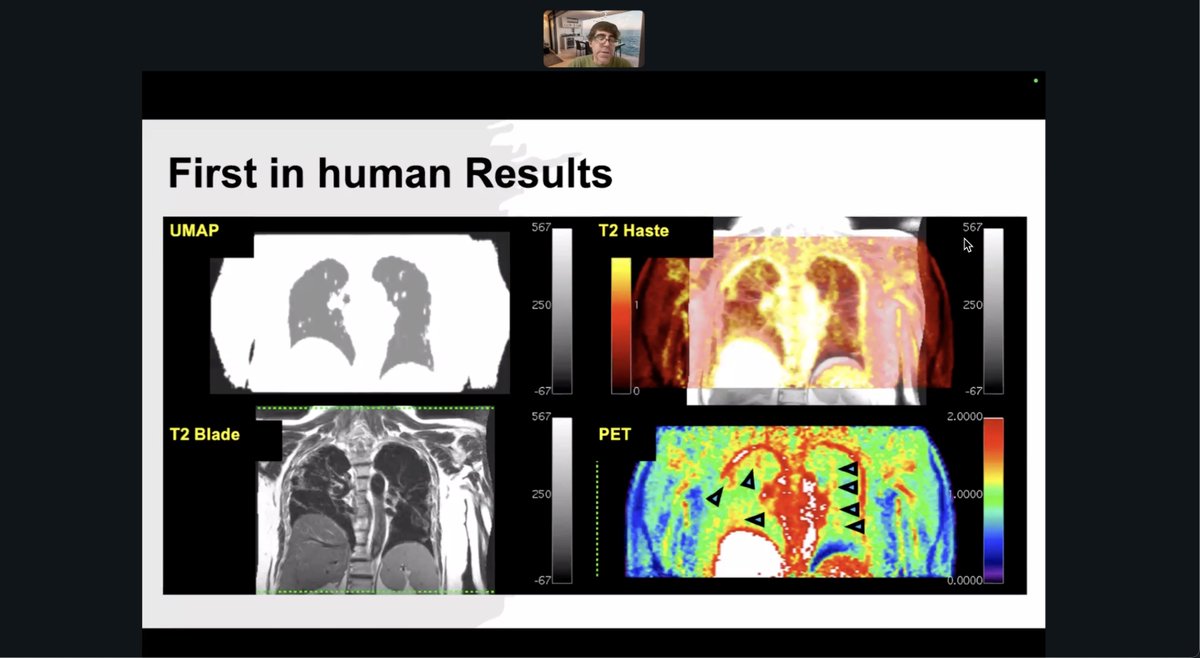
95/ PET and MRI imaging revealed elevated tracer uptake in lung tissue, marked by inflammation in regions where structural abnormalities were not visible, highlighting possible occult pathology.
96/ David Putrino shares the CoRE interventional trials that span both device-based and drug or supplement-based treatments for long COVID, including vagus nerve stimulation, lumbrokinase, rapamycin, and oxygen therapy, reflecting a multi-pronged approach to symptom relief.

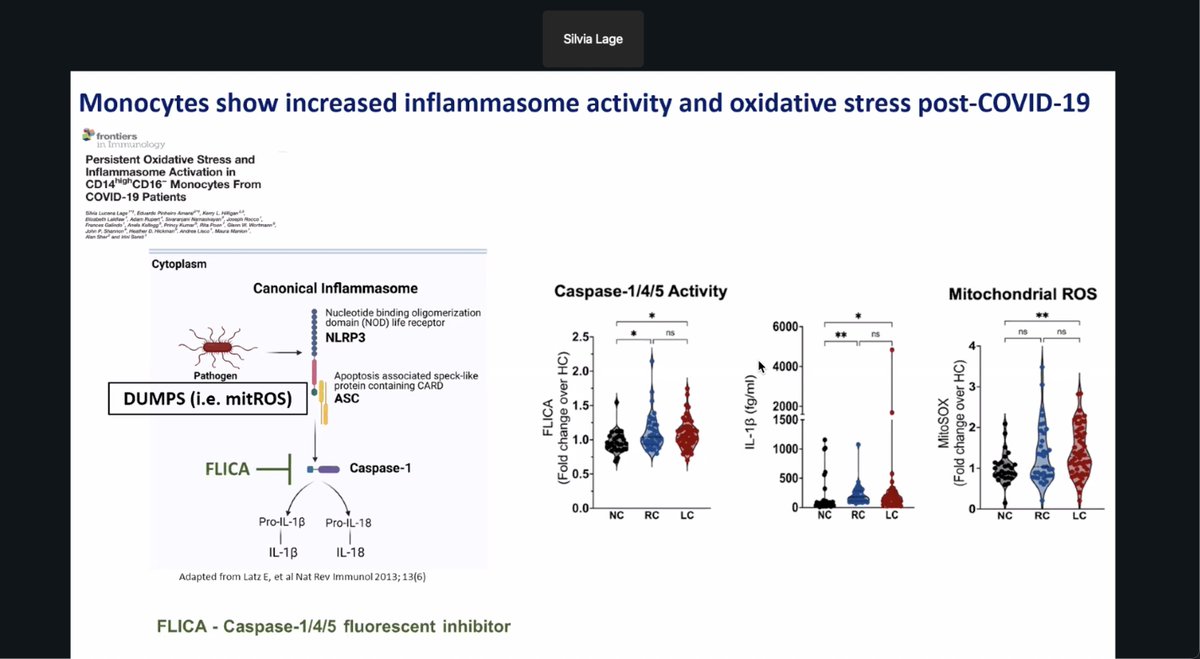
97/ Researchers found monocytes from long COVID patients show elevated caspase-1 activity and mitochondrial ROS, suggesting persistent inflammasome activation and oxidative stress may underlie lingering symptoms.
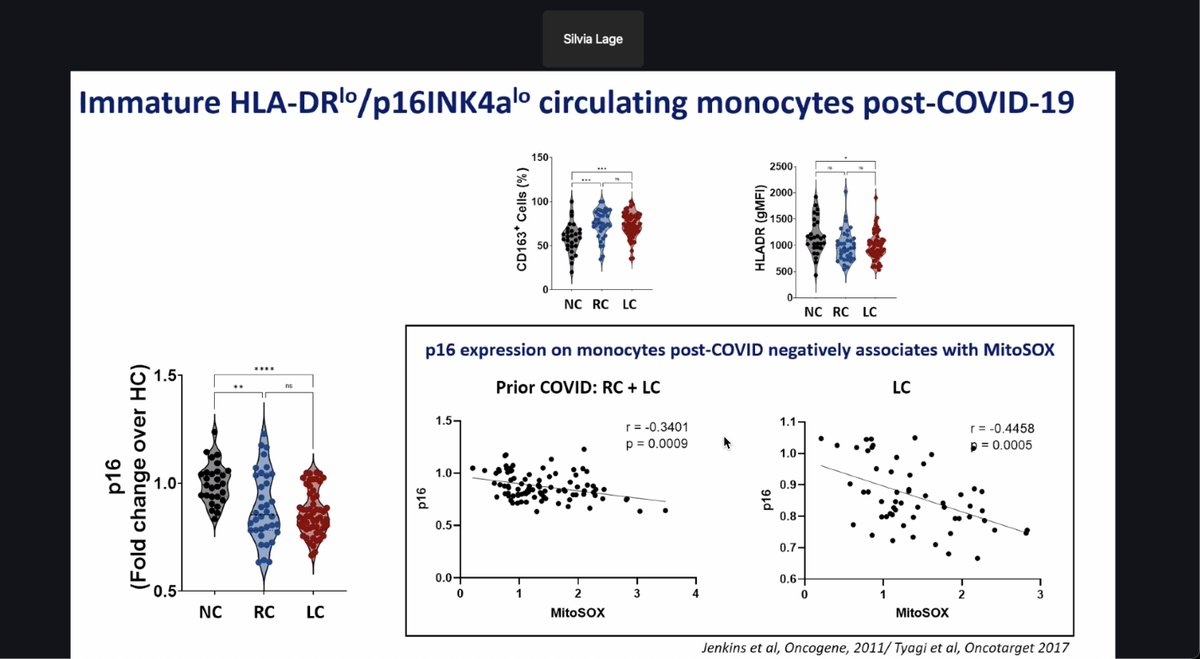
98/ Researchers found that monocytes in long COVID patients show lower p16 and HLA-DR expression, with p16 inversely correlated to oxidative stress, suggesting a shift toward immature, dysfunctional immune cells.
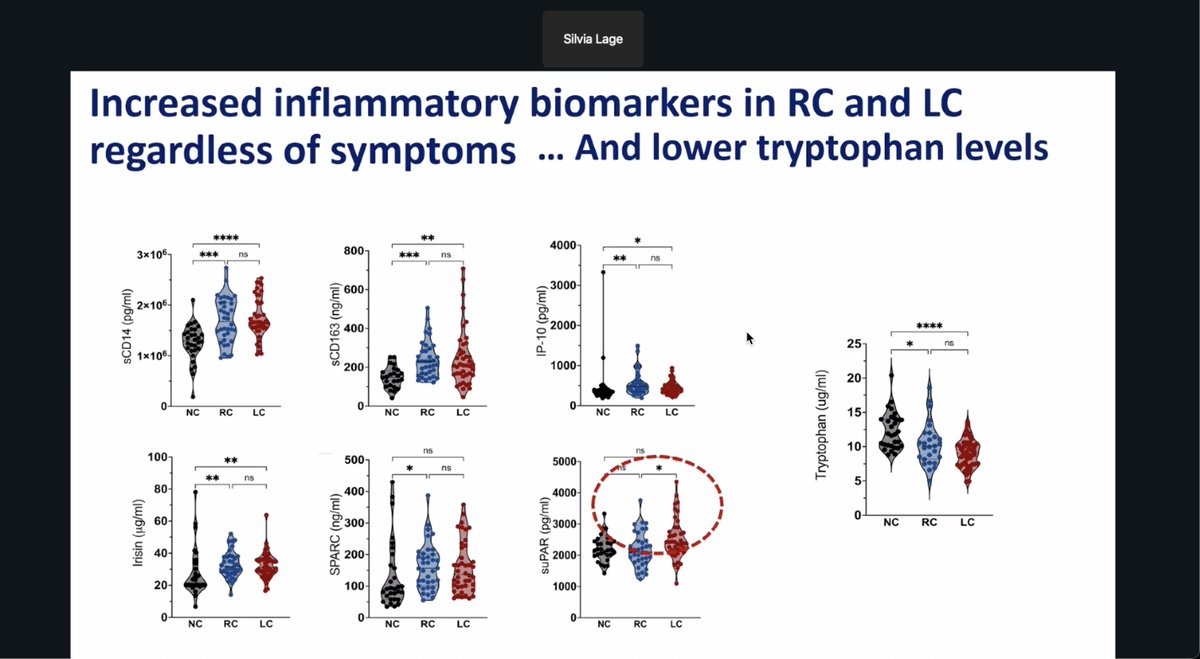
99/ Researchers report that both recovered and long COVID patients show elevated inflammatory biomarkers and reduced tryptophan levels compared to healthy controls, suggesting persistent immune activation regardless of ongoing symptoms.
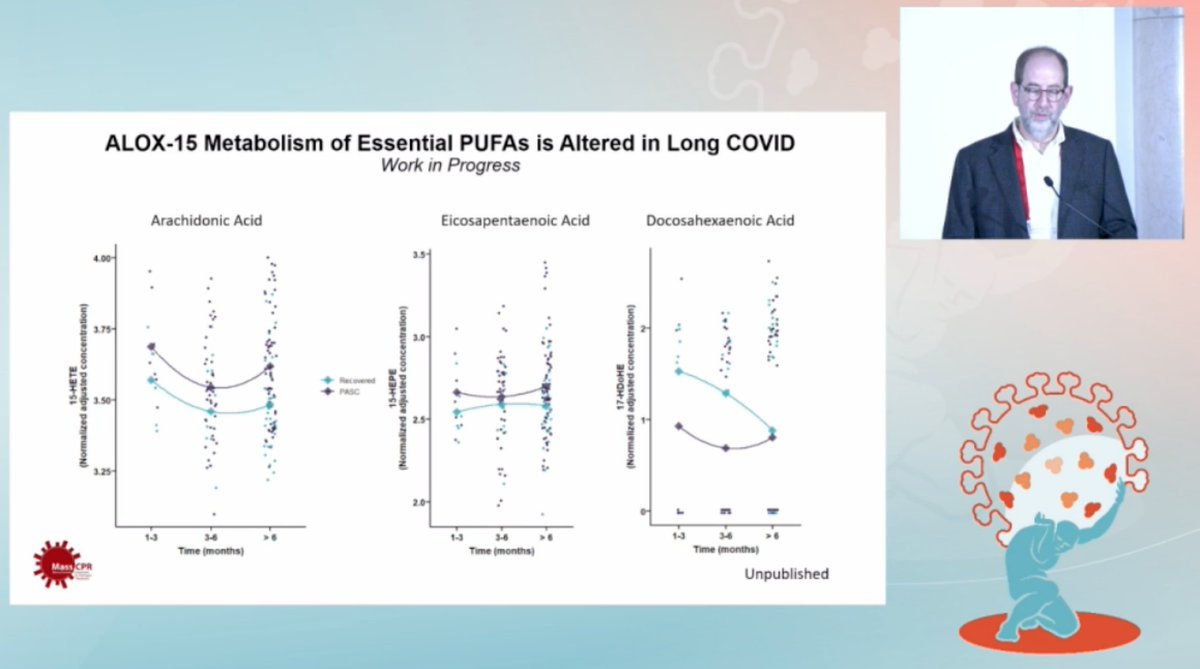
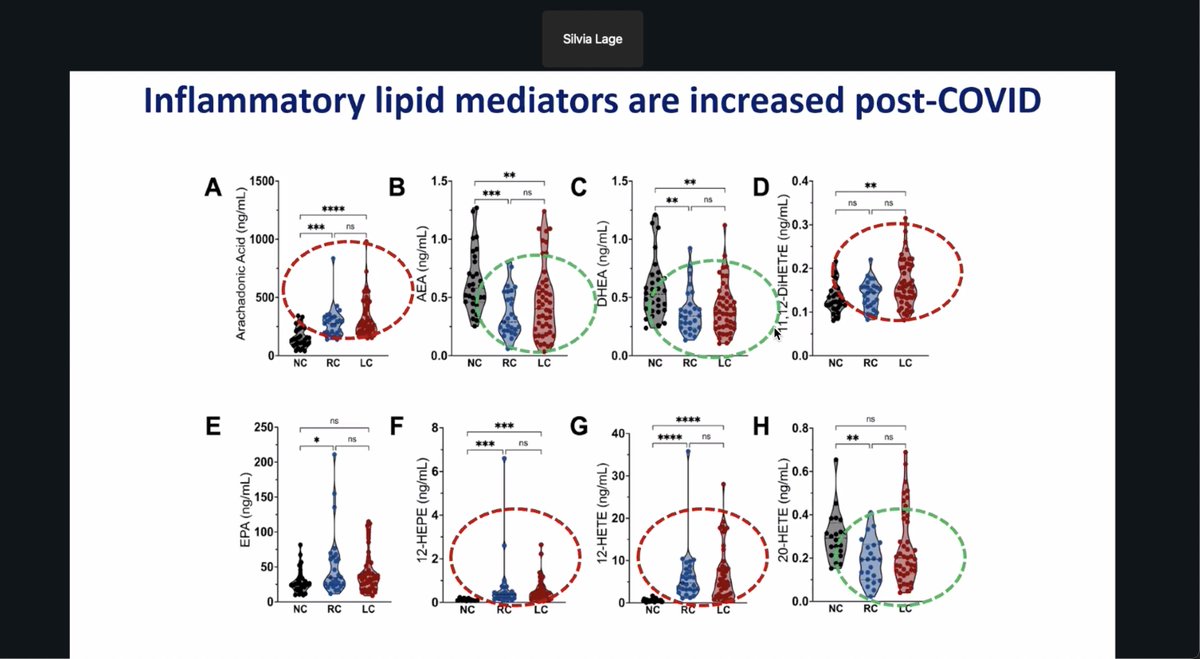
100/ Researchers found elevated inflammatory lipid mediators in recovered and long COVID patients, including arachidonic acid, 12-HETE, and 17,18-DiHETE, suggesting persistent post-infection immune signaling distinct from healthy controls.
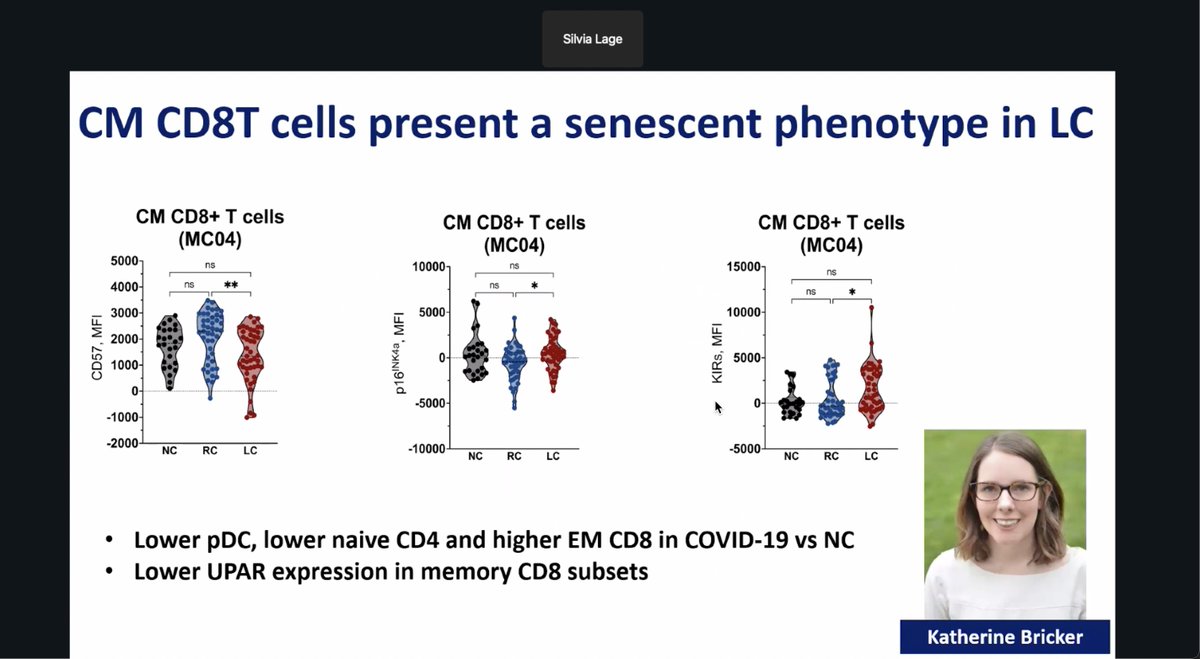
101/ Researchers show CM CD8+ T cells from long COVID patients display a senescent phenotype with higher CD57 and KIRs, and lower p16, indicating altered memory T cell aging and immune regulation post-infection.
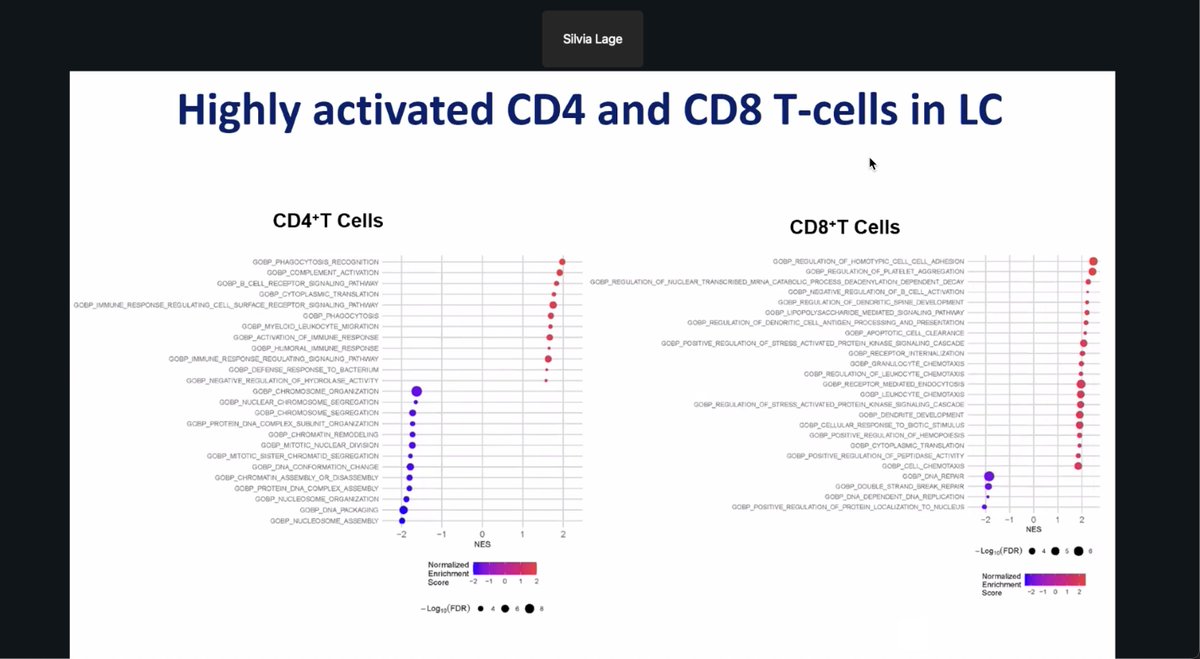
102/ Researchers find CD4 and CD8 T cells in long COVID patients are highly activated, showing enriched pathways for immune signaling, stress responses, and cell adhesion, suggesting persistent immune dysregulation.
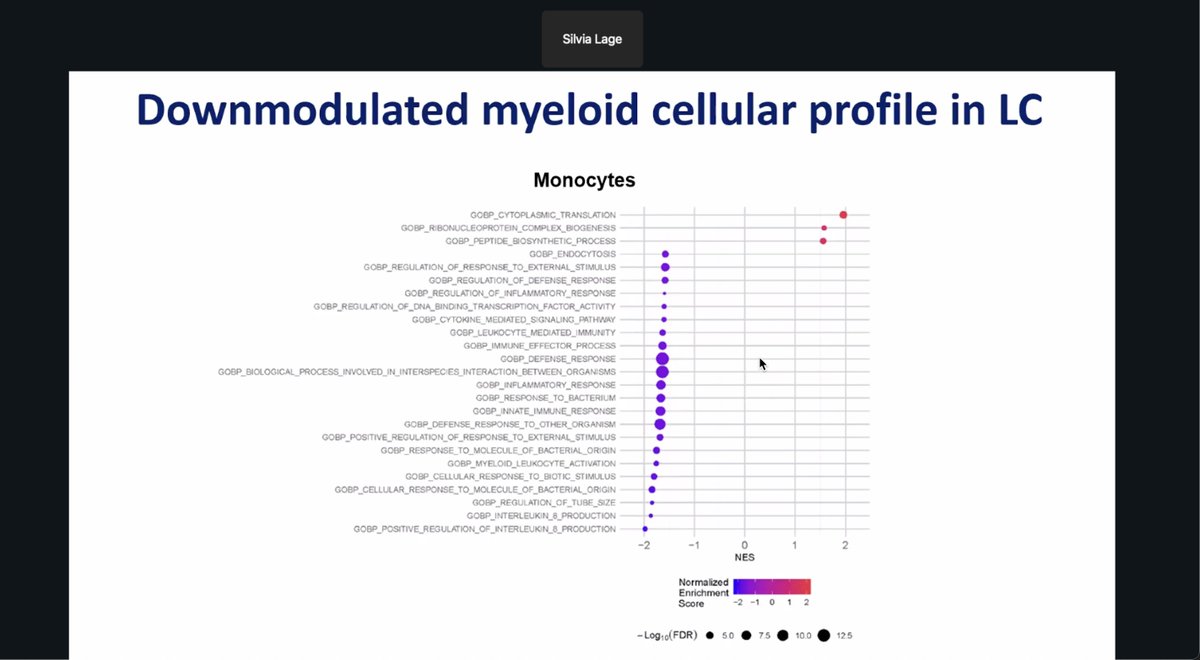
103/ Researchers report that long COVID patients show a downmodulated myeloid profile, with monocytes displaying suppressed pathways in inflammatory signaling, immune defense, and cytokine response.
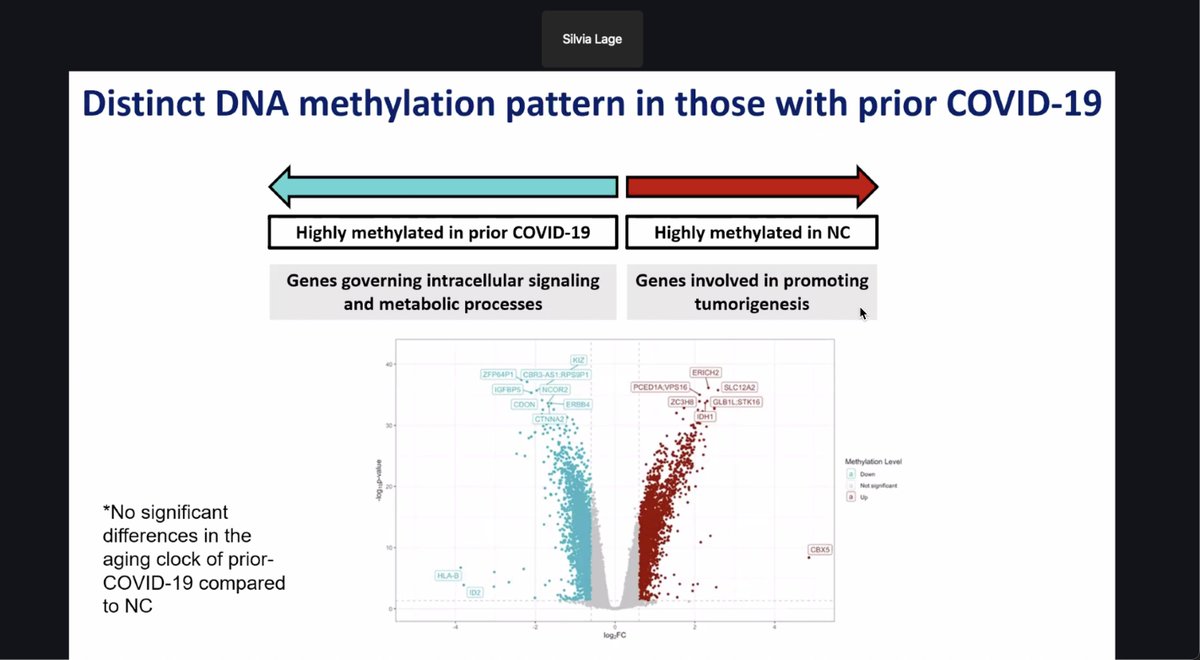
104/ Individuals with prior COVID-19 show distinct DNA methylation, with changes in genes tied to signaling and metabolism, while controls show higher methylation in tumor-related genes. No aging clock shift was observed.
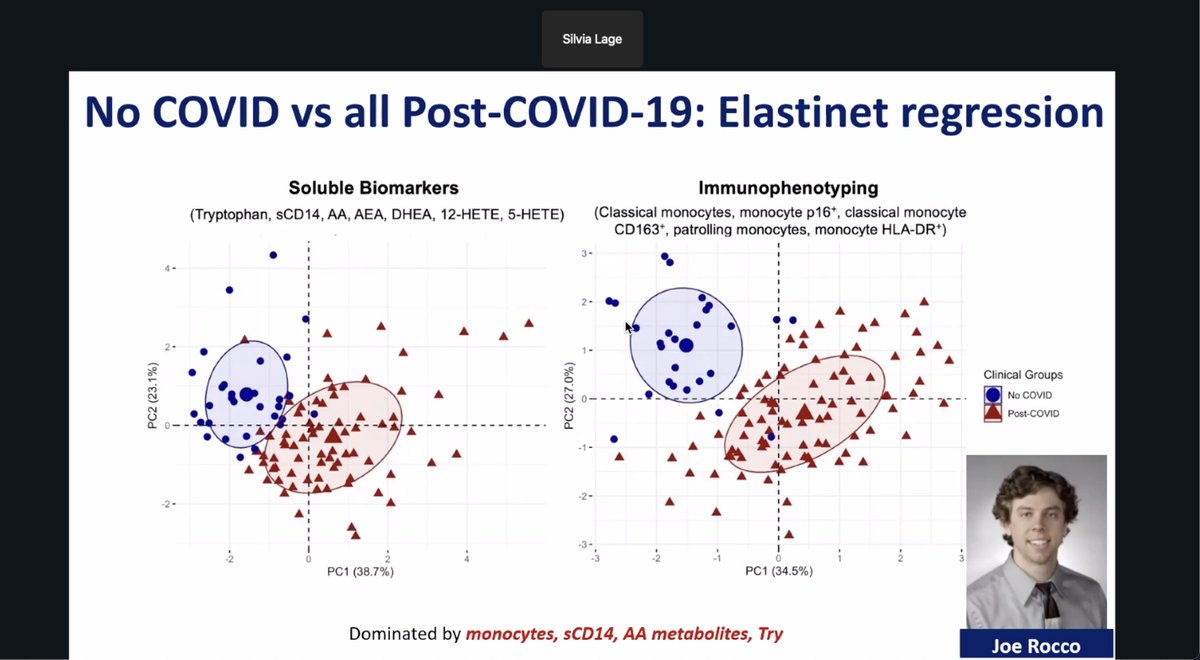
105/ Used elastic net regression to distinguish post-COVID patients from controls based on biomarkers and immune cell profiles. Monocytes, sCD14, AA metabolites, and tryptophan drove the separation across all post-COVID individuals.
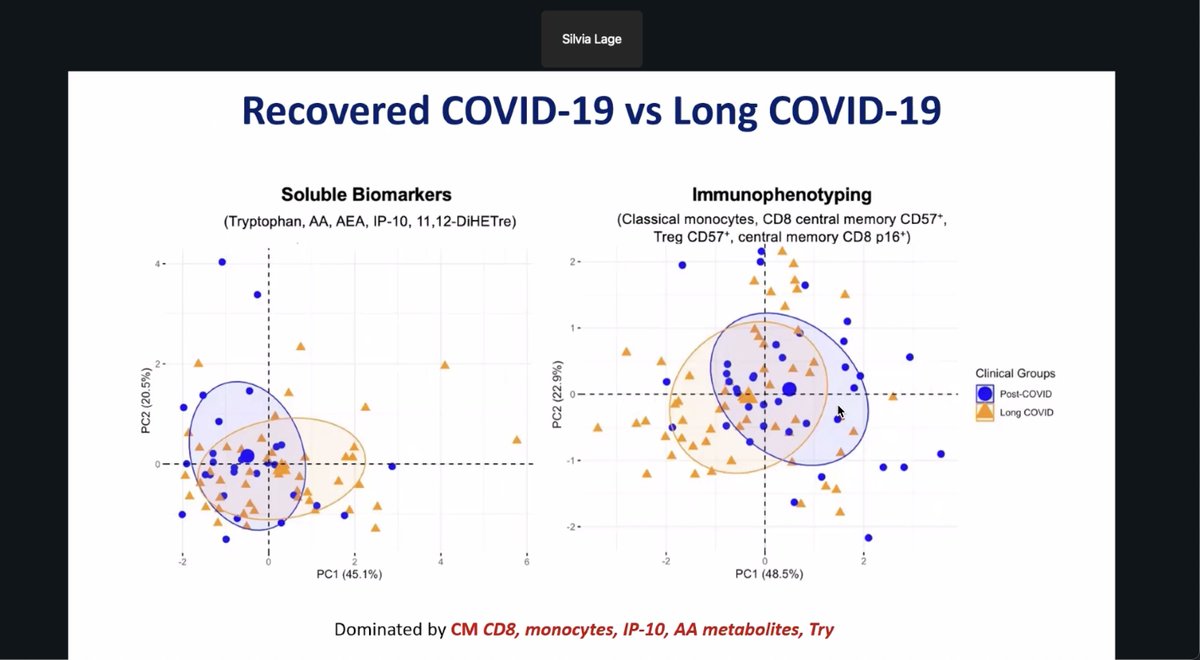
106/ Researchers found that long COVID patients and recovered individuals show partial separation based on immune and metabolic markers. Key drivers include CD8 memory T cells, monocytes, IP-10, and altered lipid and tryptophan metabolism.
107/ San Francisco researchers analyzed 435+ autopsy cases and found most sudden cardiac deaths were due to arrhythmic cardiac causes (n=229), with fewer linked to non-cardiac (n=153) or non-arrhythmic cardiac (n=13) origins.
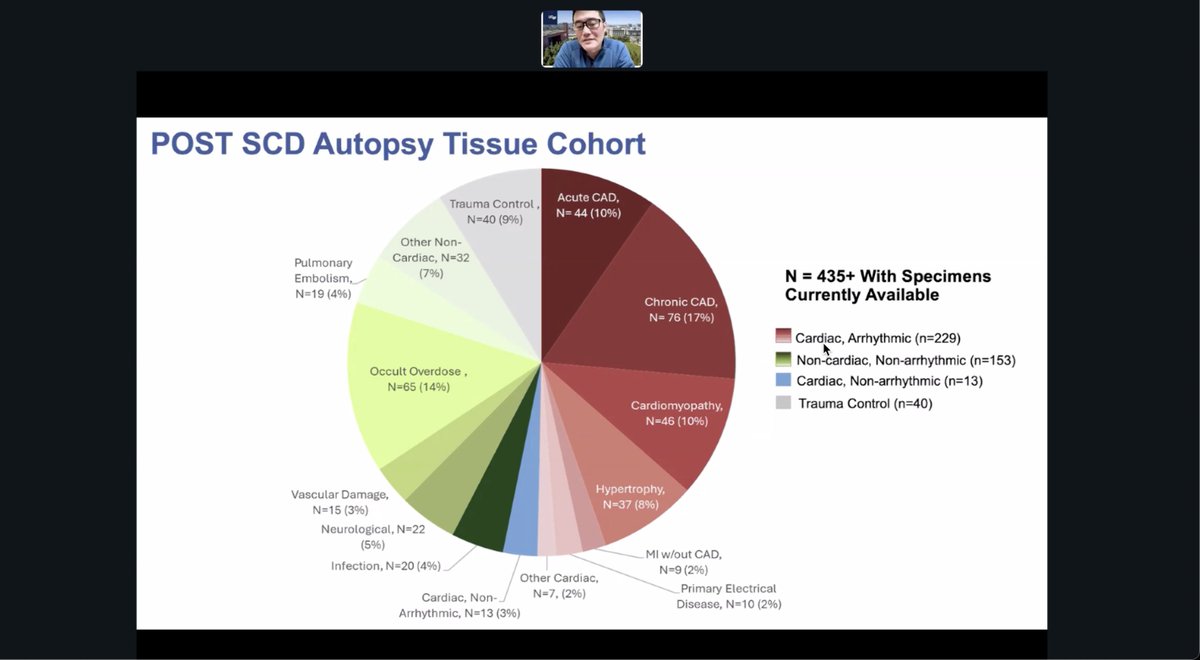
108/ Researchers in the COVID POST SCD study will analyze tissues from sudden death cases to search for viral persistence, immune dysregulation, and metabolic dysfunction as possible drivers of Long COVID.

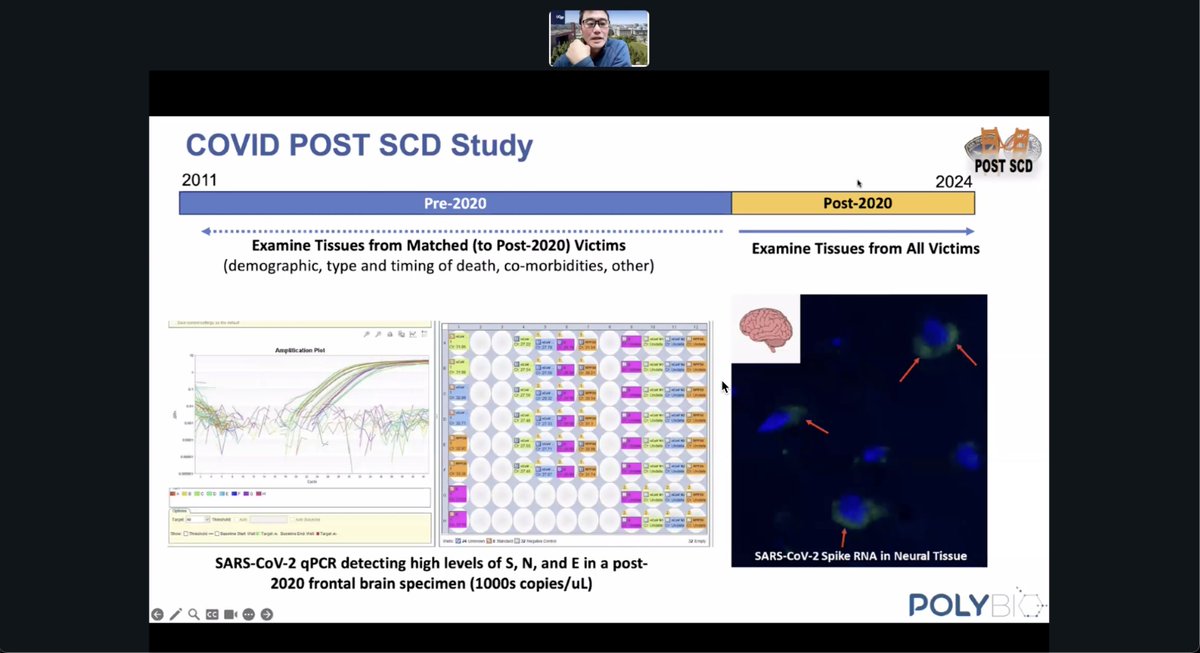
109/ In pre-2020 autopsy samples, researchers found high levels of HIV-1 and EBV RNA in brain and colon tissue, suggesting that latent viral activity in tissues is detectable and may serve as a reference for post-COVID comparisons.

110/ In a post-2020 brain sample, researchers detected high levels of SARS-CoV-2 S, N, and E gene RNA—thousands of copies per microliter—supporting evidence of viral persistence in neural tissue after COVID-19.
111/ Alzheimer’s patients with CD83-positive microglia show elevated IgG4 against HCMV proteins in CSF, pointing to a potential link between chronic viral exposure and neuroimmune activation.
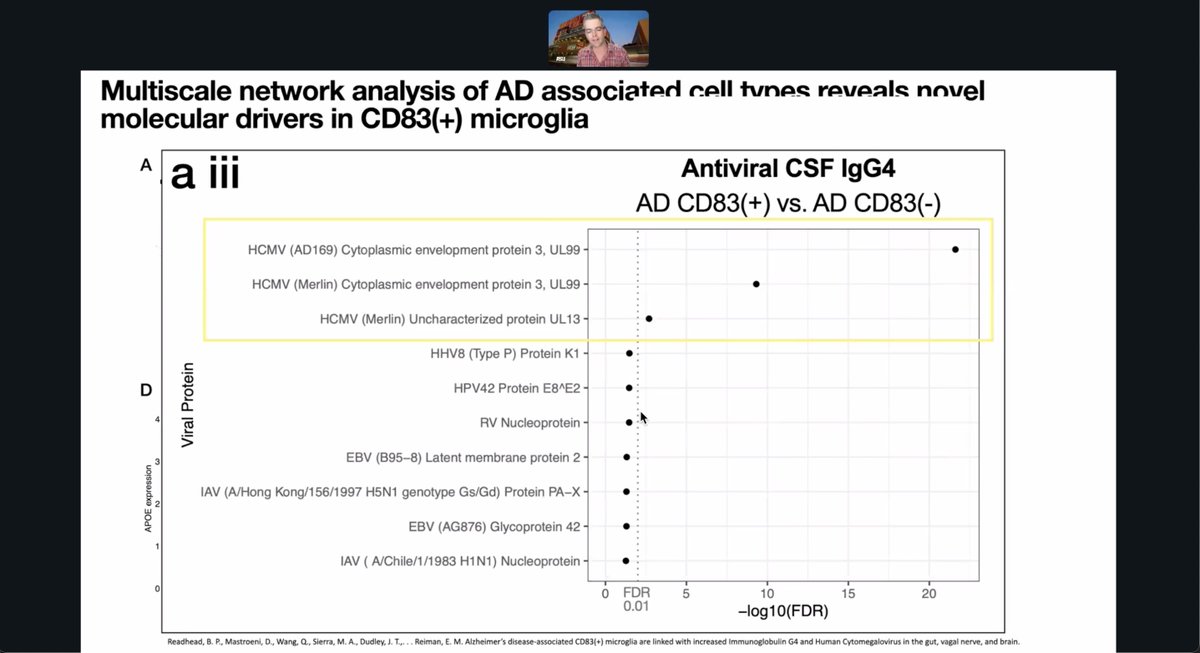
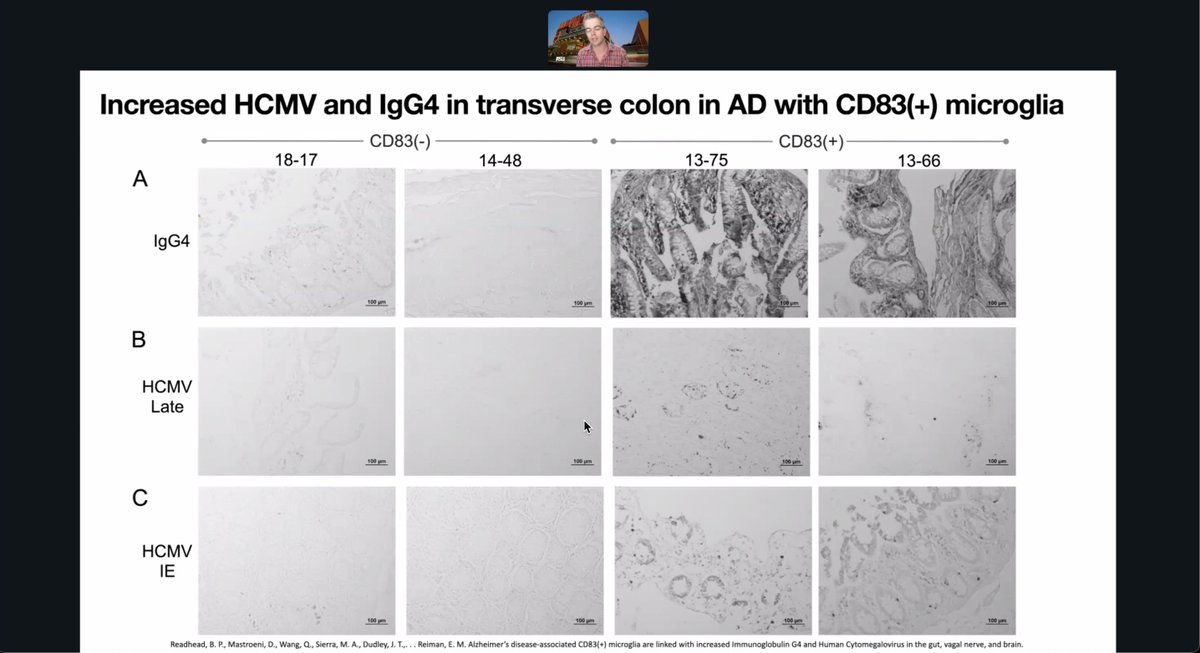
112/ Alzheimer’s patients with CD83-positive microglia have higher HCMV and IgG4 in the colon, linking viral reactivation and immune changes in gut–brain interactions.
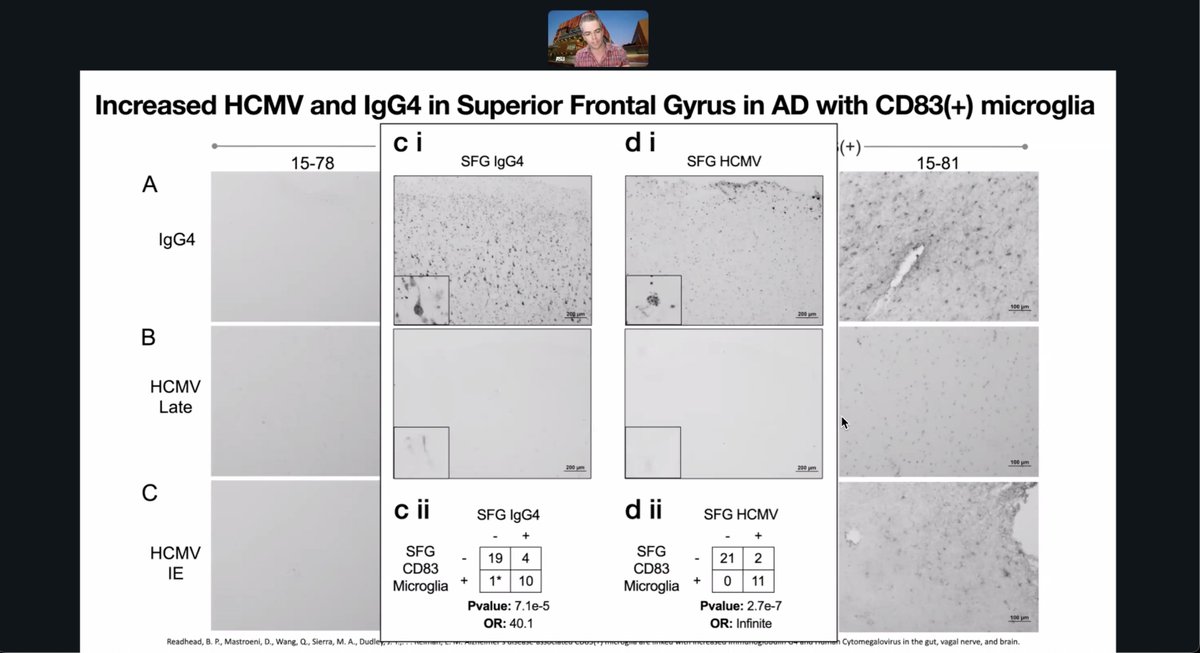
113/ Alzheimer’s brains with CD83-positive microglia show significantly higher HCMV and IgG4 in the superior frontal gyrus, suggesting localized viral reactivation and immune activation in neuroinflammatory disease.
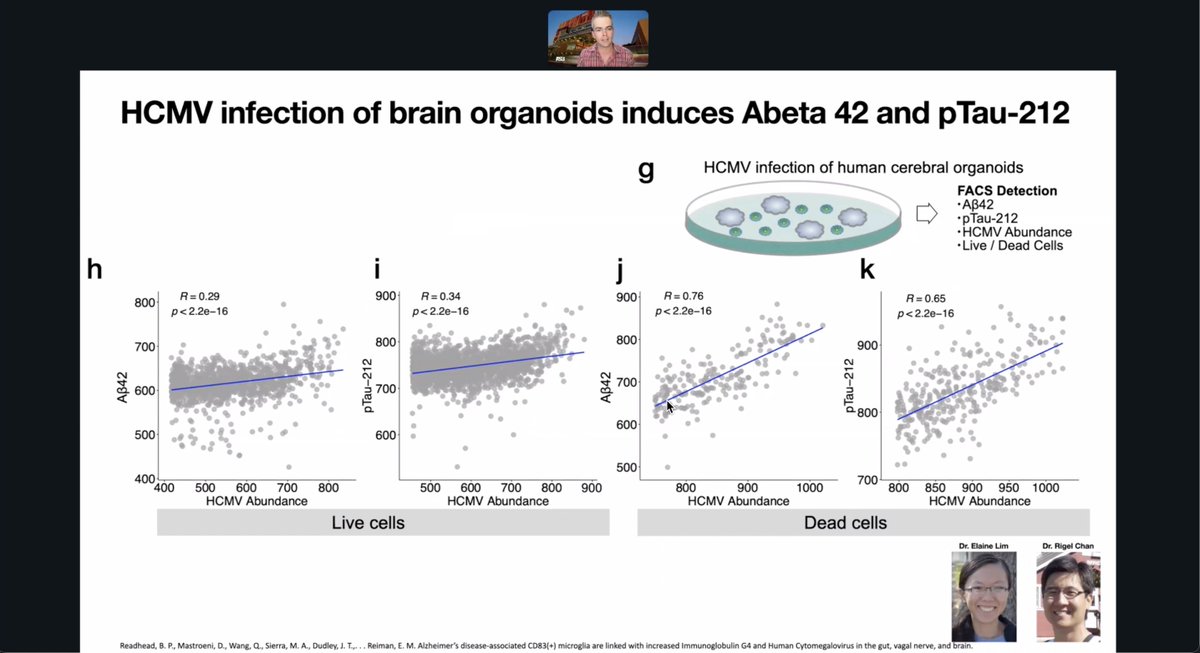
114/ HCMV infection of human brain organoids increases Abeta42 and pTau-212, especially in dead cells, linking viral burden to key Alzheimer’s-related pathologies in vitro.
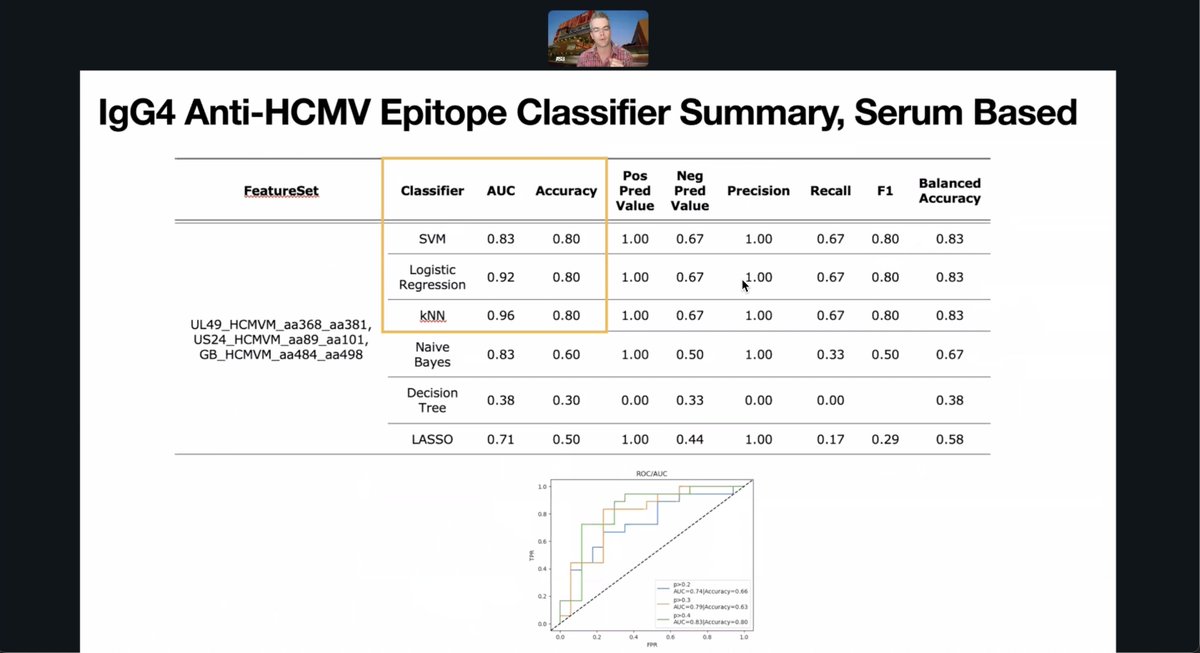
115/ Researchers used serum IgG4 responses to HCMV epitopes to classify Alzheimer’s-related immune profiles. The k-nearest neighbors model showed the highest AUC (0.96) and precision, indicating strong diagnostic potential.
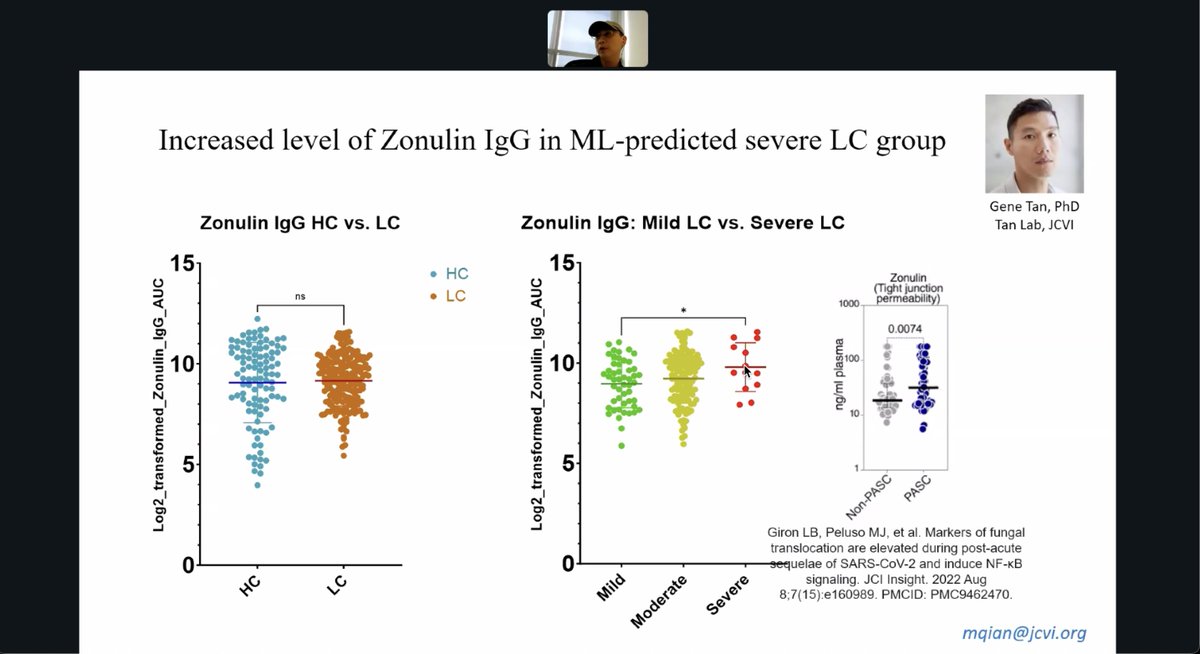
116/ JCVI researchers found higher Zonulin IgG in patients with machine-learning-predicted severe long COVID. Among 3 LC subgroups, only the severe group showed a significant increase, linking gut permeability to symptom severity.
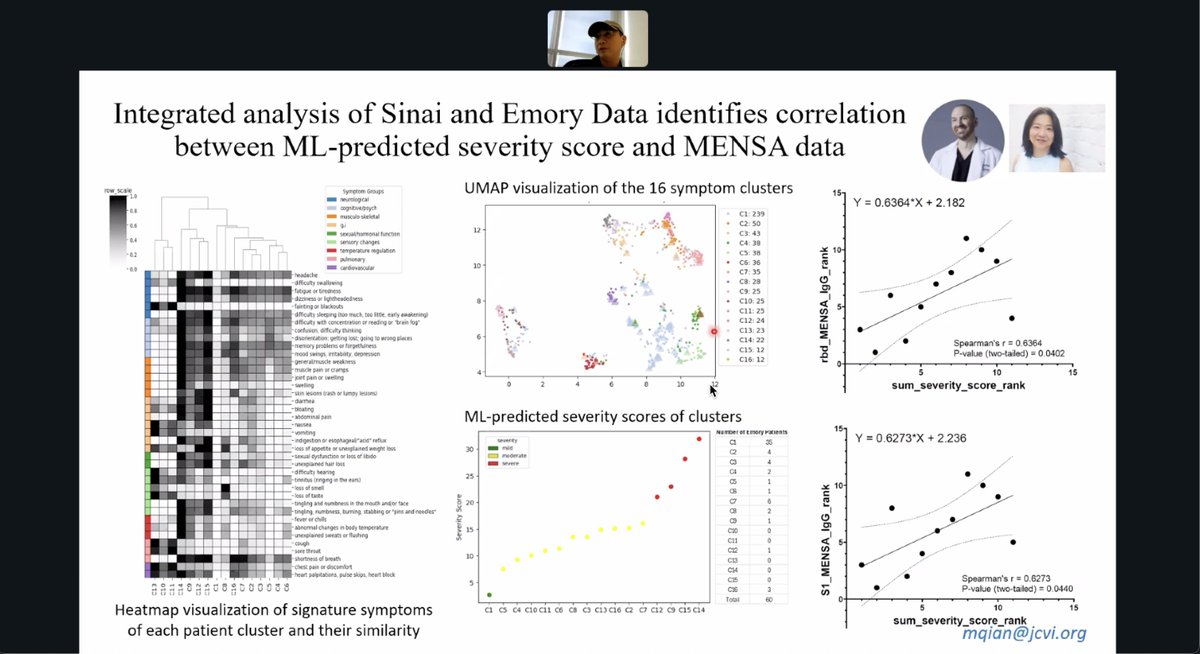
117/ Mount Sinai and Emory researchers found that machine-learning severity scores for long COVID symptom clusters strongly correlate with MENSA antibody data, suggesting immune response profiles track with symptom burden.
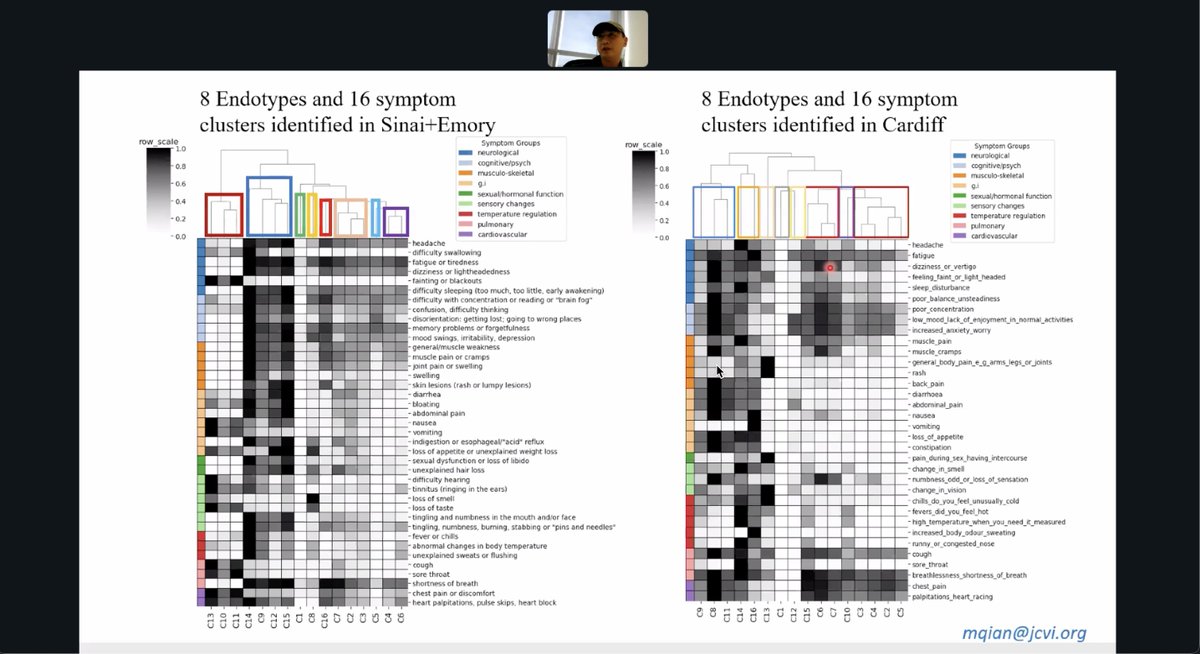
118/ Independently identified 8 biological endotypes and 16 symptom clusters in long COVID, showing convergent patterns of symptom biology across international cohorts.
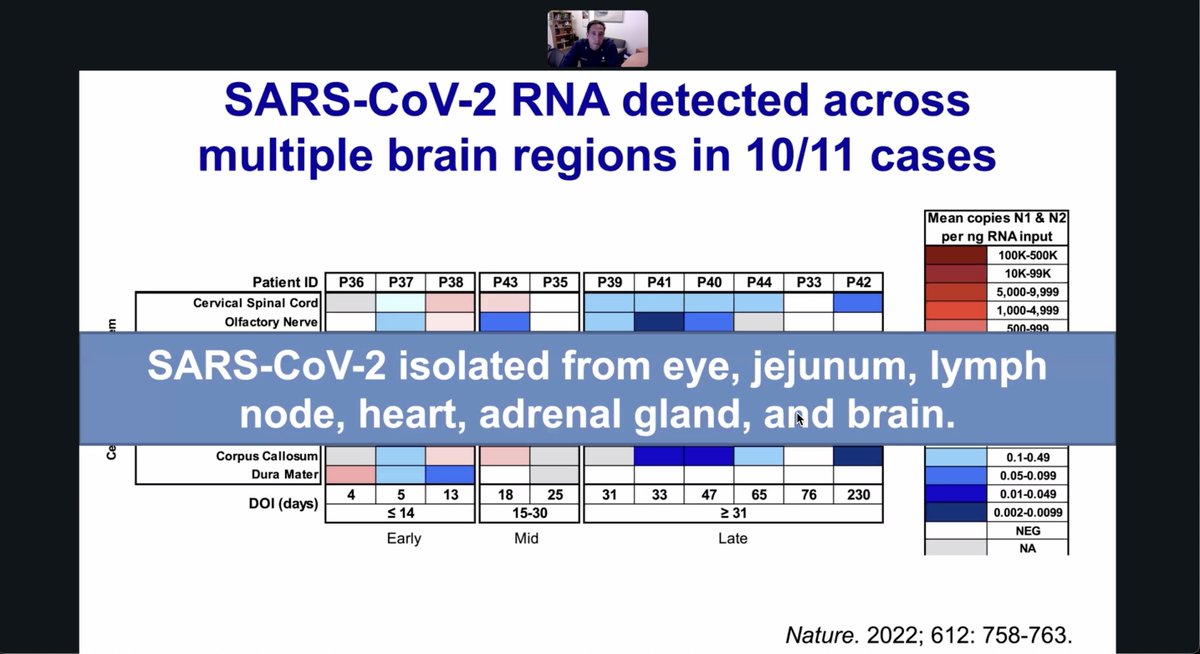
119/ NIH researchers found SARS-CoV-2 RNA in multiple brain regions in 10 of 11 autopsies and isolated virus from the eye, gut, lymph nodes, heart, adrenal gland, and brain, suggesting widespread viral persistence post-infection.
120/ Researchers propose a tissue biopsy trial to test if SARS-CoV-2 RNA or protein, known to persist for months, is linked to long COVID, using safe biopsies to rigorously explore this relationship.

121/ A pilot study of 6 long COVID patients and 6 controls includes exams, lab tests, imaging, and tissue sampling to investigate viral persistence using sequencing and microscopy.

122/ To participate in the Long COVID Tissue Procurement Study, contact Angelique Gavin at angelique.gavin@nih.gov or call (301) 402-0880.

123/ That's All Folks!
• • •
Missing some Tweet in this thread? You can try to
force a refresh