Here's the latest variant picture for the United States, to early May.
The LP.8.1.* variant has peaked and fell back to 52%.
The presumed next challengers are growing – XDV.* (led by NB.1.8.1) to 9% and XFG.* to 8%.
#COVID19 #USA #LP_8_1 #XFG #XDV #NB_1_8_1
🧵
The LP.8.1.* variant has peaked and fell back to 52%.
The presumed next challengers are growing – XDV.* (led by NB.1.8.1) to 9% and XFG.* to 8%.
#COVID19 #USA #LP_8_1 #XFG #XDV #NB_1_8_1
🧵


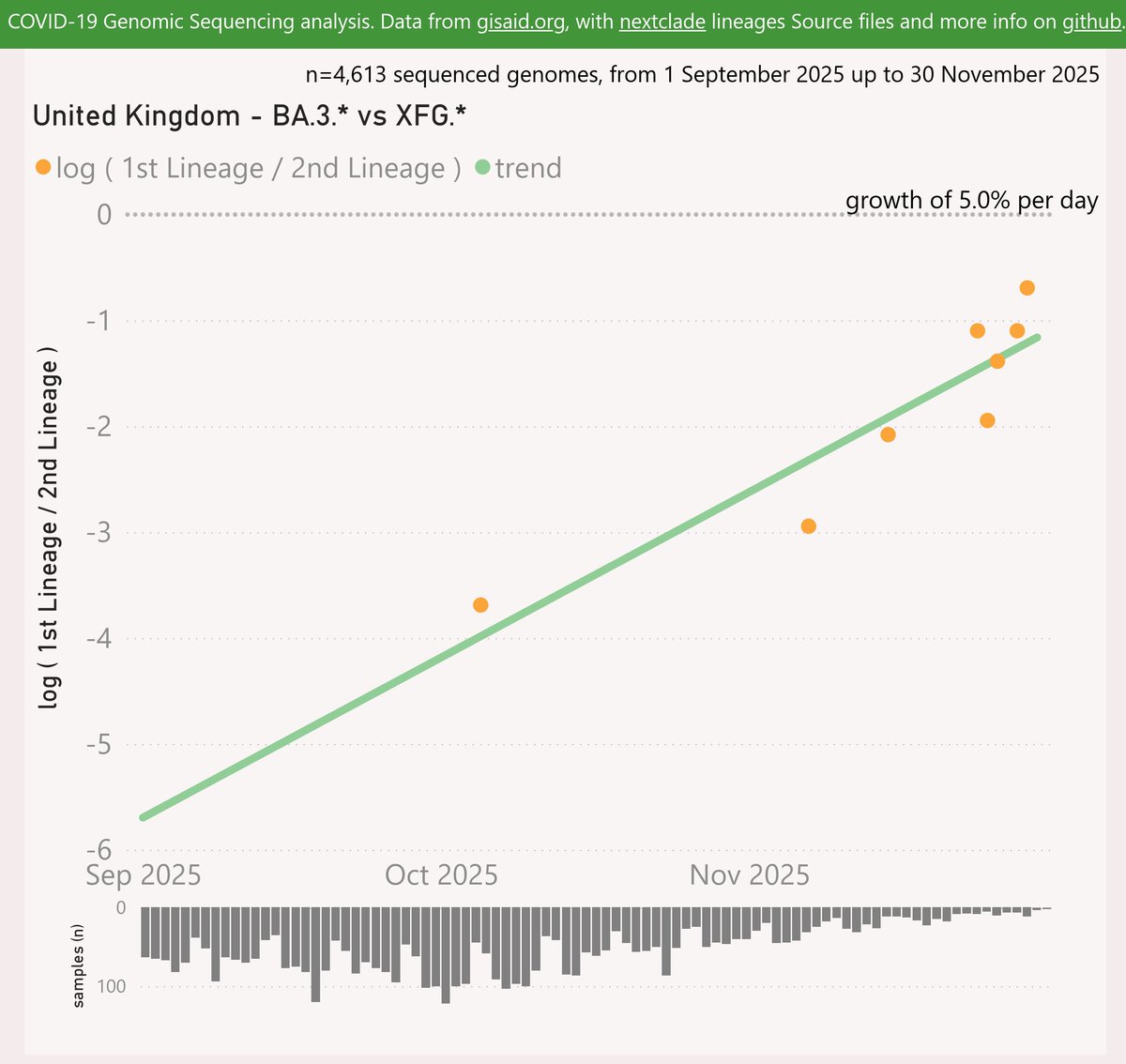
For the US, the XFG.* variant shows a strong but slightly slowing growth advantage of 5.2% per day (36% per week) over LP.8.1.*, which now predicts a crossover in early June.
🧵
🧵

For the US, the XDV.* variant (led by NB.1.8.1) shows a healthy growth advantage of 4.8% per day (34% per week) over LP.8.1.*, with a possible crossover in June.
🧵
🧵

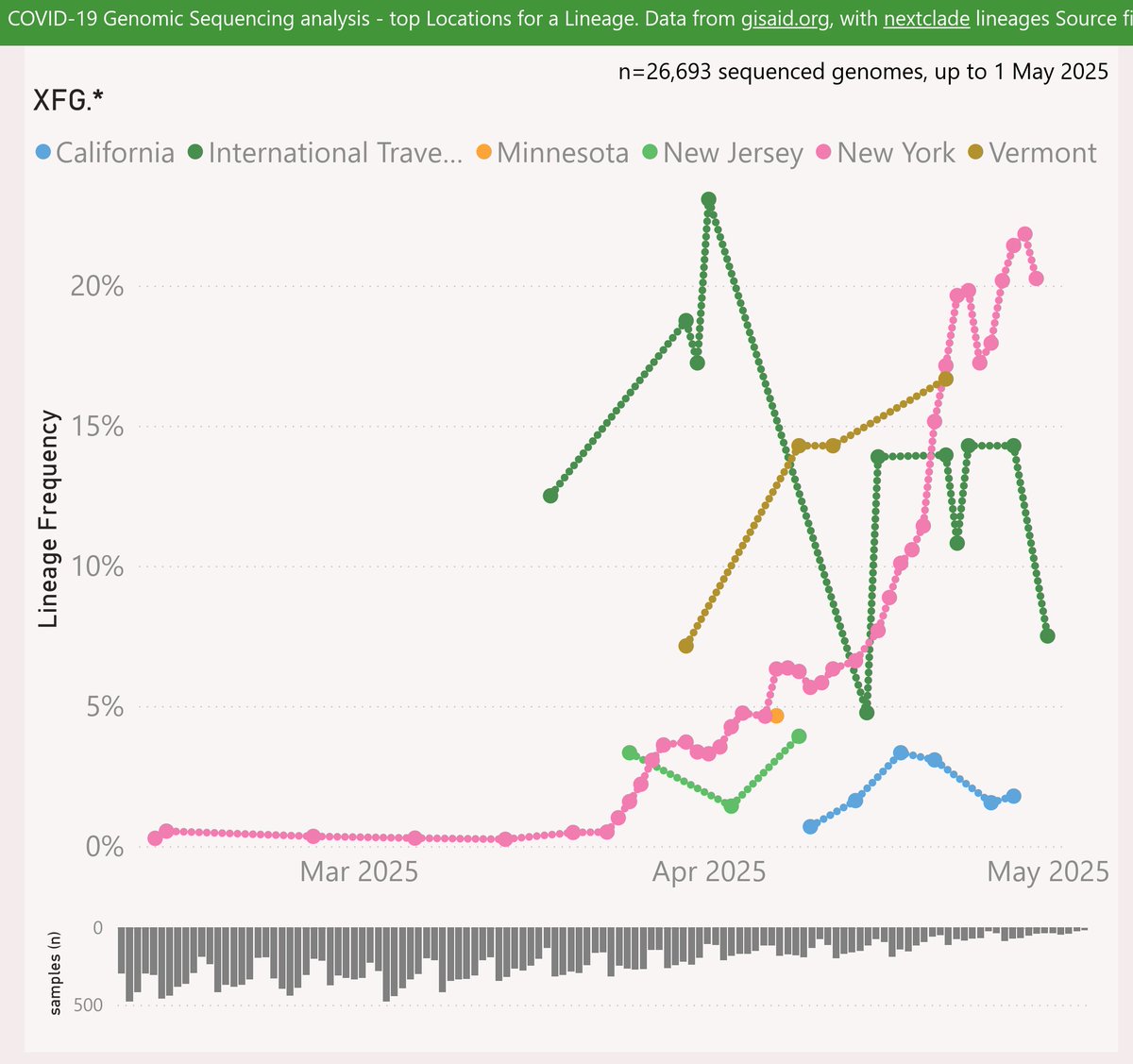
The XFG.* variant has mainly been reported from New York state, rising to 22% frequency. It was very common among the International Traveller samples in early April, but has been less common lately.
🧵
🧵
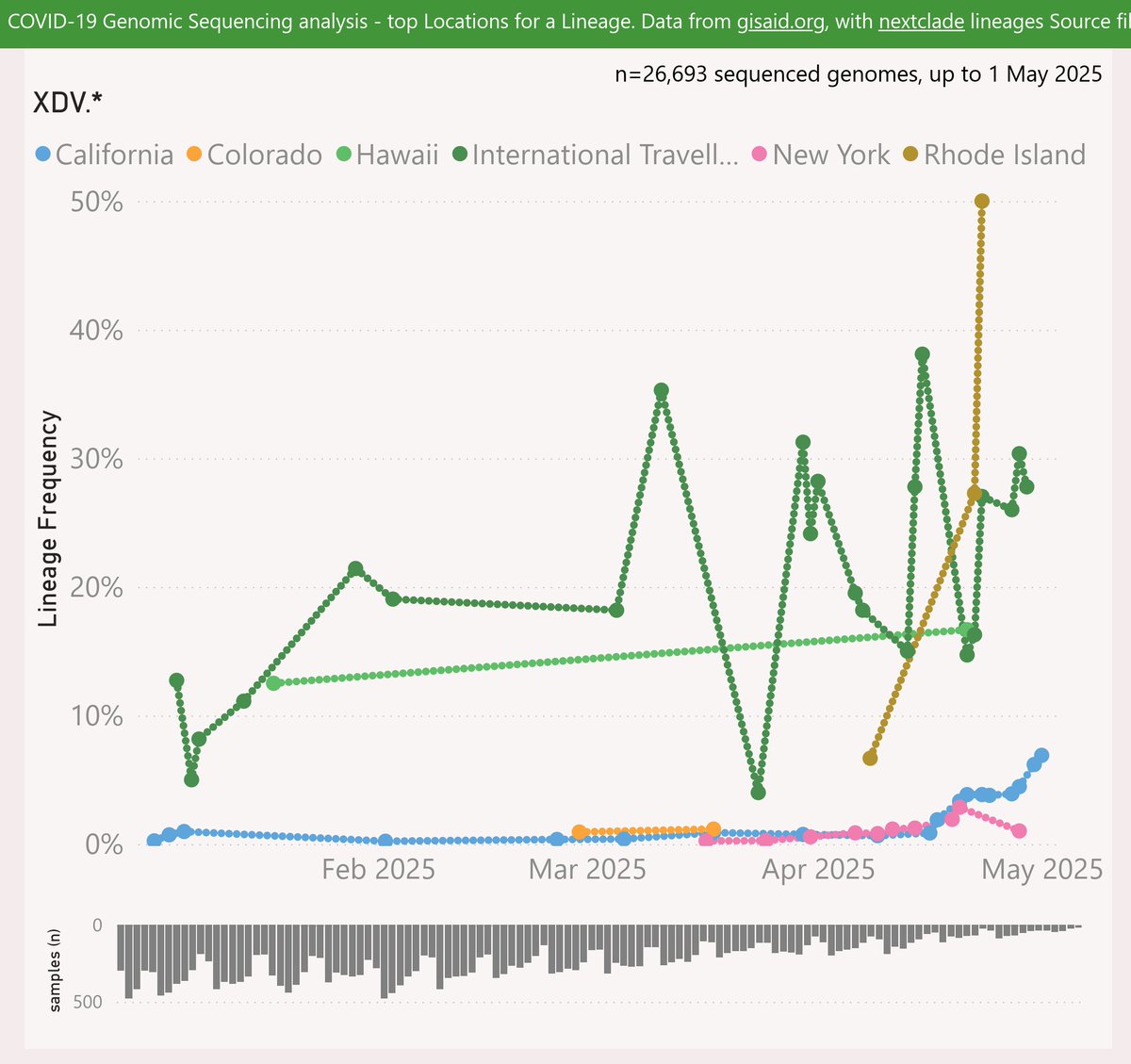
The XDV.* variant (led by NB.1.8.1) has mainly been reported among the International Traveller samples, at around 20-40% frequency. It rose to 50% in Rhode Island recently, but samples sizes from there are very thin.
🧵
🧵
International Traveller samples represent a significant population. Looking at the last 8 weeks, their volume ranks them 12th among the US states. As international arrivals are around 10-12M per month, that seems roughly proportionate.
🧵
🧵

Another factor is the profile of those people. The typical subject of a PCR test is now someone in a health care or aged care setting, so tending older. International travellers who submit a sample are more likely to be adults, so more representative of the overall population.
🧵
🧵
Recent travellers (who may be unaware they are infectious) are also seem more likely to be in superspreader scenarios eg onward domestic travel, restaurants, events etc.
So considering all of that I prefer to include the International Traveller samples in my US analysis.
🧵
So considering all of that I prefer to include the International Traveller samples in my US analysis.
🧵
• • •
Missing some Tweet in this thread? You can try to
force a refresh