
1/
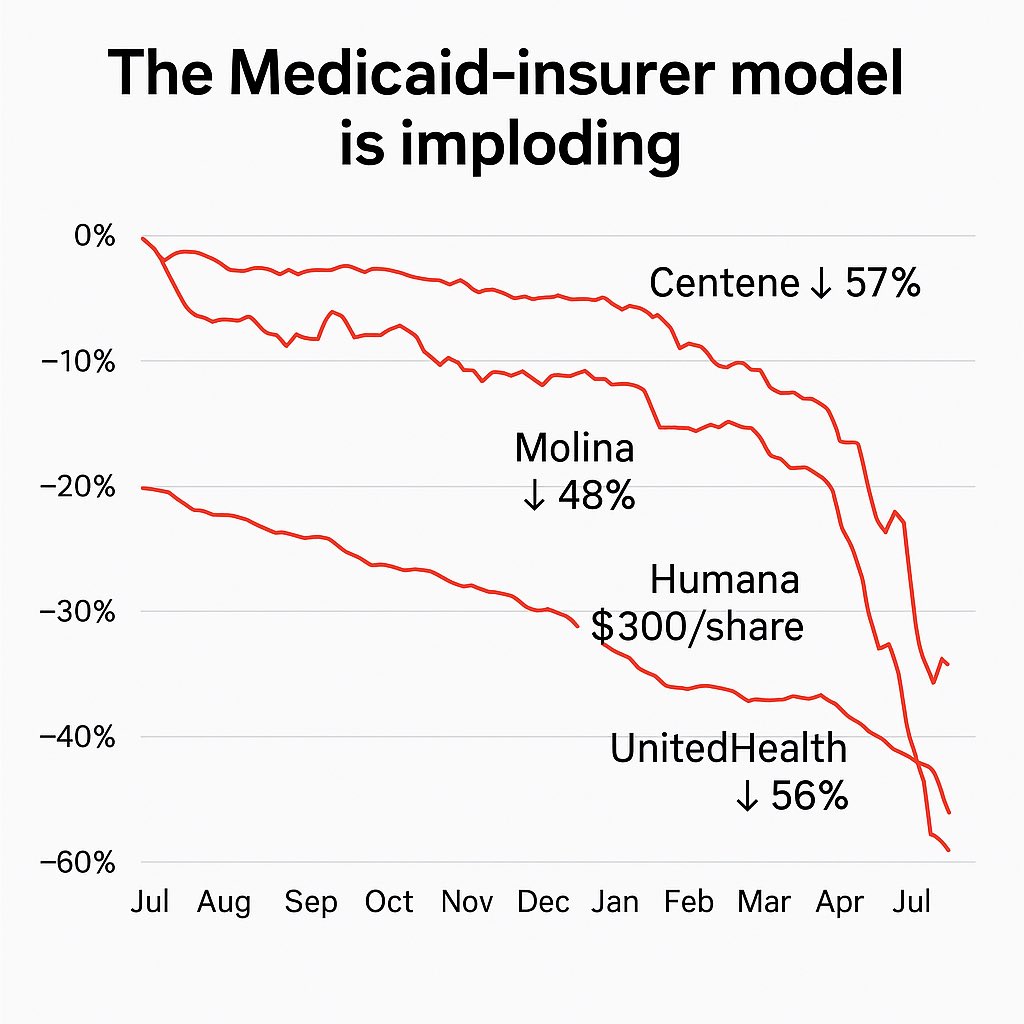
BREAKING: The Medicaid-insurer model is collapsing in real time.
Centene: down 61%
Molina: down 55%
Humana: lost $300/share
UnitedHealth: down 46% YTD and under federal investigation
This isn’t just a sell-off.
It’s the end of the myth.
🧵 Let’s go.
BREAKING: The Medicaid-insurer model is collapsing in real time.
Centene: down 61%
Molina: down 55%
Humana: lost $300/share
UnitedHealth: down 46% YTD and under federal investigation
This isn’t just a sell-off.
It’s the end of the myth.
🧵 Let’s go.
2/
Centene (CNC):
Down from $80 to $28.
That’s a 61% implosion.
This was Medicaid’s golden goose.
Now?
They’re promising “profitability by 2026.”
Translation:
They were never actually profitable without political cover.
Centene (CNC):
Down from $80 to $28.
That’s a 61% implosion.
This was Medicaid’s golden goose.
Now?
They’re promising “profitability by 2026.”
Translation:
They were never actually profitable without political cover.

2.5/
Bookmark this thread.
Follow @DutchRojas if you’re tired of pretending high premiums are normal.
We don’t just explain the collapse.
We built the replacement.
Bookmark this thread.
Follow @DutchRojas if you’re tired of pretending high premiums are normal.
We don’t just explain the collapse.
We built the replacement.
3/
Molina (MOH) is bleeding too.
$365 to $165 in 12 months.
That’s a 55% loss.
This is what happens when you wrap margin games in “value-based care” language.
Investors believed the pitch. Now they’re watching the bottom fall out.
Molina (MOH) is bleeding too.
$365 to $165 in 12 months.
That’s a 55% loss.
This is what happens when you wrap margin games in “value-based care” language.
Investors believed the pitch. Now they’re watching the bottom fall out.

4/
Humana (HUM):
Lost $300/share, more than half its value.
The media called them “innovators.”
Analysts called them “safe.”
I call it what it is:
A house of cards built on Medicare Advantage 💩💩💩💩💩.
Humana (HUM):
Lost $300/share, more than half its value.
The media called them “innovators.”
Analysts called them “safe.”
I call it what it is:
A house of cards built on Medicare Advantage 💩💩💩💩💩.
5/
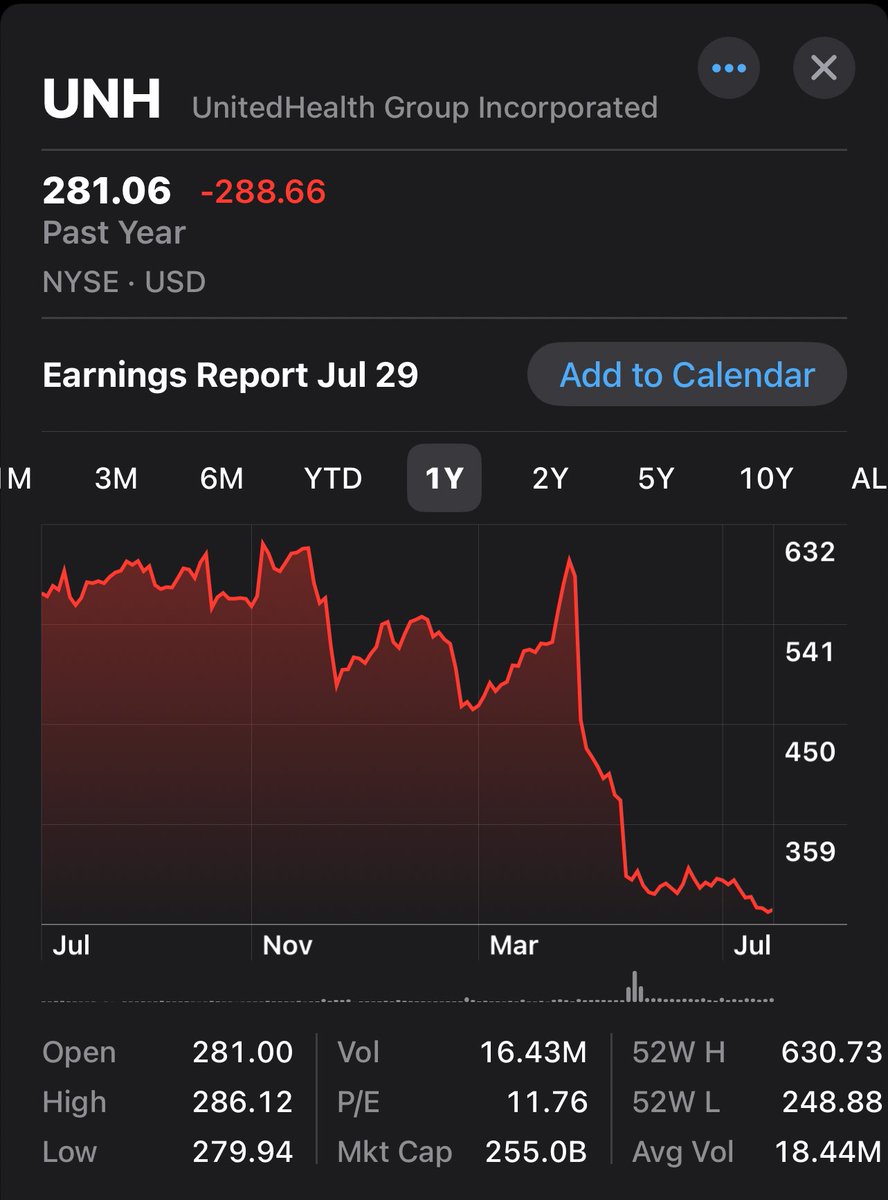
And then there’s UnitedHealth (UNH):
The Death Star.
• $630 → $281
• Down 46% YTD
• DOJ fraud probe (criminal!)
• Accused of leveraging Optum to rig MA billing
Let’s investigate the lobbyists too!
This is institutional failure at its peak.
And then there’s UnitedHealth (UNH):
The Death Star.
• $630 → $281
• Down 46% YTD
• DOJ fraud probe (criminal!)
• Accused of leveraging Optum to rig MA billing
Let’s investigate the lobbyists too!
This is institutional failure at its peak.
6/
Elevance?
Also down 50% from its 2023 peak.
This is a model that was built on lies.
Opaque billing, political dependence, monopoly behavior, fake savings.
Everyone played along, until the music stopped…
Elevance?
Also down 50% from its 2023 peak.
This is a model that was built on lies.
Opaque billing, political dependence, monopoly behavior, fake savings.
Everyone played along, until the music stopped…
7/
Jared Holz at Mizuho put it bluntly:
“This is the worst the healthcare sector has ever traded.”
Healthcare is now the worst-performing S&P sector 3 years running.
But here’s what they won’t say:
The rot isn’t external.
It’s internal.
Jared Holz at Mizuho put it bluntly:
“This is the worst the healthcare sector has ever traded.”
Healthcare is now the worst-performing S&P sector 3 years running.
But here’s what they won’t say:
The rot isn’t external.
It’s internal.
8/
Investors are waking up to this:
• Medicaid profit was political arbitrage
• Medicare Advantage was overbilled performance theater
• Consolidation was never protection for patients, it was camouflage to take in as much cash as possible.
Investors are waking up to this:
• Medicaid profit was political arbitrage
• Medicare Advantage was overbilled performance theater
• Consolidation was never protection for patients, it was camouflage to take in as much cash as possible.
9/
These insurers:
Crushed physician autonomy
Lobbied to block price transparency
Claimed nonprofit halos while hoarding cash
And now they want a bailout?
No chance!
These insurers:
Crushed physician autonomy
Lobbied to block price transparency
Claimed nonprofit halos while hoarding cash
And now they want a bailout?
No chance!
10/
If you’re an independent physician reading this:
You don’t need CMS.
You need leverage.
You need each other.
That’s why I built ReKlaim Health:
A platform to organize, aggregate, and compete, before they rewrite the rules again.
If you’re an independent physician reading this:
You don’t need CMS.
You need leverage.
You need each other.
That’s why I built ReKlaim Health:
A platform to organize, aggregate, and compete, before they rewrite the rules again.
10.5/
Like, follow, and share this with someone still stuck inside the legacy system.
@DutchRojas is where the insiders go when they finally want out.
Like, follow, and share this with someone still stuck inside the legacy system.
@DutchRojas is where the insiders go when they finally want out.
11/
The Medicaid-insurer model was never capitalism.
It was monopoly economics dressed in compliance theater.
Now the veil is off.
And the wreckage you see?
That’s what I’ve been warning you about for a decade.
Now let’s build something better.
The Medicaid-insurer model was never capitalism.
It was monopoly economics dressed in compliance theater.
Now the veil is off.
And the wreckage you see?
That’s what I’ve been warning you about for a decade.
Now let’s build something better.

• • •
Missing some Tweet in this thread? You can try to
force a refresh







