🧵 MMF in 2025: Still the Lymphocyte Whisperer
1️⃣
💊 Mycophenolate mofetil (MMF) remains a backbone immunosuppressant in lupus nephritis, ILD, and more.
But in 2025, its story has evolved — from better combos to smarter uses.
Let’s unpack the latest. 👇
@IhabFathiSulima @drkeithsiau @DrAkhilX #MedTwitter
1️⃣
💊 Mycophenolate mofetil (MMF) remains a backbone immunosuppressant in lupus nephritis, ILD, and more.
But in 2025, its story has evolved — from better combos to smarter uses.
Let’s unpack the latest. 👇
@IhabFathiSulima @drkeithsiau @DrAkhilX #MedTwitter
2️⃣
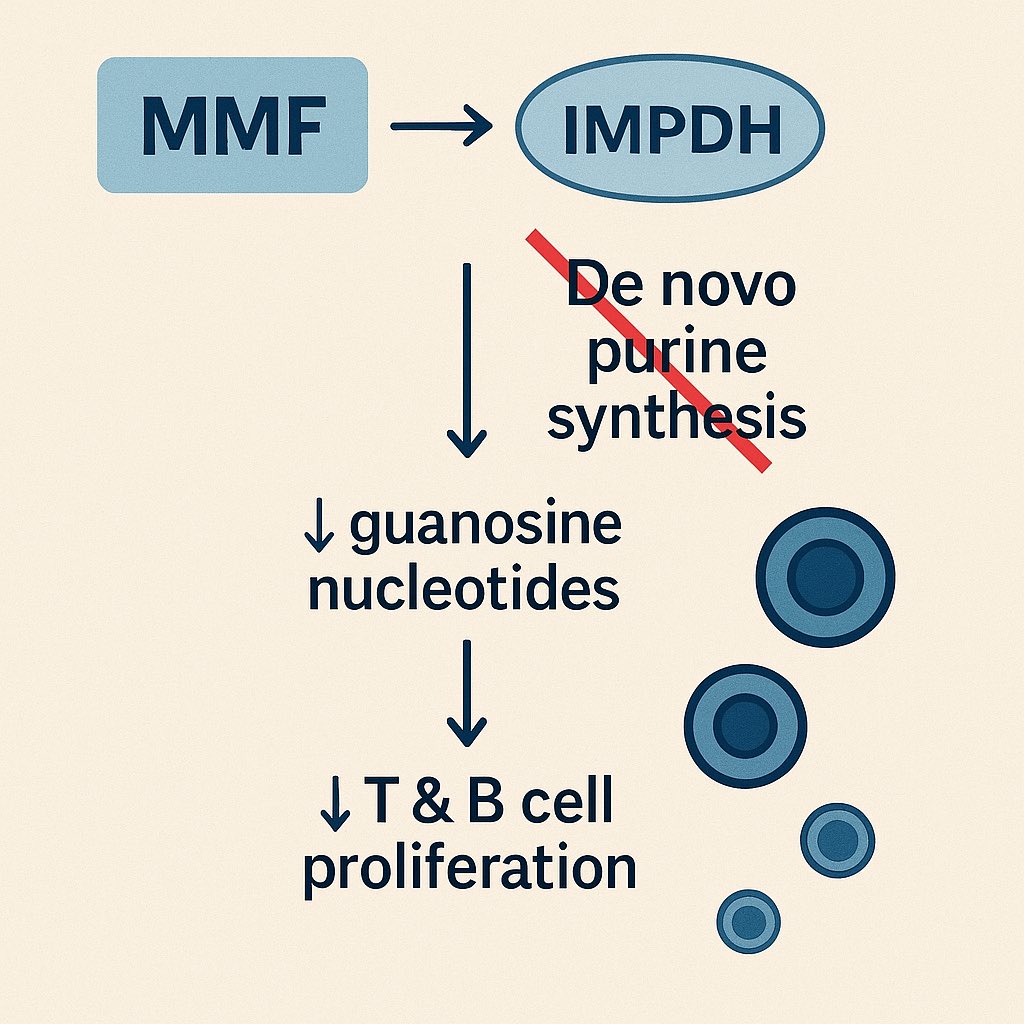
🔬 How it works
MMF blocks inosine monophosphate dehydrogenase (IMPDH) → shuts down guanosine synthesis.
This hits T & B cells hard (they rely on de novo purine synthesis).
🛑 Autoimmunity off, immunity preserved… mostly.
🔬 How it works
MMF blocks inosine monophosphate dehydrogenase (IMPDH) → shuts down guanosine synthesis.
This hits T & B cells hard (they rely on de novo purine synthesis).
🛑 Autoimmunity off, immunity preserved… mostly.
3️⃣
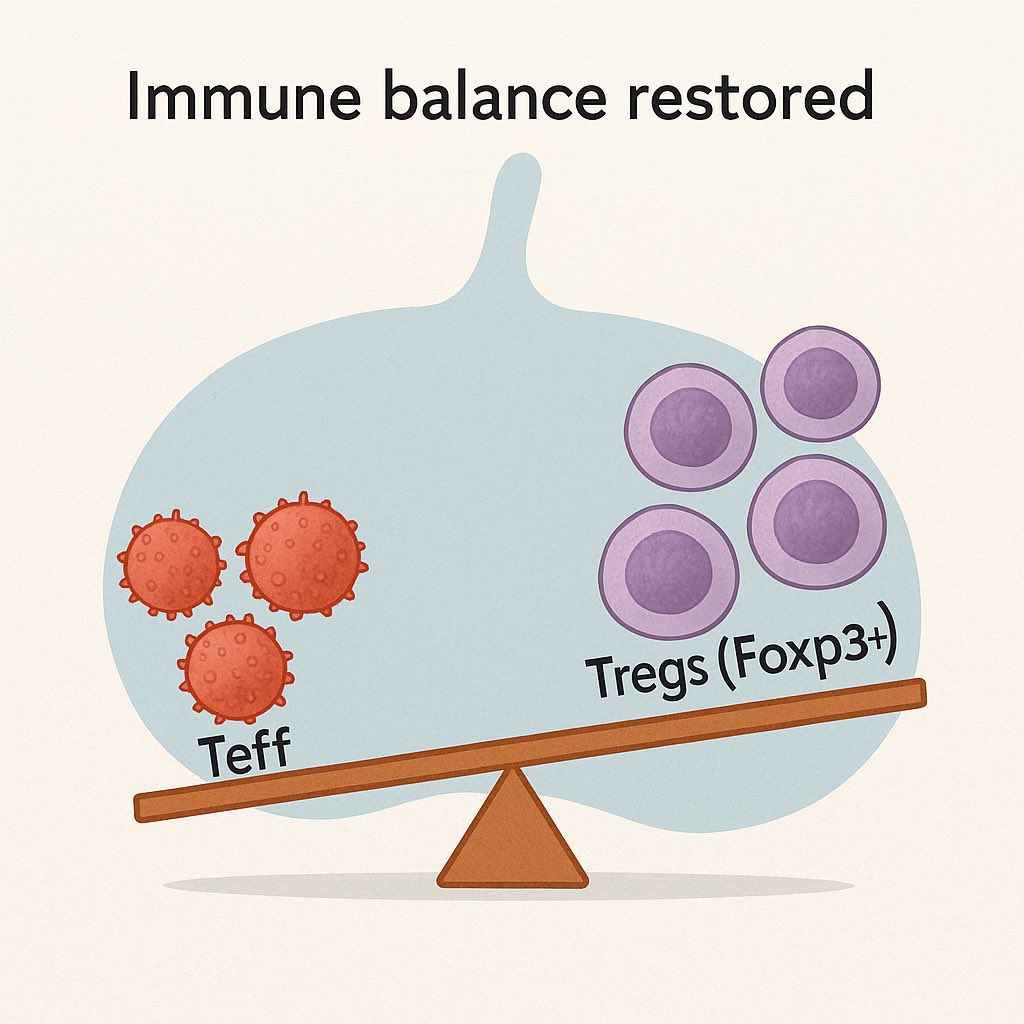
🧠 What’s new mechanistically?
MMF not only suppresses lymphocytes but also tips the scale toward regulatory T cells (Tregs).
📉 CD4+, CD8+, B cells ↓
📈 Foxp3+ Tregs ↑
A quiet immune recalibration, not just brute-force suppression.
🧠 What’s new mechanistically?
MMF not only suppresses lymphocytes but also tips the scale toward regulatory T cells (Tregs).
📉 CD4+, CD8+, B cells ↓
📈 Foxp3+ Tregs ↑
A quiet immune recalibration, not just brute-force suppression.
4️⃣
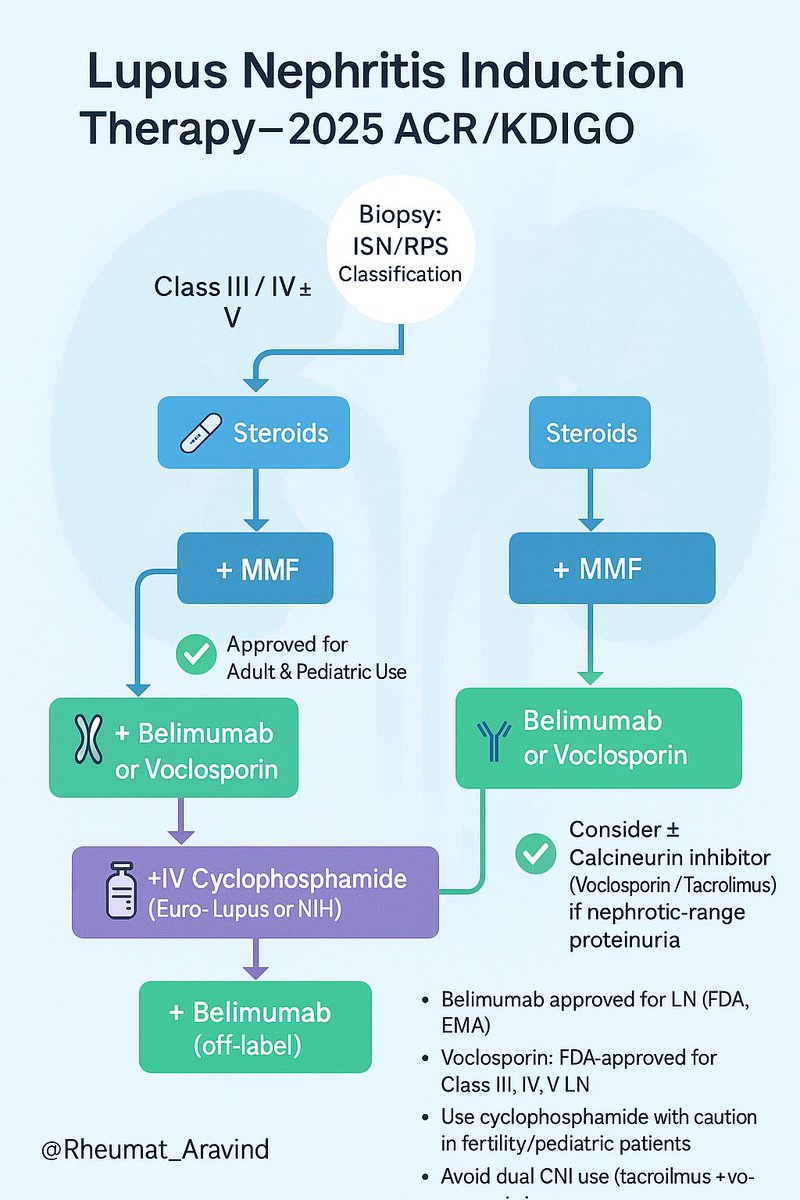
📚 Updated Guidelines (ACR & KDIGO 2024–25)
✅ MMF now first-line in lupus nephritis (esp. Class III–V)
✅ Often combined with steroids + belimumab or voclosporin
✅ Pediatric SLE? MMF is no longer off-label — it’s endorsed.
🧠 Treat early. Combine smartly.
📚 Updated Guidelines (ACR & KDIGO 2024–25)
✅ MMF now first-line in lupus nephritis (esp. Class III–V)
✅ Often combined with steroids + belimumab or voclosporin
✅ Pediatric SLE? MMF is no longer off-label — it’s endorsed.
🧠 Treat early. Combine smartly.
5️⃣
🏥 Clinical Uses (beyond LN)
• Systemic sclerosis-ILD
• ANCA vasculitis (maintenance)
• Autoimmune hepatitis (select cases)
• Uveitis, myositis, Sjögren’s (off-label)
Versatile, especially when fertility or renal preservation matters.
🏥 Clinical Uses (beyond LN)
• Systemic sclerosis-ILD
• ANCA vasculitis (maintenance)
• Autoimmune hepatitis (select cases)
• Uveitis, myositis, Sjögren’s (off-label)
Versatile, especially when fertility or renal preservation matters.
6️⃣
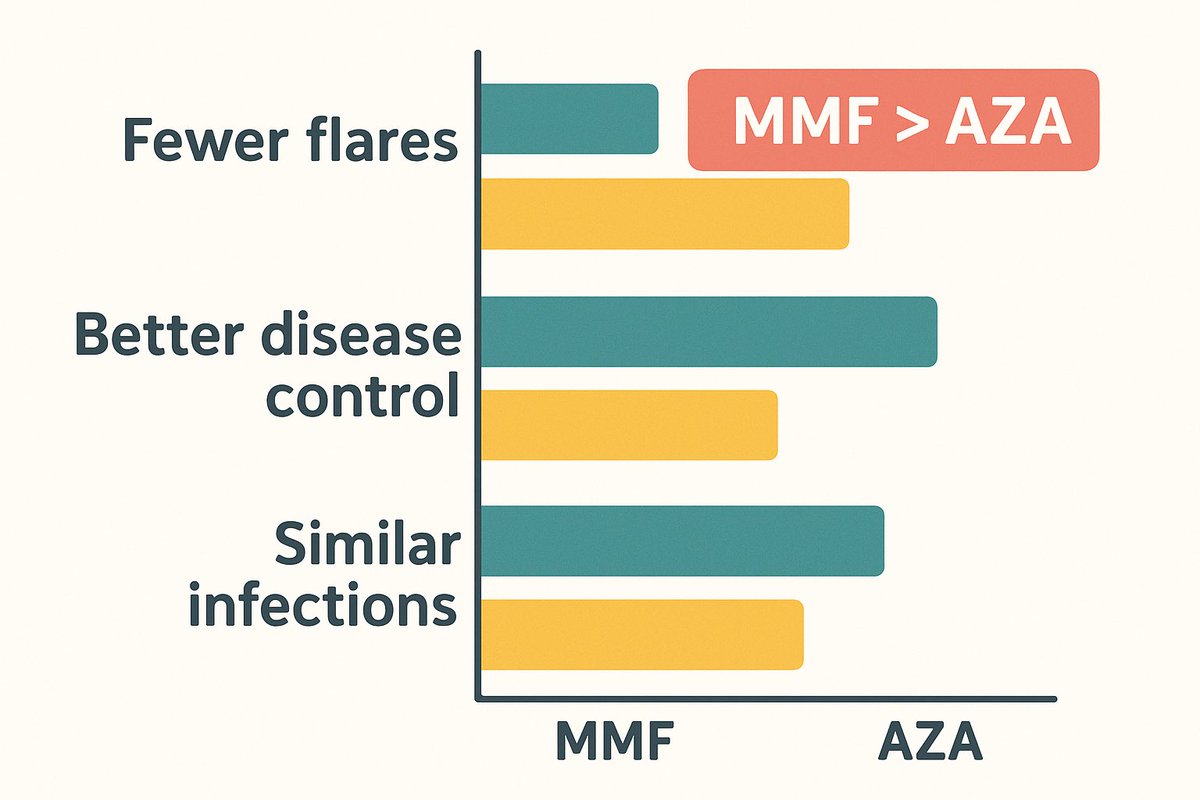
🧪 MMF vs AZA — 2025 Data
A recent RCT confirms it:
MMF > Azathioprine in preventing SLE flares during maintenance.
🛡️ Better disease control, same safety profile.
Evidence is stacking up.
🧪 MMF vs AZA — 2025 Data
A recent RCT confirms it:
MMF > Azathioprine in preventing SLE flares during maintenance.
🛡️ Better disease control, same safety profile.
Evidence is stacking up.
7️⃣
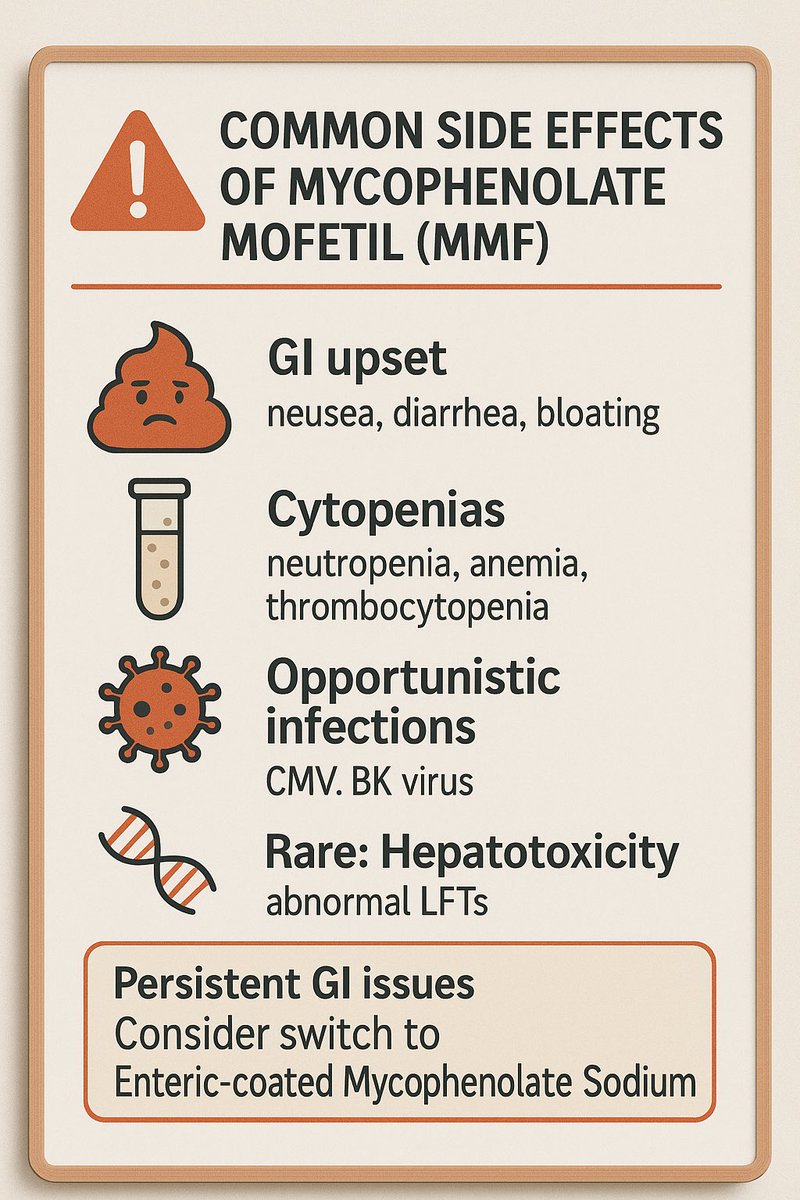
🚨 Side Effects to Watch
• GI: nausea, diarrhea
• Cytopenias
• Opportunistic infections (CMV, BK)
• Rare: hepatotoxicity
🔄 Switch to enteric-coated MPA if GI issues persist.
Stay alert, not afraid.
🚨 Side Effects to Watch
• GI: nausea, diarrhea
• Cytopenias
• Opportunistic infections (CMV, BK)
• Rare: hepatotoxicity
🔄 Switch to enteric-coated MPA if GI issues persist.
Stay alert, not afraid.
8️⃣
👶 Pregnancy & Fertility
🚫 MMF is teratogenic — linked to miscarriage and malformations.
💡 Stop 6 weeks before conception.
✅ Use azathioprine or HCQ in pregnancy.
Fertility-sparing, but not pregnancy-safe.
👶 Pregnancy & Fertility
🚫 MMF is teratogenic — linked to miscarriage and malformations.
💡 Stop 6 weeks before conception.
✅ Use azathioprine or HCQ in pregnancy.
Fertility-sparing, but not pregnancy-safe.

9️⃣
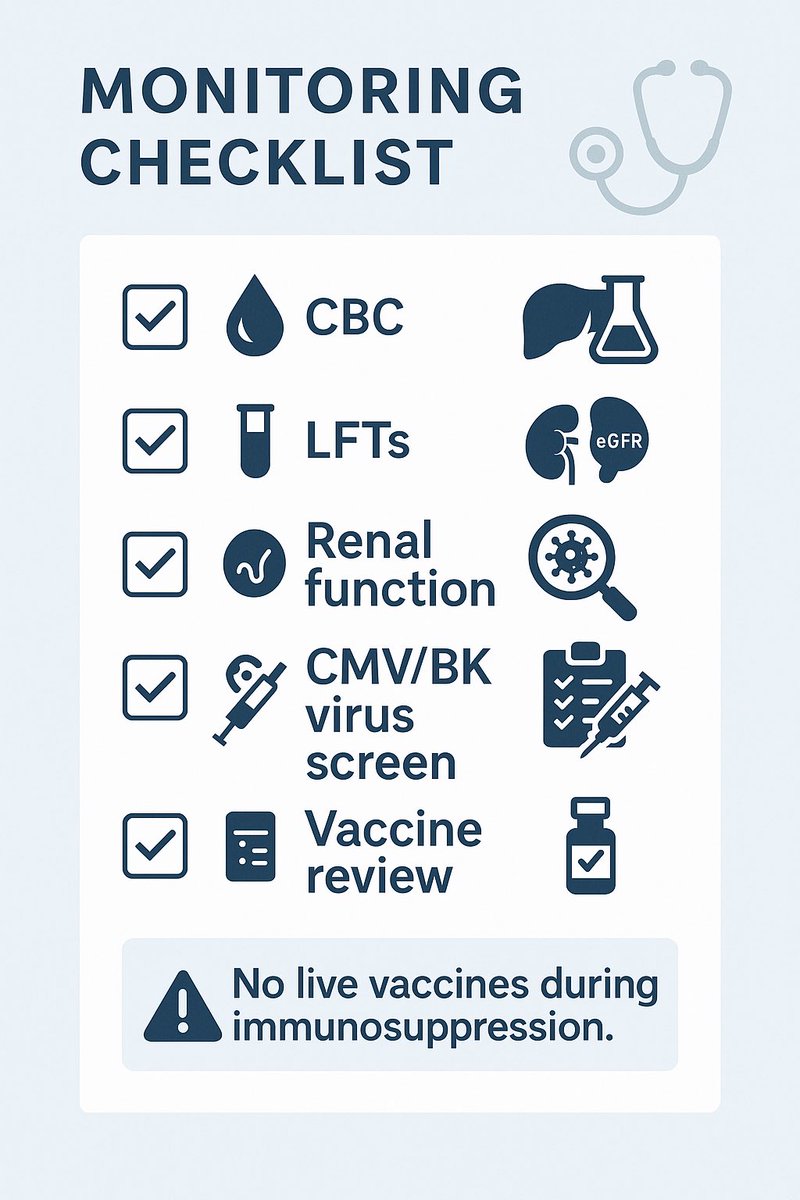
🧠 Monitoring Tips
No routine MPA levels. Focus on:
• CBC, LFTs, renal function
• Infection screening (CMV, TB, BK)
• Adherence
🧬 And don’t forget: no live vaccines during treatment.
🔄 Recheck before vaccines or surgery.
🧠 Monitoring Tips
No routine MPA levels. Focus on:
• CBC, LFTs, renal function
• Infection screening (CMV, TB, BK)
• Adherence
🧬 And don’t forget: no live vaccines during treatment.
🔄 Recheck before vaccines or surgery.
📈 Emerging Uses (2025)
• 🫁 Systemic sclerosis skin fibrosis — modest mRSS improvement in meta-analyses
• 🧠 AI-guided lupus nephritis pathology scoring now helps personalize MMF dosing
• 🧴 Liver transplant patients switching from CNIs to MMF show renal rescue!
🧬 It’s not just for lupus anymore.
• 🫁 Systemic sclerosis skin fibrosis — modest mRSS improvement in meta-analyses
• 🧠 AI-guided lupus nephritis pathology scoring now helps personalize MMF dosing
• 🧴 Liver transplant patients switching from CNIs to MMF show renal rescue!
🧬 It’s not just for lupus anymore.
1️⃣1️⃣
🧠 Pro Tips for 2025 Practice
• MMF + belimumab = synergy
• Splitting dose improves GI tolerance
• Expect immunoglobulin dip → watch for infections
• Counsel early on fertility & contraception
🎯 Use it wisely. It rewards experience.
🧠 Pro Tips for 2025 Practice
• MMF + belimumab = synergy
• Splitting dose improves GI tolerance
• Expect immunoglobulin dip → watch for infections
• Counsel early on fertility & contraception
🎯 Use it wisely. It rewards experience.
1️⃣2️⃣
💡 MMF in 2025 is not just about suppression — it’s about precision, preservation, and personalization.
From lupus kidneys to scleroderma lungs, MMF continues to deliver.
#RheumTwitter #NEETPG
💡 MMF in 2025 is not just about suppression — it’s about precision, preservation, and personalization.
From lupus kidneys to scleroderma lungs, MMF continues to deliver.
#RheumTwitter #NEETPG
• • •
Missing some Tweet in this thread? You can try to
force a refresh