
@SecKennedy says he "reviewed the science" before terminating 22 mRNA vaccine projects worth $500M.
The "data" cited? 181 pages of cherry-picked lab studies ignoring all the high-quality evidence.
The US government is citing this as its scientific basis, which is outrageous:🧵
The "data" cited? 181 pages of cherry-picked lab studies ignoring all the high-quality evidence.
The US government is citing this as its scientific basis, which is outrageous:🧵
2/ This compilation is now the official basis for ending federal funding for Nobel Prize-winning technology that has averted millions of deaths.
I've been analyzing COVID vaccine safety data since the beginning. I reviewed what @HHSGov refers to has the "science."
Here's what's actually in it - and what's missing. jamanetwork.com/journals/jama-…
I've been analyzing COVID vaccine safety data since the beginning. I reviewed what @HHSGov refers to has the "science."
Here's what's actually in it - and what's missing. jamanetwork.com/journals/jama-…
3/ What's missing
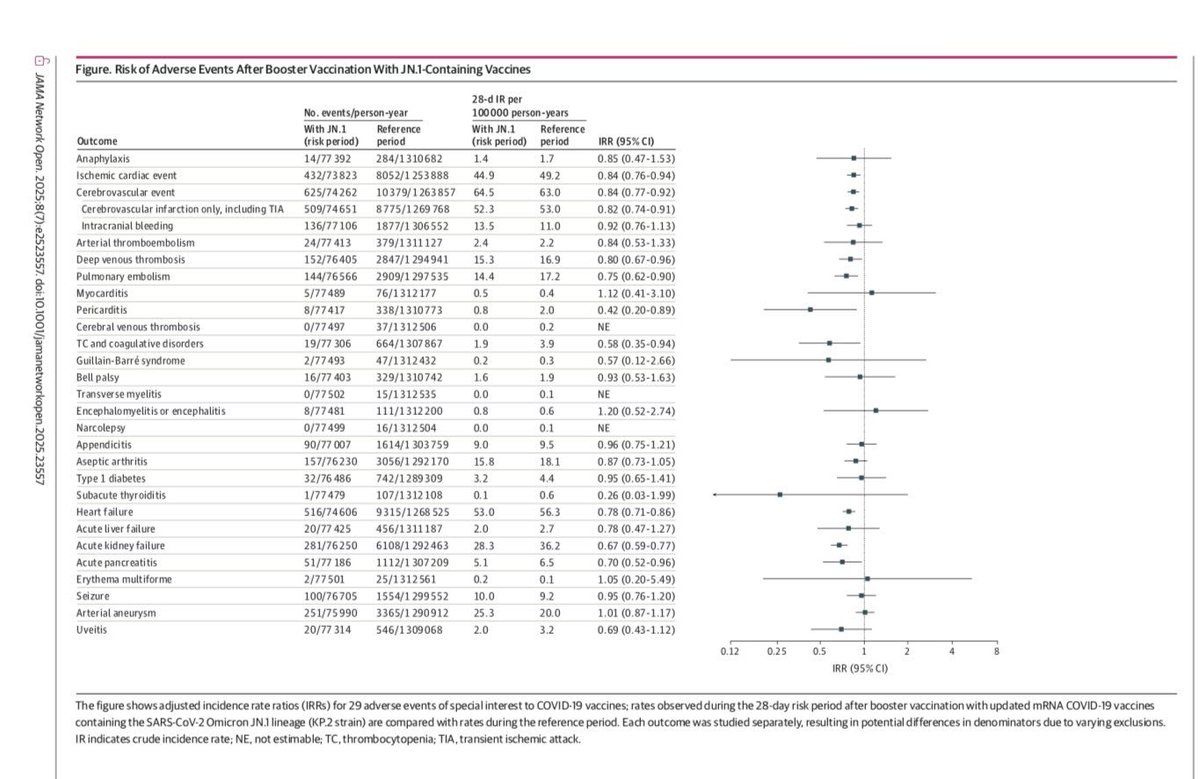
Just this week: Danish nationwide study of 1 million adults who got JN.1 boosters. Tracked 29 serious conditions for 28 days post-vaccination.
Result: No statistically significant association with any of the adverse events studied. For myocarditis specifically, the incidence rate ratio was 1.12 (95% CI: 0.41-3.10).
This is gold-standard safety monitoring. Kennedy's compilation doesn't mention it.
jamanetwork.com/journals/jaman…
Just this week: Danish nationwide study of 1 million adults who got JN.1 boosters. Tracked 29 serious conditions for 28 days post-vaccination.
Result: No statistically significant association with any of the adverse events studied. For myocarditis specifically, the incidence rate ratio was 1.12 (95% CI: 0.41-3.10).
This is gold-standard safety monitoring. Kennedy's compilation doesn't mention it.
jamanetwork.com/journals/jaman…
4/ The packet claims "375 studies prove spike protein is toxic."
Look closer: Most are in vitro studies using recombinant spike proteins or pseudoviral vectors.
They inject spike directly into mouse brains. They use IV injection when vaccines are intramuscular. They use doses hundreds to thousands of times higher than any vaccine produces.
This is basic toxicology: the dose makes the poison. Water is lethal at high enough doses. These studies show hazard, not real-world risk. The packet's own papers say "we cannot infer any causality."
Look closer: Most are in vitro studies using recombinant spike proteins or pseudoviral vectors.
They inject spike directly into mouse brains. They use IV injection when vaccines are intramuscular. They use doses hundreds to thousands of times higher than any vaccine produces.
This is basic toxicology: the dose makes the poison. Water is lethal at high enough doses. These studies show hazard, not real-world risk. The packet's own papers say "we cannot infer any causality."
5/ Yes, myocarditis occurs after mRNA vaccination and must be taken seriously. We've tracked every case since 2021.
Highest risk: young males after dose 2. Peak rates in 2021: ~106 per million (16-17 year olds), ~52-56 per million (18-24 year olds). Most cases mild and self-limited: median 2-day hospitalization, full recovery typical.
Critical context: By 2024-2025, rates dropped to background levels. COVID infection causes more frequent and severe myocarditis. The Danish study of 1 million JN.1 recipients found no statistically significant cardiac risk.
Kennedy's packet ignores both the improving safety profile and the comparison to infection risk.
cdc.gov/vaccines/covid…
Highest risk: young males after dose 2. Peak rates in 2021: ~106 per million (16-17 year olds), ~52-56 per million (18-24 year olds). Most cases mild and self-limited: median 2-day hospitalization, full recovery typical.
Critical context: By 2024-2025, rates dropped to background levels. COVID infection causes more frequent and severe myocarditis. The Danish study of 1 million JN.1 recipients found no statistically significant cardiac risk.
Kennedy's packet ignores both the improving safety profile and the comparison to infection risk.
cdc.gov/vaccines/covid…
6/ The packet claims mRNA and spike protein spread everywhere: "heart, liver, brain, ovaries."
Their evidence? Studies where scientists inject mRNA intravenously in mice. Of course IV injection distributes everywhere. That's why we don't give vaccines IV. We inject into shoulder muscle, which creates completely different pharmacokinetics.
They also cite detection of trace amounts as if it means damage. Finding molecules somewhere doesn't equal harm. We can detect single molecules with modern techniques. The question is: at what concentration and for how long?
Their evidence? Studies where scientists inject mRNA intravenously in mice. Of course IV injection distributes everywhere. That's why we don't give vaccines IV. We inject into shoulder muscle, which creates completely different pharmacokinetics.
They also cite detection of trace amounts as if it means damage. Finding molecules somewhere doesn't equal harm. We can detect single molecules with modern techniques. The question is: at what concentration and for how long?
7/ "Spike protein persists for months!"
Read their own citations carefully. Vaccine spike is typically gone within two weeks. The studies showing months of persistence? Those measured spike from Sars-CoV-2 INFECTION, not vaccination.
They're deliberately mixing infection data with vaccine data. In the packet's own studies, vaccine mRNA degrades within days to weeks, and spike protein follows shortly after. The prolonged detection they cite comes from viral replication during infection, which vaccines don't cause.
Read their own citations carefully. Vaccine spike is typically gone within two weeks. The studies showing months of persistence? Those measured spike from Sars-CoV-2 INFECTION, not vaccination.
They're deliberately mixing infection data with vaccine data. In the packet's own studies, vaccine mRNA degrades within days to weeks, and spike protein follows shortly after. The prolonged detection they cite comes from viral replication during infection, which vaccines don't cause.
8/ The packet claims anaphylaxis occurs in 1 in 2,280 doses.
CDC data from billions of real-world doses: about 5 per million (0.0005%). That's 400 times lower than the packet suggests.
For comparison: Penicillin causes anaphylaxis in 1 in 5,000. Peanuts in 1 in 50 for allergic individuals. The packet presents PEG reactions as unique to mRNA vaccines, but PEG is in toothpaste, cosmetics, and many medications. We don't ban those either.
cdc.gov/coronavirus/20…
CDC data from billions of real-world doses: about 5 per million (0.0005%). That's 400 times lower than the packet suggests.
For comparison: Penicillin causes anaphylaxis in 1 in 5,000. Peanuts in 1 in 50 for allergic individuals. The packet presents PEG reactions as unique to mRNA vaccines, but PEG is in toothpaste, cosmetics, and many medications. We don't ban those either.
cdc.gov/coronavirus/20…
9/ The packet's section on "immune imprinting" misrepresents basic immunology.
Yes, first exposures shape later responses. That's how all vaccines work. It's why we update flu shots yearly. The packet frames this as a fatal flaw, but their own sources call it a "design challenge" that can be addressed through updated formulations.
They claim vaccines "prevented antibody formation to other viral parts." But that's exactly what variant-updated boosters address. The same flexibility they're criticizing is what makes mRNA valuable.
Yes, first exposures shape later responses. That's how all vaccines work. It's why we update flu shots yearly. The packet frames this as a fatal flaw, but their own sources call it a "design challenge" that can be addressed through updated formulations.
They claim vaccines "prevented antibody formation to other viral parts." But that's exactly what variant-updated boosters address. The same flexibility they're criticizing is what makes mRNA valuable.
10/ What's completely missing from Kennedy's 181 pages:
Global Vaccine Data Network: 99 million people, confirmed known rare risks, found no hidden dangers
CDC: Unvaccinated had 53x higher death risk during
Delta Commonwealth Fund: 3.2 million US lives saved through 2022 Cost-benefit: COVID cost $16 trillion. Vaccine investment: $18 billion. Return: hundreds to one.
cdc.gov/mmwr/volumes/7… commonwealthfund.org/blog/2022/two-…
Global Vaccine Data Network: 99 million people, confirmed known rare risks, found no hidden dangers
CDC: Unvaccinated had 53x higher death risk during
Delta Commonwealth Fund: 3.2 million US lives saved through 2022 Cost-benefit: COVID cost $16 trillion. Vaccine investment: $18 billion. Return: hundreds to one.
cdc.gov/mmwr/volumes/7… commonwealthfund.org/blog/2022/two-…
11/ Here's what Kennedy just terminated based on this packet:
mRNA technology isn't just for COVID. We're killing vaccines for diseases that have plagued humanity for decades:
Norovirus (Phase 3): Would prevent 200,000+ hospitalizations yearly from the virus that shuts down schools and cruise ships. Any parents out there deal with norovirus like I have?! It's no picnic!
CMV (Phase 3): Would prevent the leading cause of non-genetic deafness in newborns
Lyme disease: Two vaccines in human trials offering seasonal protection
EBV: One for mono, another being tested to prevent
MS relapses
HIV: Early trials using germline-targeting approaches
All dead because of cherry-picked mouse studies.
modernatx.com/research-devel…
mRNA technology isn't just for COVID. We're killing vaccines for diseases that have plagued humanity for decades:
Norovirus (Phase 3): Would prevent 200,000+ hospitalizations yearly from the virus that shuts down schools and cruise ships. Any parents out there deal with norovirus like I have?! It's no picnic!
CMV (Phase 3): Would prevent the leading cause of non-genetic deafness in newborns
Lyme disease: Two vaccines in human trials offering seasonal protection
EBV: One for mono, another being tested to prevent
MS relapses
HIV: Early trials using germline-targeting approaches
All dead because of cherry-picked mouse studies.
modernatx.com/research-devel…
12/ Kennedy says he'll pivot to "safer, broader, whole-virus vaccines."
Those take 6+ months to update for variants. mRNA takes weeks. In the 2009 H1N1 pandemic, it took 6 months to retool egg-based production.
With mRNA, we went from sequence to trials in under 60 days.
H5N1 is currently spreading in dairy cattle. If it adapts to humans, that time difference between platforms won't be academic. It will be measured in lives.
And why take us backwards? Don't we want to make progress?
cdc.gov/bird-flu/situa…
Those take 6+ months to update for variants. mRNA takes weeks. In the 2009 H1N1 pandemic, it took 6 months to retool egg-based production.
With mRNA, we went from sequence to trials in under 60 days.
H5N1 is currently spreading in dairy cattle. If it adapts to humans, that time difference between platforms won't be academic. It will be measured in lives.
And why take us backwards? Don't we want to make progress?
cdc.gov/bird-flu/situa…
13/ No respiratory virus vaccine has ever guaranteed sterilizing immunity. Not flu. Not RSV. The goal has always been preventing severe disease and death.
By that metric, mRNA vaccines succeeded spectacularly. Setting impossible standards and then declaring failure when they're not met isn't science. It's sabotage.
By that metric, mRNA vaccines succeeded spectacularly. Setting impossible standards and then declaring failure when they're not met isn't science. It's sabotage.
14/ This decision affects everyone.
As I told @JuliaElenaMusto @Independent
“Vaccines aren’t some niche drug. We’re talking about medicines that apply to literally every human being on the planet. We should have learned from the SARS-CoV-2 pandemic that everyone is potentially susceptible to pandemic threats.”
@HHSGov is citing mouse studies over billions of real doses. Setting impossible standards, then declaring failure. Terminating programs that could prevent the next pandemic.
This goes beyond bad policy. It actively undermines confidence in vaccines that work. When the next pandemic comes, we will need the very tools being dismantled.
Silence now will have a cost. And it will be measured in lives.
the-independent.com/news/health/rf…
As I told @JuliaElenaMusto @Independent
“Vaccines aren’t some niche drug. We’re talking about medicines that apply to literally every human being on the planet. We should have learned from the SARS-CoV-2 pandemic that everyone is potentially susceptible to pandemic threats.”
@HHSGov is citing mouse studies over billions of real doses. Setting impossible standards, then declaring failure. Terminating programs that could prevent the next pandemic.
This goes beyond bad policy. It actively undermines confidence in vaccines that work. When the next pandemic comes, we will need the very tools being dismantled.
Silence now will have a cost. And it will be measured in lives.
the-independent.com/news/health/rf…
• • •
Missing some Tweet in this thread? You can try to
force a refresh




