🧵Vortioxetine in SSRI-Resistant OCD – Early Clinical Signals 🚨1/4
Study :
-64 adults with DSM-5 OCD
-SSRI non-responders
-Vortioxetine monotherapy ≥20 mg/day
-≥8 weeks treatment
👉Primary outcome: Y-BOCS
👉Secondary: HAM-D, HAM-A, adverse events
Results 👇1/4
Study :
-64 adults with DSM-5 OCD
-SSRI non-responders
-Vortioxetine monotherapy ≥20 mg/day
-≥8 weeks treatment
👉Primary outcome: Y-BOCS
👉Secondary: HAM-D, HAM-A, adverse events
Results 👇1/4

1/ Results:
- 39.1% met responder criteria (≥25% ↓ Y-BOCS)
-Y-BOCS ⬇️from 27.1 → 20.7
-HAM-D and HAM-A improved significantly
-Most common SEs: nausea (29.7%), sedation (18.8%)
-No serious adverse events
- 39.1% met responder criteria (≥25% ↓ Y-BOCS)
-Y-BOCS ⬇️from 27.1 → 20.7
-HAM-D and HAM-A improved significantly
-Most common SEs: nausea (29.7%), sedation (18.8%)
-No serious adverse events
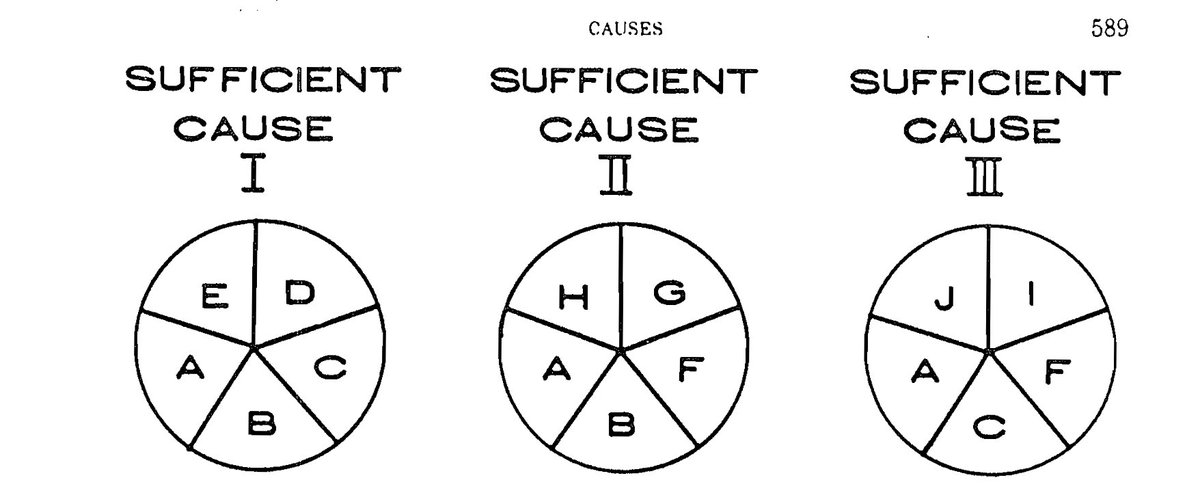
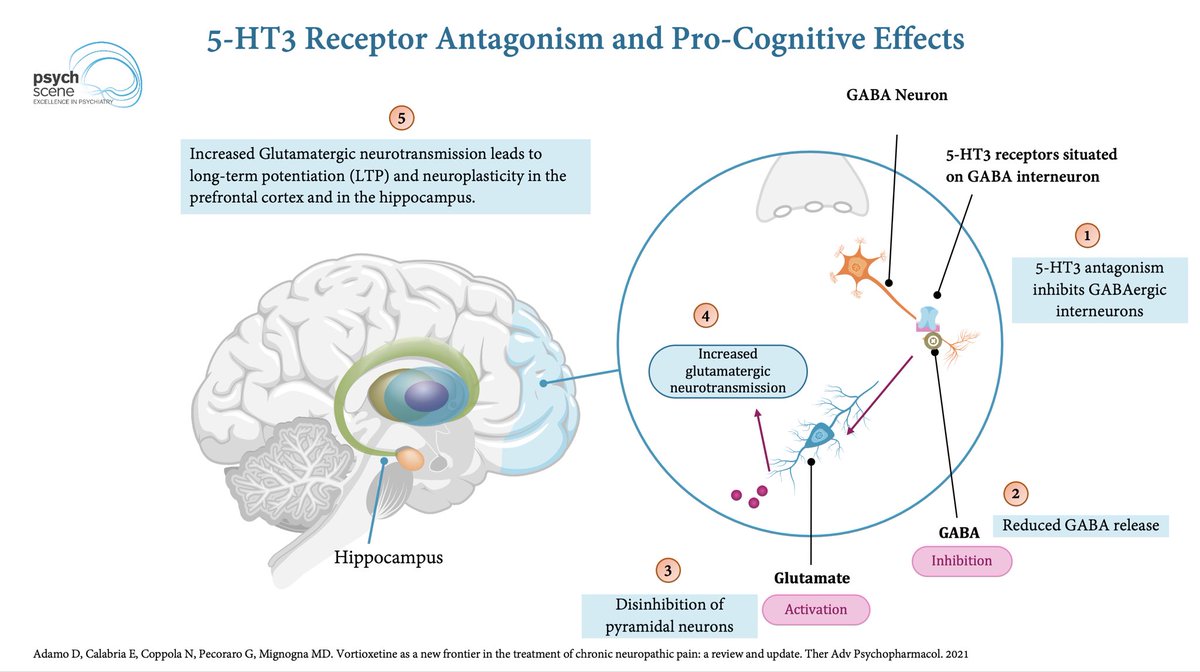
2/ One key mechanism may be 5-HT3 antagonism
We know ondansetron, a selective 5-HT3 antagonist, has shown benefits in OCD.
Vortioxetine also has 5HT3 antagonism, and it’s possible the clinical effects in this study emerged at higher doses, which is also where the response was most evident.
*nausea as a side effect has been postulated to be due to Vortioxetine being a partial 5HT3 agonist rather than antagonist.
We know ondansetron, a selective 5-HT3 antagonist, has shown benefits in OCD.
Vortioxetine also has 5HT3 antagonism, and it’s possible the clinical effects in this study emerged at higher doses, which is also where the response was most evident.
*nausea as a side effect has been postulated to be due to Vortioxetine being a partial 5HT3 agonist rather than antagonist.
3/ Clinical insights -
👉lower doses (5–10 mg) can help mild/moderate presentations of depression ( with ACE dysfunction)
👉For melancholic mod-severe higher doses 15-20 mg are often needed
👉Also trialled in Long COVID.
And here is something really interesting 👉 “Vortioxetine, exhibits anticancer abilities and can traverse the blood-brain barrier... vortioxetine inhibits the PI3K-Akt signaling pathway, which is known to play a critical role in promoting the progression of GBM. Furthermore, vortioxetine induces cytoprotective autophagy,
👉lower doses (5–10 mg) can help mild/moderate presentations of depression ( with ACE dysfunction)
👉For melancholic mod-severe higher doses 15-20 mg are often needed
👉Also trialled in Long COVID.
And here is something really interesting 👉 “Vortioxetine, exhibits anticancer abilities and can traverse the blood-brain barrier... vortioxetine inhibits the PI3K-Akt signaling pathway, which is known to play a critical role in promoting the progression of GBM. Furthermore, vortioxetine induces cytoprotective autophagy,
4/ Learn more about Vortioxetine here
👉 psychscenehub.com/psychinsights/…
Paper 👉 frontiersin.org/journals/psych…
🧵 END
👉 psychscenehub.com/psychinsights/…
Paper 👉 frontiersin.org/journals/psych…
🧵 END
• • •
Missing some Tweet in this thread? You can try to
force a refresh