
Psychiatrist blending neuroscience with real-world practice. Insights beyond the textbooks, made actionable. Follow for clear, practical takes.
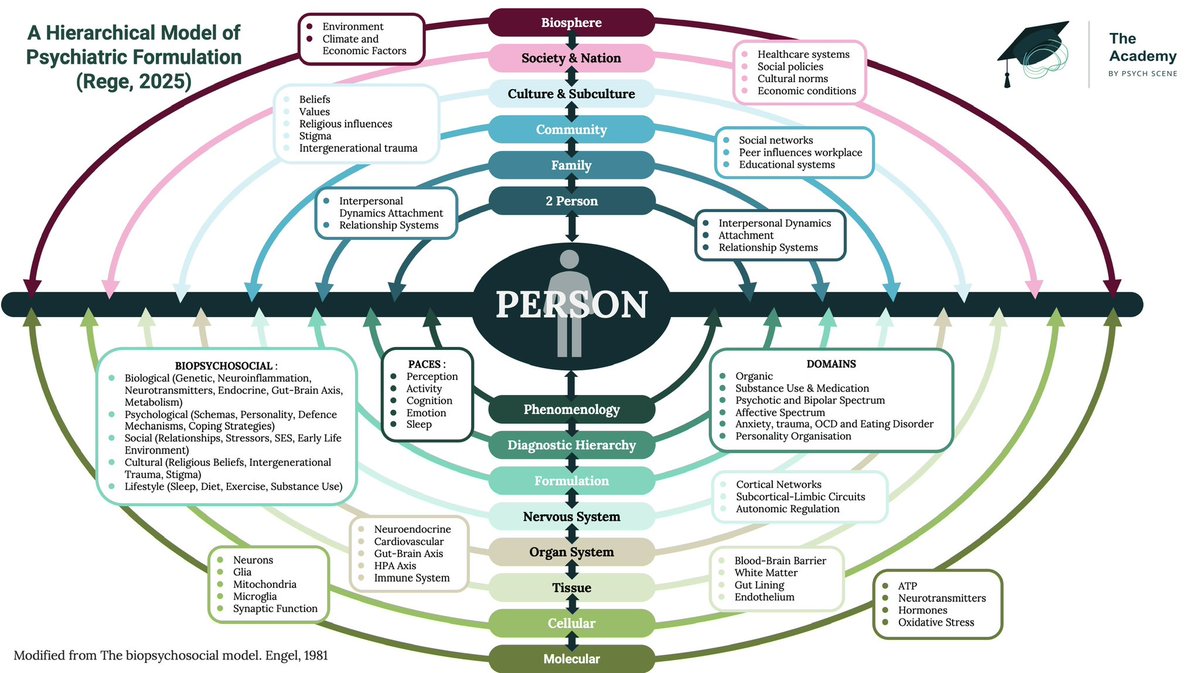 1/ Below-the-person targets
1/ Below-the-person targets 1/ The first ‘mistake’ is to treat masking as though it simply means “pretending.”
1/ The first ‘mistake’ is to treat masking as though it simply means “pretending.” 2/ Prof Hughes in Melbourne 2013
2/ Prof Hughes in Melbourne 2013 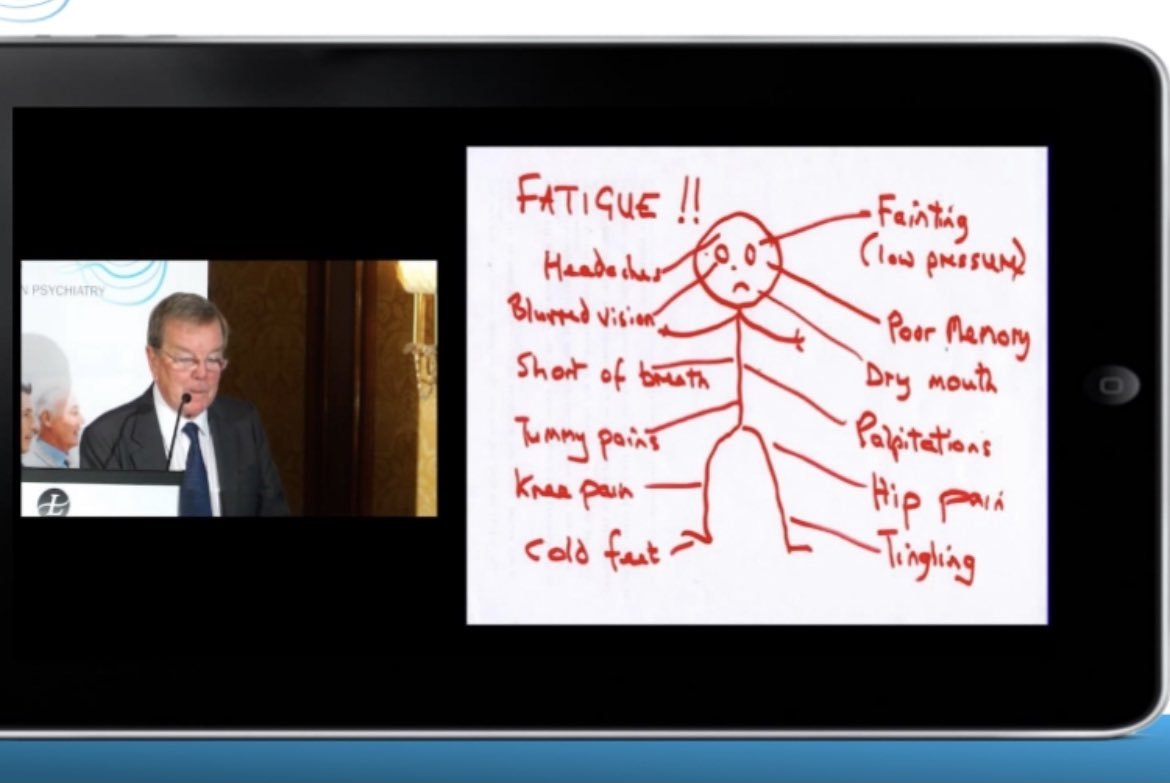
 1/ In cannabinoid hyperemesis syndrome (CHS), patients often report compulsive hot showers or baths that temporarily relieve severe nausea and vomiting.
1/ In cannabinoid hyperemesis syndrome (CHS), patients often report compulsive hot showers or baths that temporarily relieve severe nausea and vomiting. 1/ Lessons from angina -
1/ Lessons from angina - 
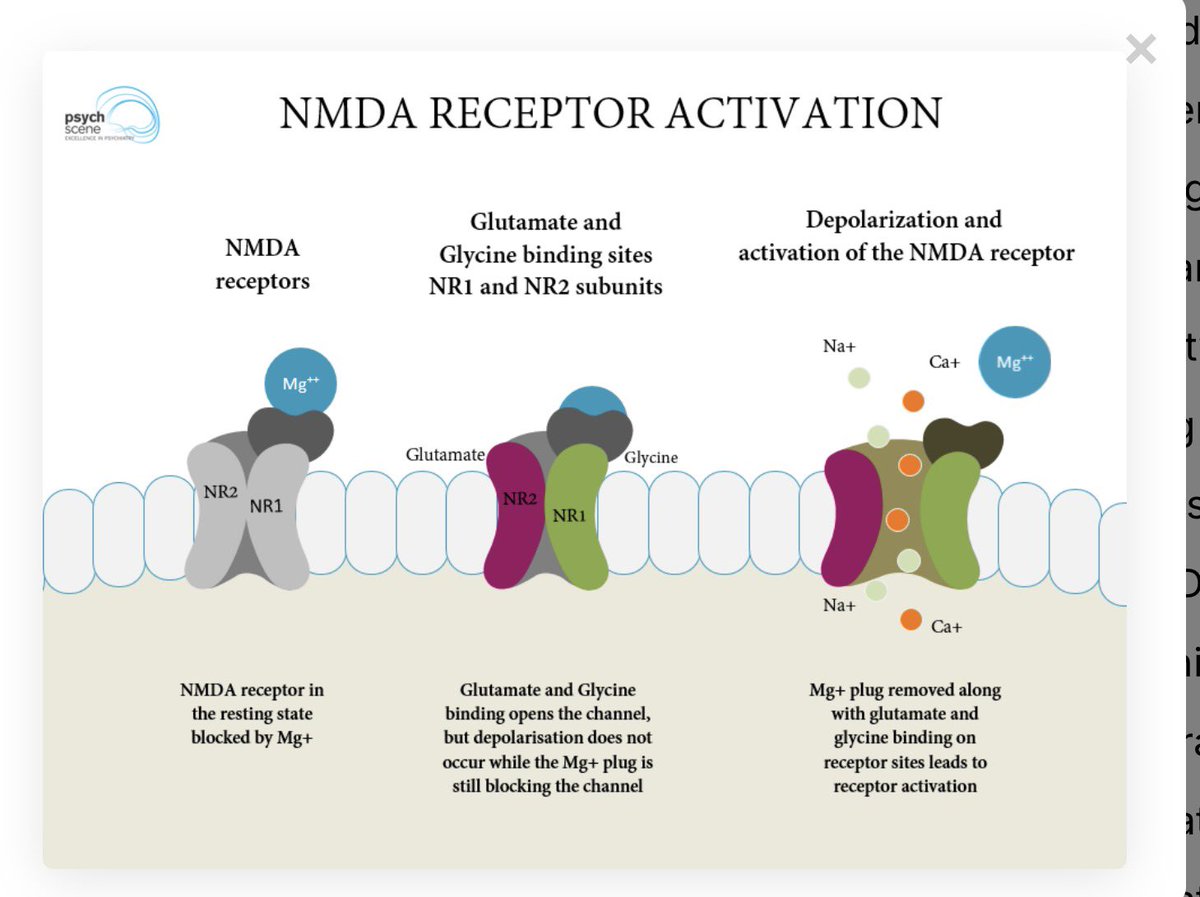 1/ Receptor selectivity
1/ Receptor selectivity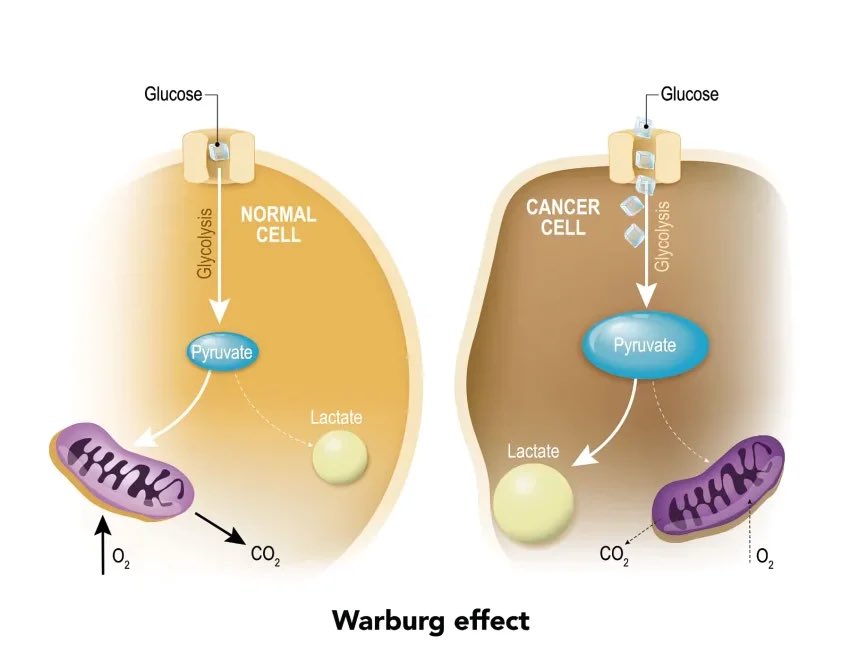 1/ In cancer, one of the earliest changes isn’t a mass or a tumour.
1/ In cancer, one of the earliest changes isn’t a mass or a tumour. 1/ Prof Michael Berk has just published an important editorial in the British Journal of Psychiatry that articulates something many clinicians feel but rarely name.
1/ Prof Michael Berk has just published an important editorial in the British Journal of Psychiatry that articulates something many clinicians feel but rarely name.

 1/ Sleep problems in ADHD are heterogeneous.
1/ Sleep problems in ADHD are heterogeneous. 1️⃣ Treat diagnosis as a process, not an endpoint
1️⃣ Treat diagnosis as a process, not an endpoint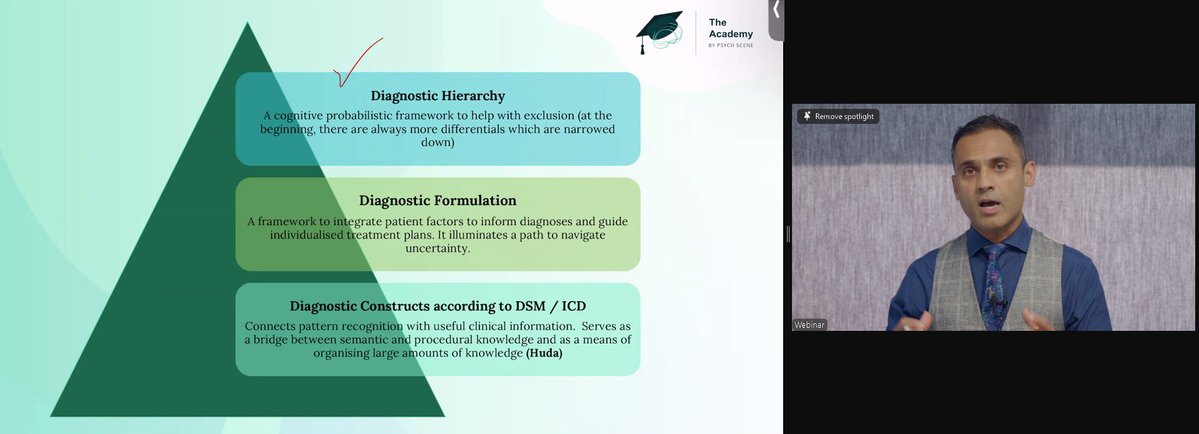
 1/ Psychosis isn’t just about voices or dopamine.
1/ Psychosis isn’t just about voices or dopamine. 1/At #WCP25 Attended a talk by Prof Tomas Paus and this one theme stood out - the retina.
1/At #WCP25 Attended a talk by Prof Tomas Paus and this one theme stood out - the retina.
 1/ What we often call “ADHD” is a cluster of domains -
1/ What we often call “ADHD” is a cluster of domains - 


 1/ As a psychiatrist who work in addiction psychiatry - Understanding neuroscience is crucial because the brain doesn’t label behaviours as gambling or porn.
1/ As a psychiatrist who work in addiction psychiatry - Understanding neuroscience is crucial because the brain doesn’t label behaviours as gambling or porn.
 1/ Role of D3 receptors #WCP25 #WCP2025
1/ Role of D3 receptors #WCP25 #WCP2025 
 1/ Maxim 1: Define the depression
1/ Maxim 1: Define the depression
 2/ That factor is Depression and exhaustion (DEEX)
2/ That factor is Depression and exhaustion (DEEX)  1/ STAR*D is often described as a pragmatic trial.
1/ STAR*D is often described as a pragmatic trial.
 1/ Psychotherapy is essential in BPD.
1/ Psychotherapy is essential in BPD.  1/ Depression is frequently reduced to sadness or low mood.
1/ Depression is frequently reduced to sadness or low mood.