🧵 ANA (Antinuclear Antibody): What Every GP Needs To Know—2025 Guide
1/ What is ANA—and Why Test It?
ANA is a blood test that helps detect autoantibodies against cell nuclei, seen in autoimmune diseases like lupus, Sjögren’s, and more. It’s NOT a screening test for general complaints. Use it when history or exam genuinely points to autoimmune disorders
@IhabFathiSulima @DrAkhilX @CelestinoGutirr @Janetbirdope @SarahSchaferMD @NeuroSjogrens #MedTwitter #RheumatX
1/ What is ANA—and Why Test It?
ANA is a blood test that helps detect autoantibodies against cell nuclei, seen in autoimmune diseases like lupus, Sjögren’s, and more. It’s NOT a screening test for general complaints. Use it when history or exam genuinely points to autoimmune disorders
@IhabFathiSulima @DrAkhilX @CelestinoGutirr @Janetbirdope @SarahSchaferMD @NeuroSjogrens #MedTwitter #RheumatX

2/ Who Should Be Tested?
Test ANA only when you see signs such as:
•Unexplained, non-infectious joint pain/swelling
•Persistent rash, especially photosensitive
•Raynaud’s phenomenon
•Sicca symptoms (dry eyes/mouth)
•Multi-system symptoms (e.g., nephritis, serositis)
Test ANA only when you see signs such as:
•Unexplained, non-infectious joint pain/swelling
•Persistent rash, especially photosensitive
•Raynaud’s phenomenon
•Sicca symptoms (dry eyes/mouth)
•Multi-system symptoms (e.g., nephritis, serositis)

3/ How To Interpret ANA Results
•Negative ANA: Very low likelihood of connective tissue disease, but rarely rules out all autoimmune illness.
•Positive ANA: Means autoantibodies were detected, but CAUTION! Many healthy people, especially elderly and women, can test positive.
•Negative ANA: Very low likelihood of connective tissue disease, but rarely rules out all autoimmune illness.
•Positive ANA: Means autoantibodies were detected, but CAUTION! Many healthy people, especially elderly and women, can test positive.

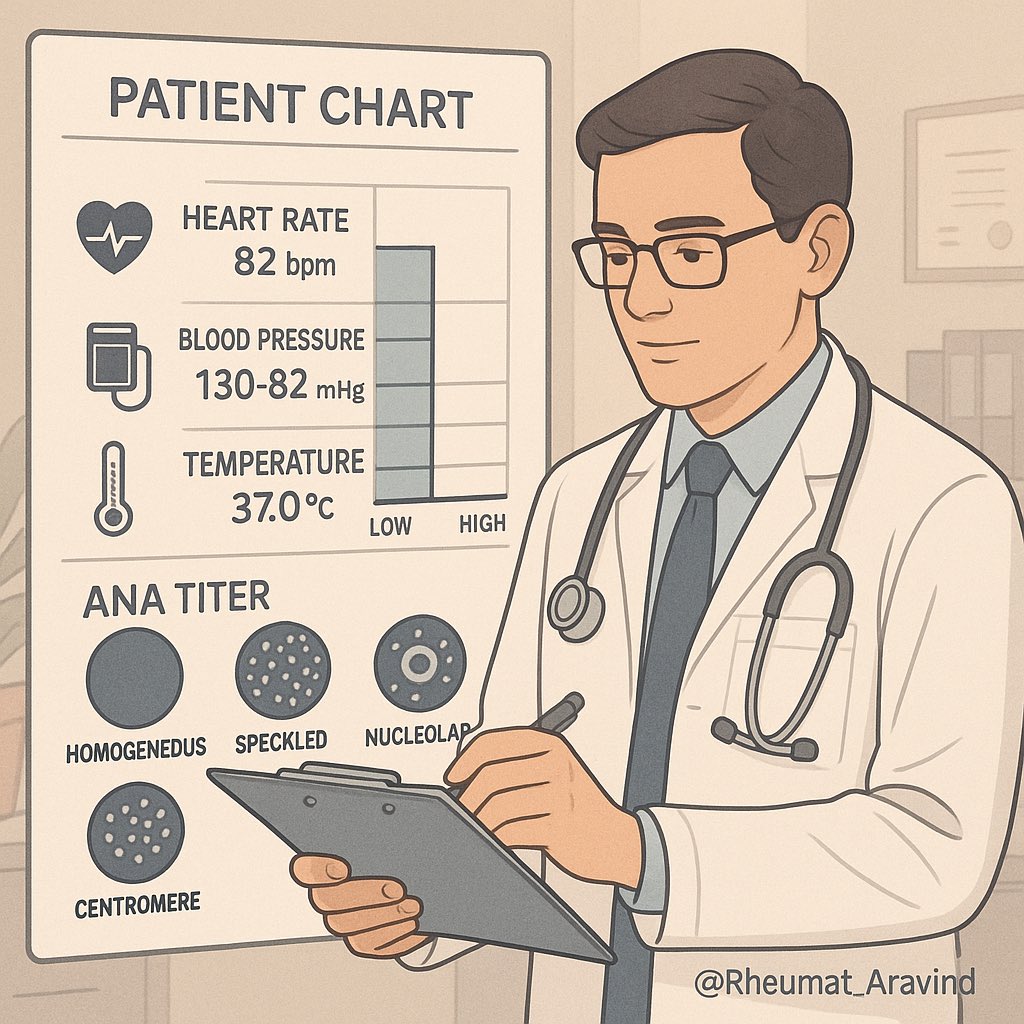
4/ Clinical Context is Everything
A positive ANA doesn’t make the diagnosis. Look at titer (strength) and pattern, but always match results to clinical findings.
•Low titer (≤1:80): Often non-specific, can occur in healthy people.
•High titer (≥1:160): More likely significant, especially with typical symptoms.
A positive ANA doesn’t make the diagnosis. Look at titer (strength) and pattern, but always match results to clinical findings.
•Low titer (≤1:80): Often non-specific, can occur in healthy people.
•High titer (≥1:160): More likely significant, especially with typical symptoms.
5/ Common Pitfalls
•Do NOT order ANA for general fatigue, back pain, or isolated arthralgia.
•Do NOT treat ANA positivity alone—diagnose and manage based on the whole clinical picture, not just the lab.
•Do NOT order ANA for general fatigue, back pain, or isolated arthralgia.
•Do NOT treat ANA positivity alone—diagnose and manage based on the whole clinical picture, not just the lab.

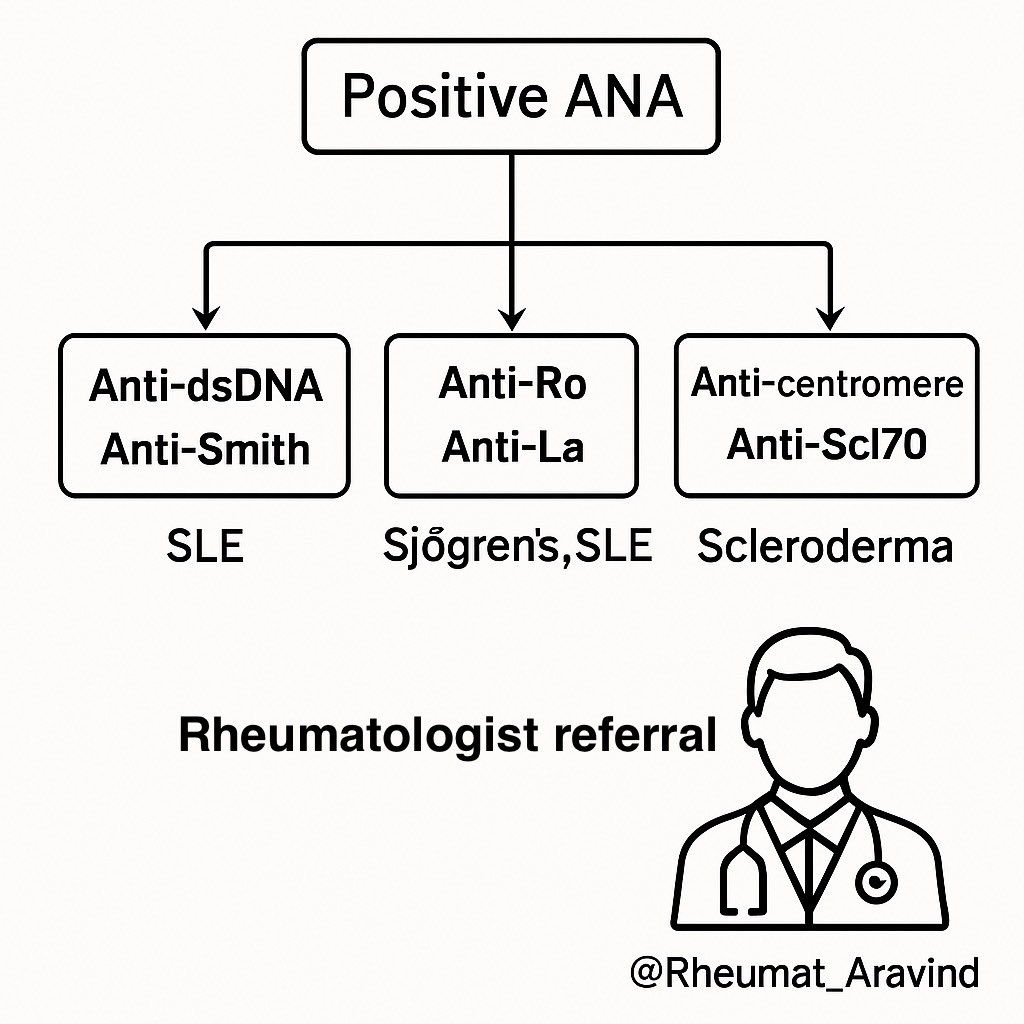
6/ Next Steps After Positive ANA
If clinical suspicion remains, GP should consider further antibody tests:
•Anti-dsDNA, anti-Smith (SLE)
•Anti-Ro, anti-La (Sjögren’s, SLE)
•Anti-centromere, anti-Scl70 (Scleroderma)
Work with a rheumatologist if unclear, especially for moderate/high titers or multi-system complaints.
If clinical suspicion remains, GP should consider further antibody tests:
•Anti-dsDNA, anti-Smith (SLE)
•Anti-Ro, anti-La (Sjögren’s, SLE)
•Anti-centromere, anti-Scl70 (Scleroderma)
Work with a rheumatologist if unclear, especially for moderate/high titers or multi-system complaints.
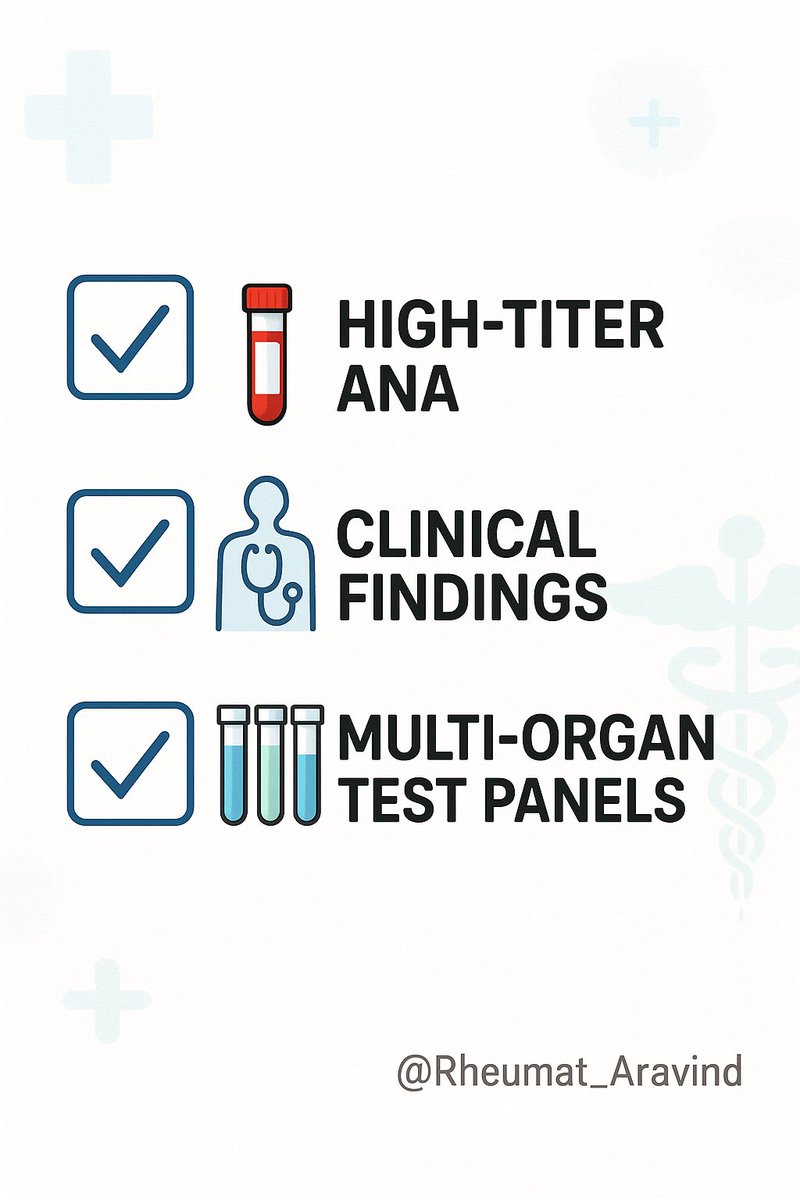
7/ Pearls for GPs
•ANA positivity alone rarely equals disease.
•High-titer or active patterns (homogenous, speckled, centromere, nucleolar) deserve attention if symptoms fit.
•Always interpret ANA alongside CBC, renal, and liver panels, complement levels, and urinalysis to spot multi-organ involvement.
•ANA positivity alone rarely equals disease.
•High-titer or active patterns (homogenous, speckled, centromere, nucleolar) deserve attention if symptoms fit.
•Always interpret ANA alongside CBC, renal, and liver panels, complement levels, and urinalysis to spot multi-organ involvement.
8/ Summary for General Practice
ANA is a valuable tool—used in the right context. Avoid indiscriminate ordering. Use clinical suspicion, interpret results carefully, confirm with further antibody tests, and refer to rheumatology when in doubt.
—
Share to help general practitioners use ANA wisely—and avoid common clinical pitfalls in 2025. #Rheumatology #GPs #AutoimmuneTesting
ANA is a valuable tool—used in the right context. Avoid indiscriminate ordering. Use clinical suspicion, interpret results carefully, confirm with further antibody tests, and refer to rheumatology when in doubt.
—
Share to help general practitioners use ANA wisely—and avoid common clinical pitfalls in 2025. #Rheumatology #GPs #AutoimmuneTesting
• • •
Missing some Tweet in this thread? You can try to
force a refresh