🧵 ANCA in Rheumatology:
Tweet 1:
ANCA — one antibody, many confusions.
From GPA to drug-induced vasculitis, it’s powerful when used right…
and misleading when used wrong.
Here’s a quick guide 👇
@IhabFathiSulima @DrAkhilX @CelestinoGutirr #MedTwitter #Rheumatology
Tweet 1:
ANCA — one antibody, many confusions.
From GPA to drug-induced vasculitis, it’s powerful when used right…
and misleading when used wrong.
Here’s a quick guide 👇
@IhabFathiSulima @DrAkhilX @CelestinoGutirr #MedTwitter #Rheumatology

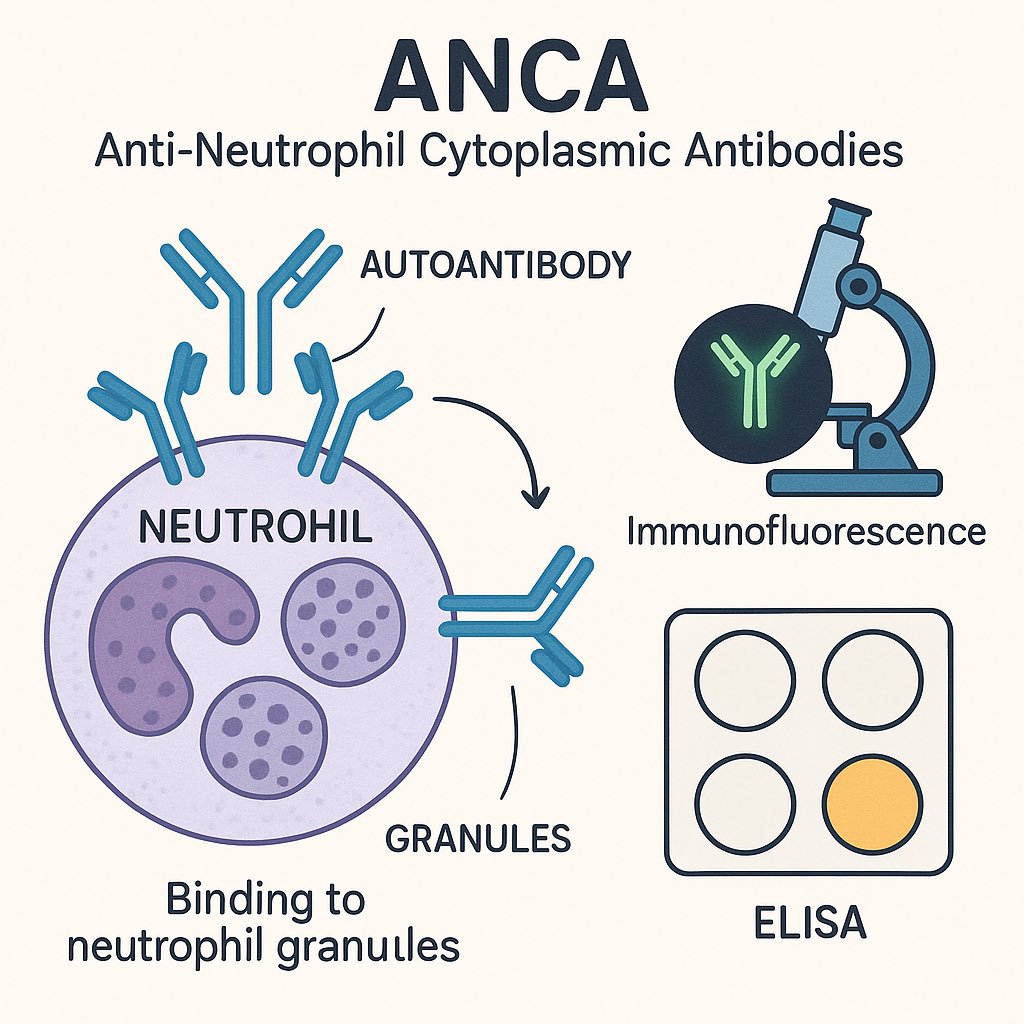
Tweet 2 (What is ANCA?):
•Anti-Neutrophil Cytoplasmic Antibodies
•Autoantibodies targeting neutrophil granule proteins
•Tested by:
🔬 Immunofluorescence (IFA)
🧪 Antigen-specific assays (ELISA, CLIA)
•Anti-Neutrophil Cytoplasmic Antibodies
•Autoantibodies targeting neutrophil granule proteins
•Tested by:
🔬 Immunofluorescence (IFA)
🧪 Antigen-specific assays (ELISA, CLIA)
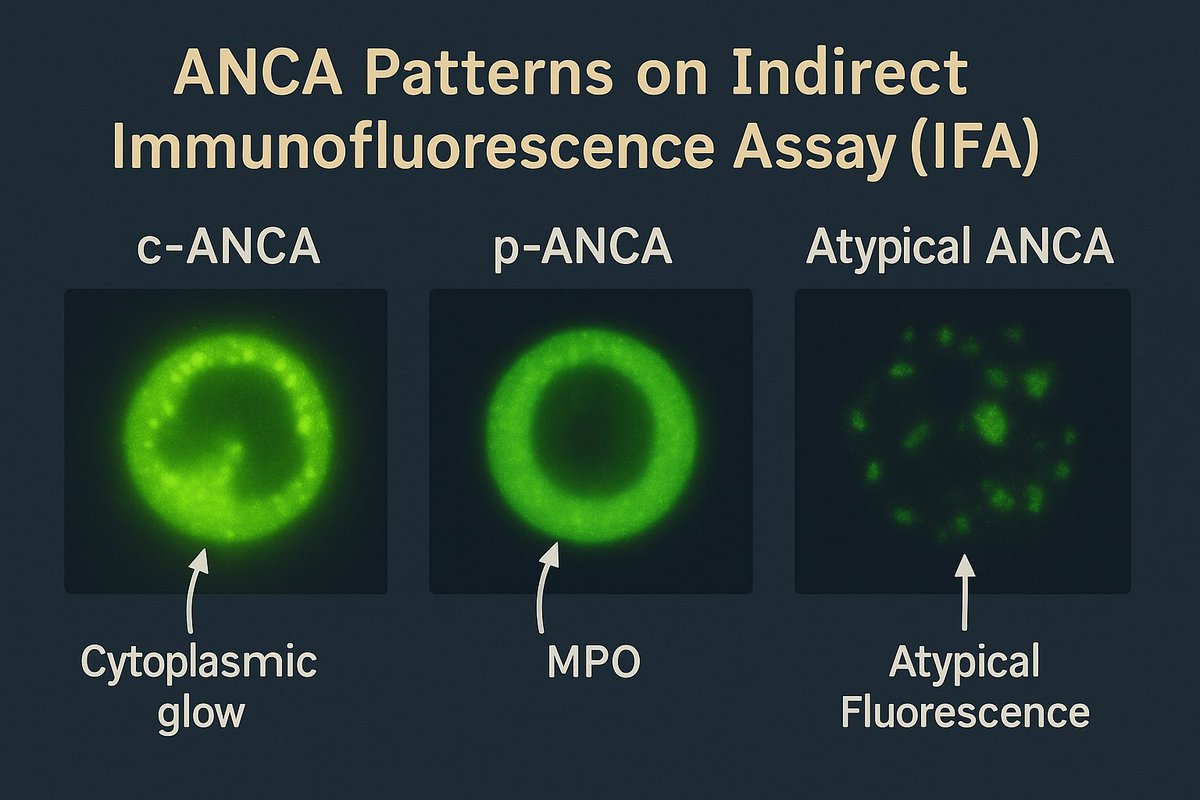
Tweet 3 (Patterns):
•c-ANCA → cytoplasmic glow → usually PR3
•p-ANCA → perinuclear halo → usually MPO
•Atypical ANCA → seen in IBD, drugs, infections
•c-ANCA → cytoplasmic glow → usually PR3
•p-ANCA → perinuclear halo → usually MPO
•Atypical ANCA → seen in IBD, drugs, infections
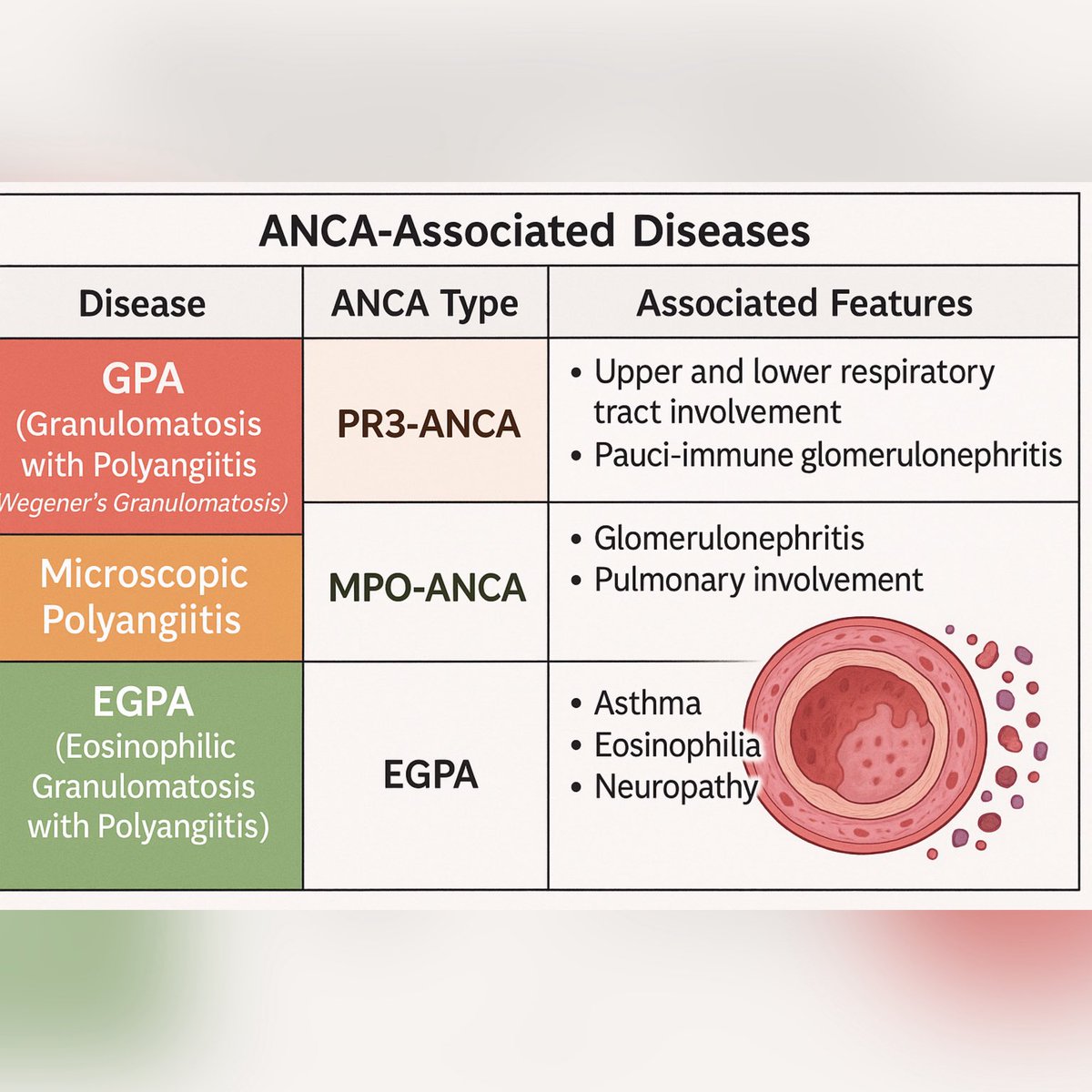
Tweet 4 (Associated diseases):
•GPA → PR3-ANCA (c-ANCA)
•MPA → MPO-ANCA (p-ANCA)
•EGPA → MPO-ANCA (but many negative)
•Others: drug-induced vasculitis, IBD, autoimmune hepatitis
⚠️ Not all vasculitis is ANCA-positive (e.g., PAN, limited GPA).
•GPA → PR3-ANCA (c-ANCA)
•MPA → MPO-ANCA (p-ANCA)
•EGPA → MPO-ANCA (but many negative)
•Others: drug-induced vasculitis, IBD, autoimmune hepatitis
⚠️ Not all vasculitis is ANCA-positive (e.g., PAN, limited GPA).
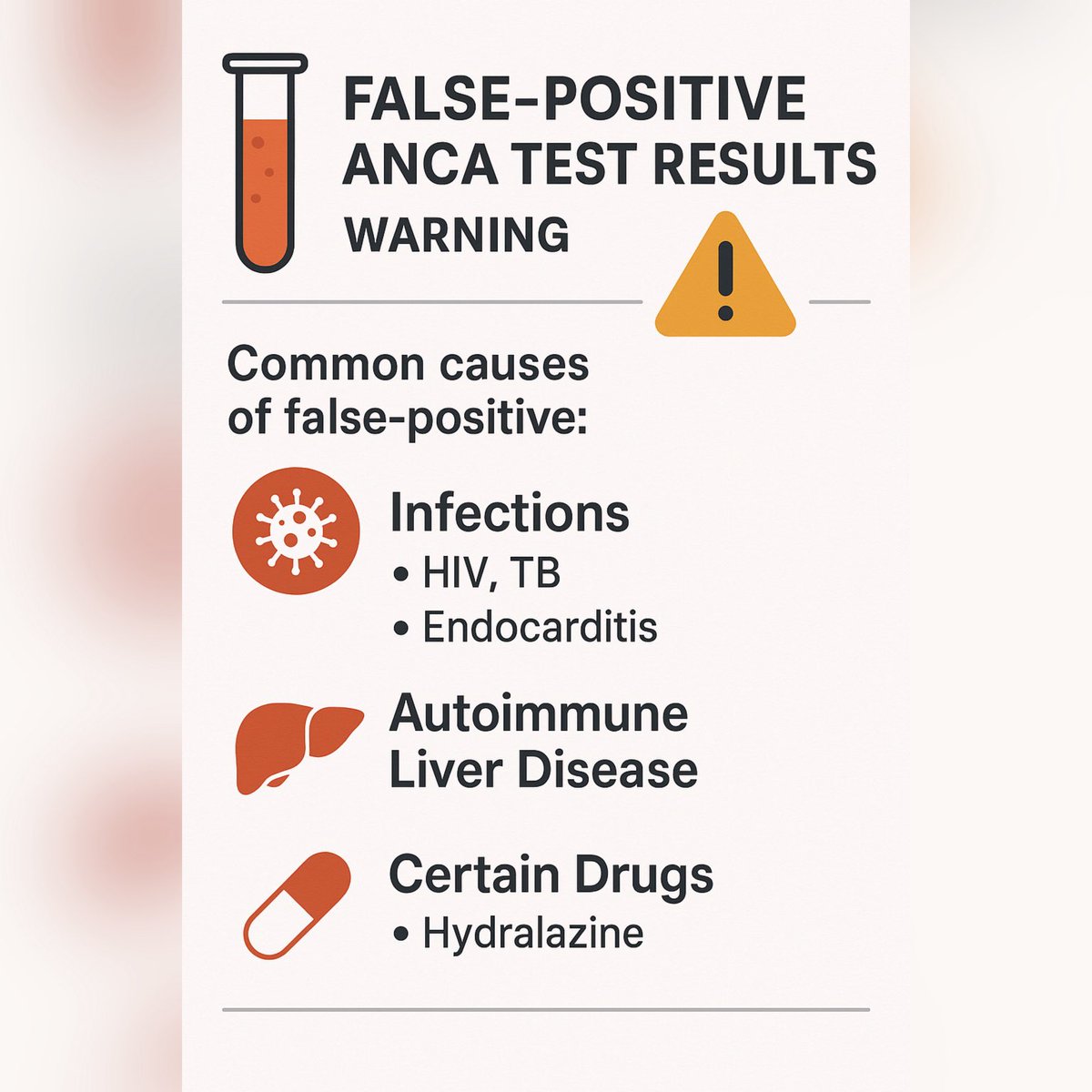
Tweet 5 (Pitfalls):
ANCA ≠ always vasculitis.
•Infections (TB, HIV, endocarditis)
•Autoimmune liver disease
•Drugs: hydralazine, PTU, minocycline
ANCA ≠ always vasculitis.
•Infections (TB, HIV, endocarditis)
•Autoimmune liver disease
•Drugs: hydralazine, PTU, minocycline
Tweet 6 (Clinical pearls):
•ANCA supports but never replaces suspicion.
•Rising titers sometimes predict relapse — but not reliably.
•Tissue biopsy remains the gold standard.
•ANCA supports but never replaces suspicion.
•Rising titers sometimes predict relapse — but not reliably.
•Tissue biopsy remains the gold standard.
Tweet 7 (Take-home):
✅ ANCA is key in vasculitis diagnosis.
❌ False positives are common.
🔑 Always interpret with history, exam, imaging & biopsy.
✅ ANCA is key in vasculitis diagnosis.
❌ False positives are common.
🔑 Always interpret with history, exam, imaging & biopsy.
• • •
Missing some Tweet in this thread? You can try to
force a refresh