Let's say you're a dairy farmer. You have 100 cows. Each year, about 5 cows die, and another 5 cows are born. Then, along comes a virus. Let's call it "cowvid"...
1/
1/
Let's say "cowvid" wipes out about half the cows over the course of a couple years. Now, you're down to 50 cows....
2/
2/
The local mayor declares "cowvid" to be over. This surprises you as a farmer because 5 of your cows keep dying annually. 5 of 50 instead of 5 out of 100. Seems like more, but you're not a city slicker...
3/
3/
The local newspaper puts out dozens of articles about how "cowvid" is over, nobody remembering the international milk and beef industries own the paper.
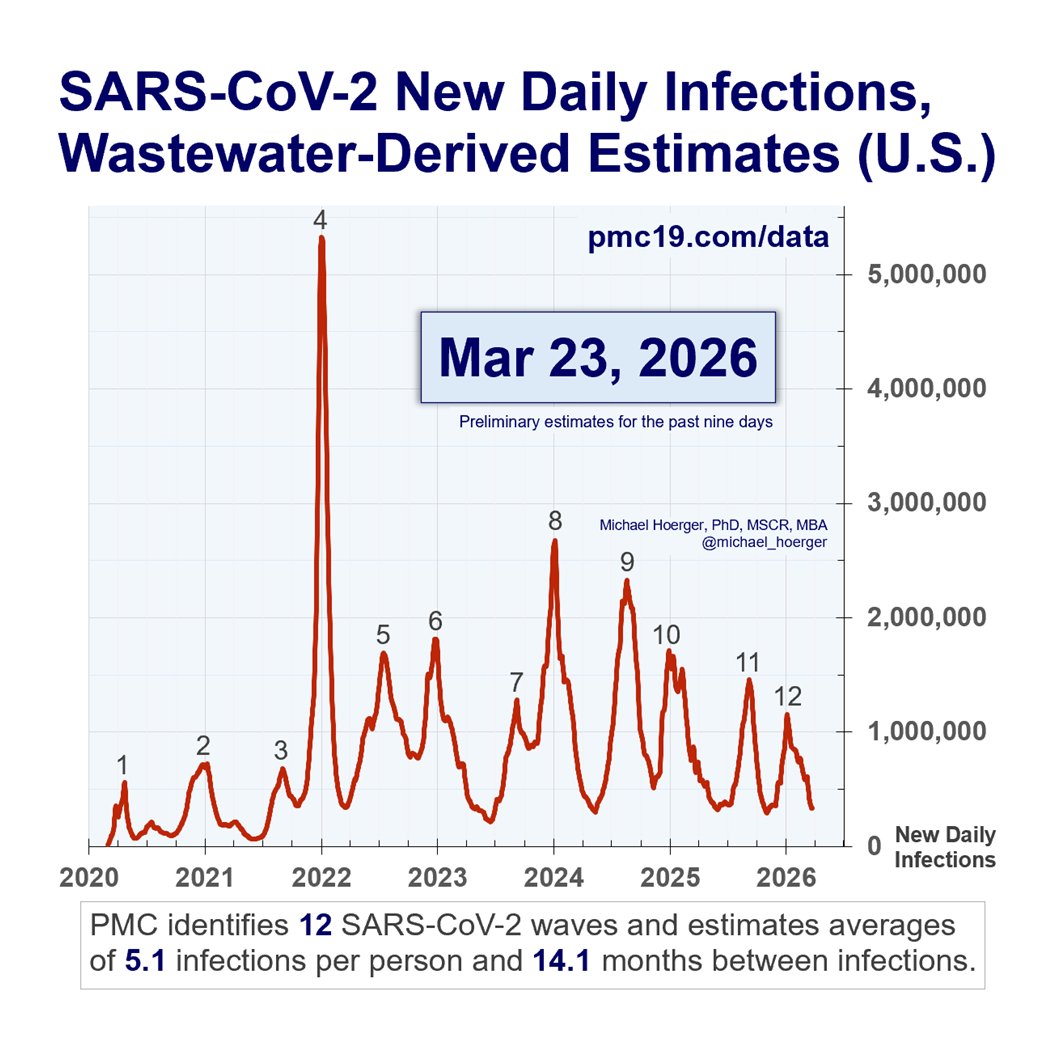
They present very serious graphs showing that local cow deaths have stabilized to pre-cowvid levels...
4/
They present very serious graphs showing that local cow deaths have stabilized to pre-cowvid levels...
4/
Simultaneously, the newspaper puts out articles quoting the town veterinarian stating that while they don't test for "cowvid" anymore, a lot of cows are just dropping dead. Cow heart attacks. Cow cancer. Cow strokes. Sometimes, they just fall over....
5/
5/
In fact, every health problem seems up, except for "cowvid"...
6/
6/
Talking to other dairy farmers, you learn most lost about half their cows to "cowvid" and they're now seeing about as many total deaths as pre-cowvid but among a smaller herd. Weird...
7/
7/
And you begin to wonder, if you all lost half your cows, why would you keep seeing the same number of deaths post-cowvid as pre-cowvid?
8/
8/
In fact, those that made it through the "cowvid" times tended to be your cows that were strongest and healthiest to begin with...
9/
9/
So if you're down from 100 cows to 50, and it's the "strongest" cows that made it, why on earth do you still have 5 cows dying per year just like pre-cowvid? Shouldn't it be 2 or 3?
10/
10/
The main difference between "cowvid" and covid is that we are the cows. Additionally, the mortality was not 50% but below 1%, so rather than being able to see "mortality displacement" with our eyes, it requires excess mortality calculations.
11/
11/
So, remember that when headlines state mortality has returned to pre-pandemic levels. Instead, listen to the multi-billion dollar actuaries whose livelihoods rely on precise estimates and suggest substantial excess mortality will persist a long time.
12/end
12/end
• • •
Missing some Tweet in this thread? You can try to
force a refresh