
In many epidemics and in the COVID-19 pandemic, healthcare workers (HCW) have died or suffered long-term illness. Governments were criticized for not providing PPE. Now the backlash: @UniofOxford @CebmOxford, @cochranecollab and others claim that N95/FFP2 masks are useless. 1/ 

The two most recent Cochrane reviews about physical interventions against respiratory viruses basically claim that face masks do not work, neither in the community nor in the healthcare sector, & that surgical masks are not inferior to N95/FFP2 masks. 2/
cochranelibrary.com/cdsr/doi/10.10…
cochranelibrary.com/cdsr/doi/10.10…
Cochrane reviews are supposed to implement the principles of evidence-based medicine (EBM). Those discussed here do not. They are not the only examples where people with extremely problematic attitudes refer to EBM to justify their actions. We need an investigation. 3/
Initially, Cochrane asked for the abstract to be corrected, to clarify that the absence of evidence for the efficiency of masks and for the superiority of N95/FFP2 masks does not mean that they do not work. The demand for correction has been retracted. 4/
cochrane.org/about-us/news/…
cochrane.org/about-us/news/…
This thread focuses on the question of N95/FFP2 vs surgical mask. In the video below, we see Tom Jefferson, author of these Cochrane reviews, and Carl Heneghan, director of the Oxford University Center for Evidence-Based Medicine, discuss the topic. 5/
At 0:45:00, they claim that the measures taken during the COVID-19 pandemic, like gathering limitations, apps, wearing face masks, and trying to provide HCWs with N95/FFP2 masks, were "ridiculous", caused by "panic and fear", based on "poor evidence". 6/
They refer to a study by Loeb 2022, a randomized controlled trial (RCT) surgical vs N95/FFP2 masks in the COVID-19 pandemic, to support their claim (see below). They also say what should have been done instead: Randomizing UK, US to groups for RCTs. Research, not saving lives. 7/
What is the problem with the Cochrane studies 2020 and 2023? 1) They only take into account RCTs. Not the observational studies, mechanistic (lab) studies, and epidemiologic studies, which show that face masks work and (obs. & mec.) that N95/FFP2 is better than surgical. 8/
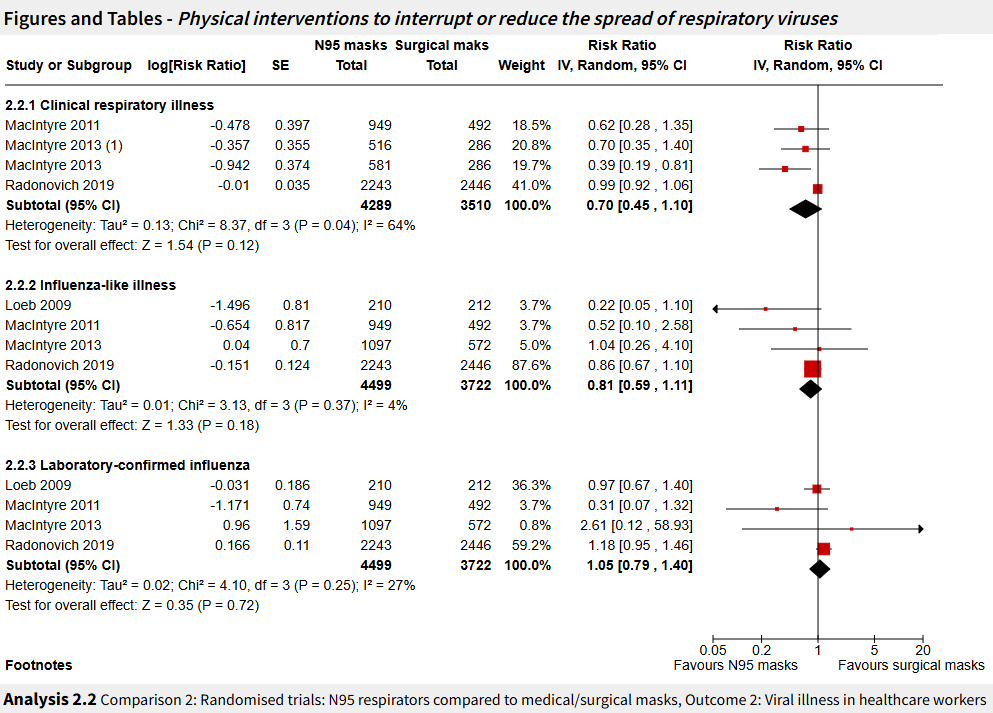
2) In two of the RCTs (Loeb 2009 and Radonovich 2019), the effect is strongly diluted. Loeb: HCW wear N95 or surgical masks when caring for patients with febrile respiratory illness, nothing with other patients, co-workers, outside work. 9/
jamanetwork.com/journals/jama/…
jamanetwork.com/journals/jama/…
Obs. & mech. evidence show that both surgical and N95 masks protect well against respiratory viruses. In an influenza wave, participants can also get infected from pre-symptomatic patients, colleagues, friends, at home, etc. The difference surgical/N95 is strongly diluted. 10/
MacIntyre 2013 is better: participants wear surgical or N95 the whole day. No problem, study conducted in Beijing. 3 groups: surgical, targeted use of N95, all N95. Result: In all outcomes with >10 cases, N95 better than targeted better than surgical. 11/
pubmed.ncbi.nlm.nih.gov/23413265/
pubmed.ncbi.nlm.nih.gov/23413265/
But: For the Cochrane review, cases from studies where the difference surgical vs N95 is strongly diluted are added to cases from well designed studies. One study with strong dilution (Radonovich 2019), but more cases than the other studies, gets the upper hand. 12/
Another issue: What is a surgical mask? According to one study, several surgical masks commonly used in the UK healthcare sector were analyzed regarding filtration efficiency of bioaerosols. Result: Reduction by a factor 1.1 to 55, average 6. 13/
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
How is it that neither the authors (Loeb et al., Radonovich et al.), nor the peer reviewers, nor the Cochrane study authors and reviewers, nor others in the academic community see the problem? Several factors, which must be analyzed through rigorous academic research. 14/
1) Researchers in medical science strictly follow a pattern suitable for drug research. Prescribe a certain drug and see whether it is efficient. Drugs are standardized. No specific skill required to take a pill. Participants want to be cured. Nobody can see they took a pill. 15/
2) The medical community seems to be quite hostile to prevention which does not require the intervention of a doctor. No funding from big Pharma, no income from consultations. Just putting this here, without references. All purely speculative. 16/
3) More worrying: Jefferson (author Cochrane reviews) and Heneghan (director Oxford University Center for Evidence-Based Medicine) have got a blog (behind a paywall, I had to pay Euro 70.- to these people). In one word: QAnon level. Really scary. 17/
trusttheevidence.substack.com
trusttheevidence.substack.com
One example: "Synchronicity of Deaths in the Pandemic", i.e. the fact that COVID-19 mortality peaks in all British counties at the same time in spring 2020. Easy to explain. Measures. But if you deny the efficiency of all measures, →mystery →QAnon. 18/
trusttheevidence.substack.com/p/synchronicit…
trusttheevidence.substack.com/p/synchronicit…
Worse: in the video already mentioned above, Tom Jefferson claims that all Cochrane reviews, incl. pre-pandemic, come "to the same conclusion". This is dishonest. The pre-pandemic reviews conclude that face masks are "the best performing intervention". 19/
doi.org/10.1002/146518…
doi.org/10.1002/146518…
How can @UniofOxford @CebmOxford, @cochranecollab tolerate that people holding such extremist views write highly influential guidelines and the Cochrane reviews which are supposed to implement them? When so many human lives are at stake? And how can we tolerate this? 20/
For an investigation of face masks in the COVID-19 pandemic, from before the pandemic until now, have a look at the following article, by @CK65375 and me. Millions of deaths because in January 2020, WHO suddenly claimed face masks do not work. 21/21
ottokolbl.medium.com/how-face-masks…
ottokolbl.medium.com/how-face-masks…
• • •
Missing some Tweet in this thread? You can try to
force a refresh






