
1/8 Here is some email correspondence obtained via FOIA request between Virologist Vincent Munster at the Rocky Mountain BSL3 lab and Simon Anthony, a virologist who worked under Ian Lipkin at Columbia’s Center for Infection and Immunity, which also doubled as the lab for The ME/CFS Collaborative Research Center. A 🧵:
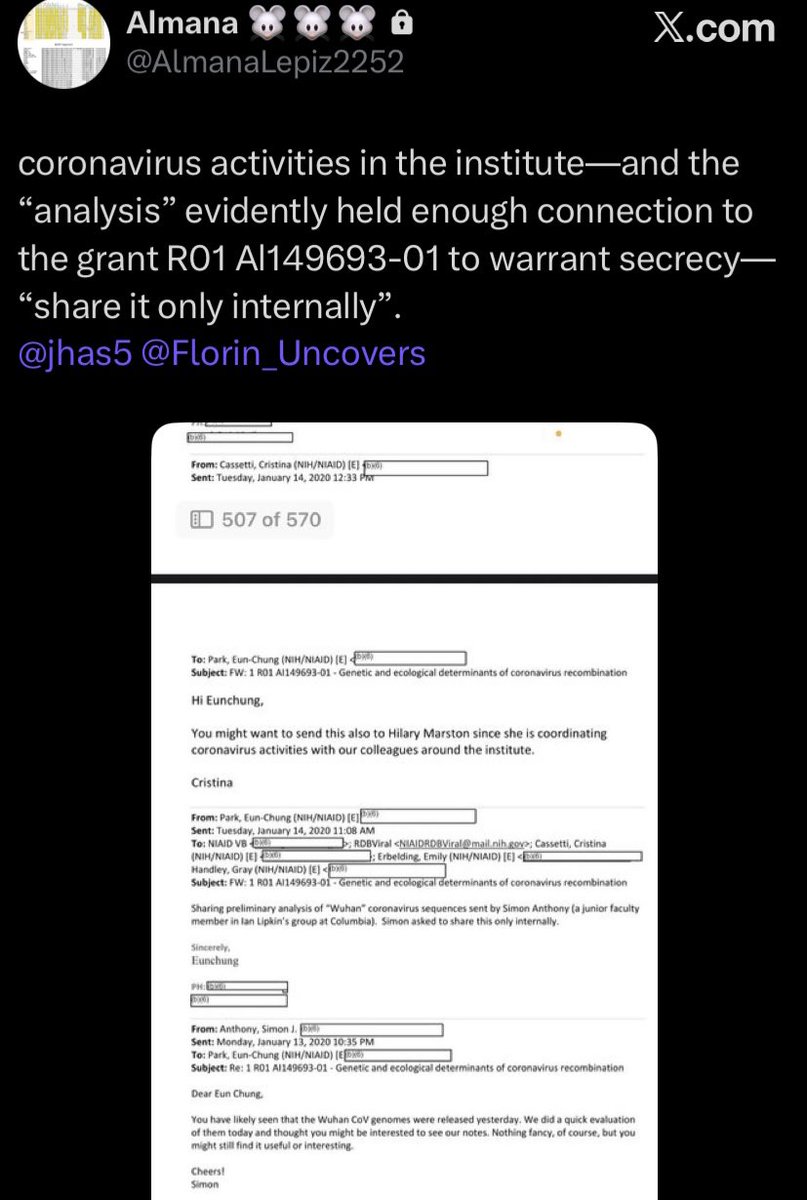
2/8 Here we see the virologists discussing requests to review an attachment on the preliminary analysis of the Wuhan Coronavirus responsible for causing an outbreak of human pneumonia that was originally sent by virologist Simon Anthony who worked under Ian Lipkin at Columbia who sequenced it.
3/8 Here we can see the request Simon Anthony made asking them to only share the document internally. They obviously do not want anyone else seeing this. 👀👀👀
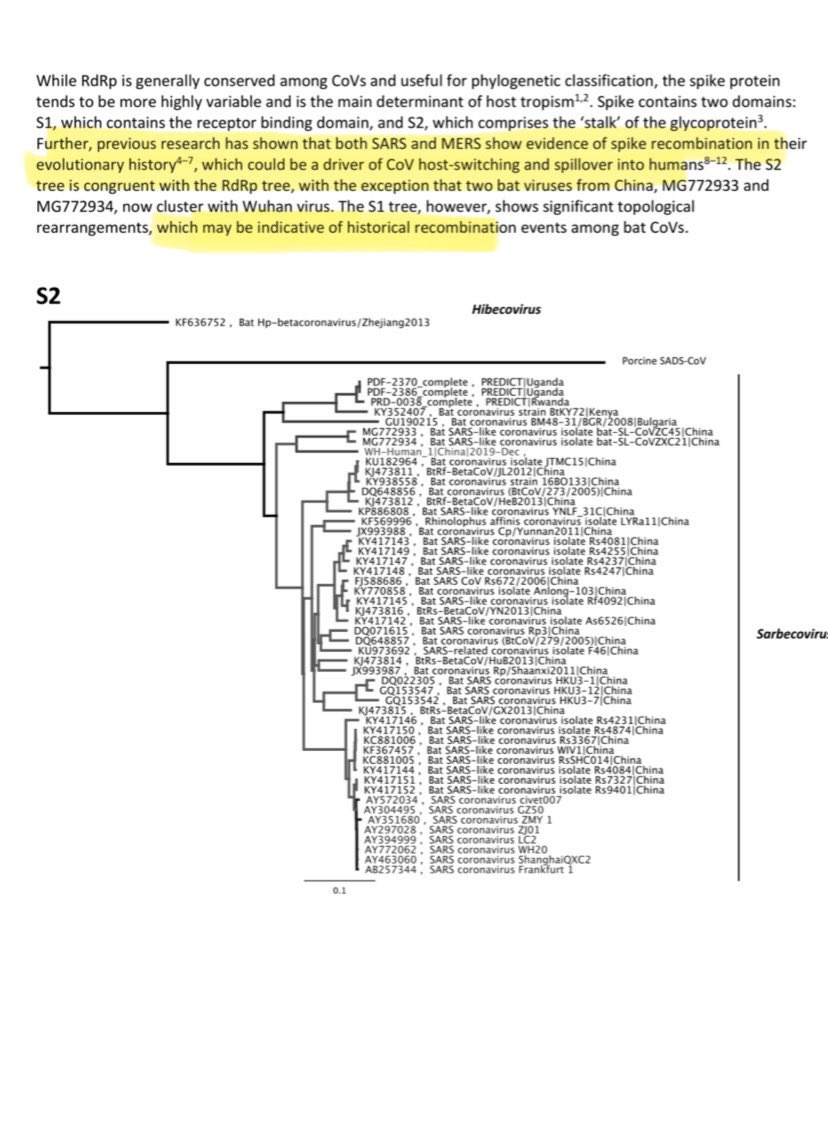
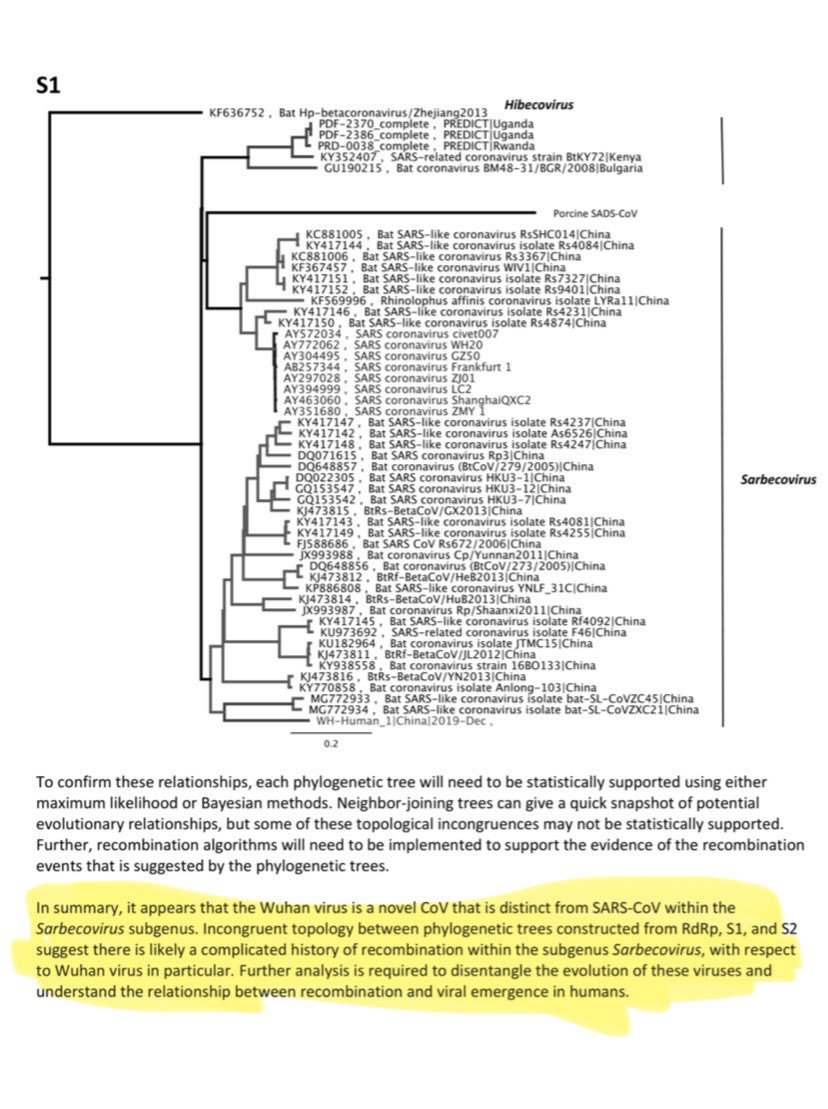
4/8 Simon Anthony states that the virus from Wuhan is very distinct from other human SARS viruses as well as being distinct from other SARS like viruses in China. Simon’s sequencing shows it contains components of human SARS, components of Chinese bat SARS like viruses, as well as evidence of specimens from Africa and Eastern Europe. However Virologists use terms to obfuscate their findings to hide origins of pathogens, so Simon does not directly admit this is what he sees. Instead he uses words like “evidence of historical recombination.”


5/8 Some background information on Simon Anthony. I urge everyone to read between the lines:
Simon Anthony is a virologist who worked with Dr. W. Ian Lipkin at Columbia University's Center for Infection and Immunity (CII). As Lipkin's protégé, he focused on viral discovery and surveillance, with an emphasis on zoonotic diseases—infections that spread from animals to humans.
Expertise in the field and lab: Lipkin praised Anthony as a "brilliant young investigator" with expertise in both field surveillance and laboratory work, a rare combination in the study of pathogen discovery.
Bat viruses: Anthony was a lead researcher on bat-related projects and an authority on the ecology of bat viruses. He co-authored a paper with Lipkin on bats as a major reservoir for hepaciviruses and pegiviruses.
One Health framework: His research advocated for a more systematic, "One Health" approach to studying viruses in wildlife to better understand how viruses emerge as disease-causing pathogens.
PREDICT project: Under Lipkin's guidance at the CII, Anthony was involved with the United States Agency for International Development's PREDICT program, which aimed to identify viral threats before they could spill over into humans.
Later career: After working with Lipkin at Columbia, Anthony moved to the University of California, Davis, where he is now a professor in the Department of Pathology, Microbiology, and Immunology. He also serves as the associate director of the NSF Center for Pandemic Insights.
Simon Anthony is a virologist who worked with Dr. W. Ian Lipkin at Columbia University's Center for Infection and Immunity (CII). As Lipkin's protégé, he focused on viral discovery and surveillance, with an emphasis on zoonotic diseases—infections that spread from animals to humans.
Expertise in the field and lab: Lipkin praised Anthony as a "brilliant young investigator" with expertise in both field surveillance and laboratory work, a rare combination in the study of pathogen discovery.
Bat viruses: Anthony was a lead researcher on bat-related projects and an authority on the ecology of bat viruses. He co-authored a paper with Lipkin on bats as a major reservoir for hepaciviruses and pegiviruses.
One Health framework: His research advocated for a more systematic, "One Health" approach to studying viruses in wildlife to better understand how viruses emerge as disease-causing pathogens.
PREDICT project: Under Lipkin's guidance at the CII, Anthony was involved with the United States Agency for International Development's PREDICT program, which aimed to identify viral threats before they could spill over into humans.
Later career: After working with Lipkin at Columbia, Anthony moved to the University of California, Davis, where he is now a professor in the Department of Pathology, Microbiology, and Immunology. He also serves as the associate director of the NSF Center for Pandemic Insights.
6/8 Here is some background information on virologist Vincent Munster. Once again I ask everyone to read between the lines:
Vincent Munster is a prominent virologist and the Chief of the Virus Ecology Section at the Rocky Mountain Laboratories (RML) in Montana, which is part of the National Institute of Allergy and Infectious Diseases (NIAID). His research focuses on understanding the ecology of emerging viruses and the factors driving zoonotic, or cross-species, transmission. He is a leading expert on high and maximum containment pathogens, including filoviruses (like Ebola), henipaviruses (like Nipah), and coronaviruses.
Key areas of his research
•Virus Ecology and Zoonotic Spillover: Munster leads a Virus Ecology Unit that combines fieldwork with advanced laboratory experiments. His team conducts research at field sites around the world, including Africa, the Caribbean, and the Middle East, to study viruses in their natural reservoirs, such as bats and dromedary camels.
•High-Containment Experimental Work: At the RML, Munster's lab uses high- and maximum-containment facilities (BSL-3 and BSL-4) to safely study highly pathogenic viruses. This allows for detailed research on viral replication, transmission, and pathogenesis in animal models.
•Outbreak Response: Munster has been actively involved in responding to outbreaks of MERS-CoV, Ebola virus, COVID-19, and mpox. During the COVID-19 pandemic, his team worked on developing medical countermeasures and generating experimental data to guide public health decisions.
•Specific Virus Research: His work includes:
◦Studying the transmission of MERS-CoV from dromedary camels to humans.
◦Developing countermeasures against COVID-19 using rhesus macaques and hamster models.
◦Researching viruses in bats, their potential role as reservoirs for pathogens, and their interactions with arthropods
Vincent Munster is a prominent virologist and the Chief of the Virus Ecology Section at the Rocky Mountain Laboratories (RML) in Montana, which is part of the National Institute of Allergy and Infectious Diseases (NIAID). His research focuses on understanding the ecology of emerging viruses and the factors driving zoonotic, or cross-species, transmission. He is a leading expert on high and maximum containment pathogens, including filoviruses (like Ebola), henipaviruses (like Nipah), and coronaviruses.
Key areas of his research
•Virus Ecology and Zoonotic Spillover: Munster leads a Virus Ecology Unit that combines fieldwork with advanced laboratory experiments. His team conducts research at field sites around the world, including Africa, the Caribbean, and the Middle East, to study viruses in their natural reservoirs, such as bats and dromedary camels.
•High-Containment Experimental Work: At the RML, Munster's lab uses high- and maximum-containment facilities (BSL-3 and BSL-4) to safely study highly pathogenic viruses. This allows for detailed research on viral replication, transmission, and pathogenesis in animal models.
•Outbreak Response: Munster has been actively involved in responding to outbreaks of MERS-CoV, Ebola virus, COVID-19, and mpox. During the COVID-19 pandemic, his team worked on developing medical countermeasures and generating experimental data to guide public health decisions.
•Specific Virus Research: His work includes:
◦Studying the transmission of MERS-CoV from dromedary camels to humans.
◦Developing countermeasures against COVID-19 using rhesus macaques and hamster models.
◦Researching viruses in bats, their potential role as reservoirs for pathogens, and their interactions with arthropods
7/8 More on Vincent Munster and his work:
Relation to gain-of-function research
The topic of gain-of-function (GOF) research is closely tied to studies involving dangerous pathogens, and Vincent Munster's lab has been part of this public debate.
Defining Gain-of-Function
Broad definition: Broadly, GOF refers to research that alters an organism, such as a virus, to give it new properties or functions. Most GOF research is mundane, with positive applications like creating vaccines or improving crops.
Specific, controversial definition: In the context of pandemic pathogens, GOF has a narrower meaning, referring to experiments that could enhance a pathogen's ability to spread more easily or cause more severe disease in humans. This is known as "Gain-of-Function Research of Concern" (GOFROC) or "Enhanced Potential Pandemic Pathogen" (ePPP) research.
The debate and Munster's work
Risk vs. benefit: The central debate surrounding GOFROC involves weighing the potential benefits against the risks. Proponents argue that it's necessary to understand potential threats and develop countermeasures, while opponents express concern about the risk of accidental lab release.
RML and the COVID-19 pandemic: Following the COVID-19 pandemic, some US policymakers raised concerns about the research conducted at the RML and attempted to defund it. The RML's work on coronaviruses in the years prior to the pandemic was a point of public discussion, and some media reports implied a direct link to the pandemic's origin.
Relation to gain-of-function research
The topic of gain-of-function (GOF) research is closely tied to studies involving dangerous pathogens, and Vincent Munster's lab has been part of this public debate.
Defining Gain-of-Function
Broad definition: Broadly, GOF refers to research that alters an organism, such as a virus, to give it new properties or functions. Most GOF research is mundane, with positive applications like creating vaccines or improving crops.
Specific, controversial definition: In the context of pandemic pathogens, GOF has a narrower meaning, referring to experiments that could enhance a pathogen's ability to spread more easily or cause more severe disease in humans. This is known as "Gain-of-Function Research of Concern" (GOFROC) or "Enhanced Potential Pandemic Pathogen" (ePPP) research.
The debate and Munster's work
Risk vs. benefit: The central debate surrounding GOFROC involves weighing the potential benefits against the risks. Proponents argue that it's necessary to understand potential threats and develop countermeasures, while opponents express concern about the risk of accidental lab release.
RML and the COVID-19 pandemic: Following the COVID-19 pandemic, some US policymakers raised concerns about the research conducted at the RML and attempted to defund it. The RML's work on coronaviruses in the years prior to the pandemic was a point of public discussion, and some media reports implied a direct link to the pandemic's origin.
8/8 This is why the correspondence between Vincent Munster with the NIAID and Simon Anthony at Columbia matters.
Both Lipkin's team (which included Anthony) and researchers at NIAID (like Munster) were key players in the PREDICT consortium. These large, multi-institutional projects required the kind of collaboration seen between their respective labs.
The PREDICT program, funded by the United States Agency for International Development (USAID), was a global initiative focused on identifying viral threats in wildlife before they could cause a pandemic.
“Supposedly.” 😒
Both Lipkin's team (which included Anthony) and researchers at NIAID (like Munster) were key players in the PREDICT consortium. These large, multi-institutional projects required the kind of collaboration seen between their respective labs.
The PREDICT program, funded by the United States Agency for International Development (USAID), was a global initiative focused on identifying viral threats in wildlife before they could cause a pandemic.
“Supposedly.” 😒
Supplemental: 😒
https://x.com/almanalepiz2252/status/1969764798918500621?s=46&t=wRQSWp_1VffWmS2vKQwhSA
Supplemental:
Per Chrome’s Gemini Neo AI:
“While the number of potential viruses in animals is massive, estimated to be between 260,000 and 1.6 million, only a tiny fraction (far less than 0.1%) have ever caused a known human infection.” 😒
Per Chrome’s Gemini Neo AI:
“While the number of potential viruses in animals is massive, estimated to be between 260,000 and 1.6 million, only a tiny fraction (far less than 0.1%) have ever caused a known human infection.” 😒
Supplemental:
https://x.com/jhas5/status/1953588074497376324?s=46
Supplemental: This is a previous thread and link to a previous FOIA request on the Rocky Mountain Lab.
https://twitter.com/CD57227/status/1754947809705394293
Supplemental: from previous FOIA as well.
https://twitter.com/Rebecca21951651/status/1841646310421676511
X has blurred out legally obtained documents. They were fine and now they are not. That is obfuscation. Here is what Simon said in his analysis on part 4/8 of this thread.
https://twitter.com/missyTHX1138/status/1969904881885393402

@KevinMcCairnPhD
• • •
Missing some Tweet in this thread? You can try to
force a refresh



